Surgery, Gastroenterology and Oncology

|
|
Pancreatic glucagonoma is a well-known rare subtype of pancreatic neuroendocrine tumors (PNETs). Most cases of pancreatic glucagonoma are associated with symptoms such as skin rash and necrotizing migratory erythema; however, some cases are asymptomatic. Complete tumor resection has an important impact on the long-term prognosis of patients with primary PNETs. The 2019 edition of the Japanese Guidelines for Neuroendocrine Tumors recommends recurrent lesions of pancreatic and gastrointestinal NETs to be treated multimodally, including resection if the lesions are curatively resectable. However, no treatment strategy has been established for recurrent pancreatic glucagonoma. We report the case of a patient who underwent distal pancreatectomy for primary pancreatic glucagonoma and developed multiple hepatic metastatic recurrences five years after the primary surgery. After two and a half years of somatostatin analog (SSA) treatment, neither tumor growth nor extrahepatic recurrence was detected, and curative surgery was performed. This study reports a rare case of complete resection for multiple metachronous liver metastases from a pancreatic glucagonoma after curative surgery. During SSA therapy, the metastatic tumors showed a very slow growth pattern. No other distant extrahepatic metastases emerged. Curative hepatectomy was performed safely, and the postoperative course was uneventful.
INTRODUCTION
Pancreatic glucagonomas are rare pancreatic neuroendocrine tumors (PNETs), with an incidence of approximately 2.6/100 million people in Japan (1). In most cases, symptomatic pancreatic glucagonoma, a subtype of PNET, is diagnosed based on the chief complaints of skin rash, necrotizing migratory erythema (NME), and weight loss. The incidence rates of typical clinical findings are as follows: NME, 82.4%; diabetes, 68.5%; weight loss, 60.2%; anemia, 49.6%; and glossitis, stomatitis, or cheilitis, 41.2% (2). Surgery is the only curative treatment for this disease.
Somatostatin analogs (SSA) and amino acid solution can be administered to relieve the symptoms; however, this treatment can only be used in patients with advanced disease. The number of reports on PNET treatment has increased in recent years (3,4). The rarity of this disease has hindered the discovery of therapeutic options, including drugs or surgical treatments for the recurrence of pancreatic glucagonoma. According to the 2019 edition of the Japanese Guidelines for Neuroendocrine Tumors, aggressive surgery for recurrent neuroendocrine tumors (NETs) is recommended to prolong overall survival (OS) and disease-free survival under the strict patient selection (5).
Here, we report the case of a patient who underwent distal pancreatectomy for primary pancreatic glucagonoma and developed multiple hepatic metastatic recurrences five years after the primary surgery. After two and a half years of SSA treatment, neither tumor growth nor extrahepatic recurrence was detected, and curative hepatectomy was performed. Thus, we report a rare case of conversion surgery for multiple metachronous liver metastases from a pancreatic glucagonoma after curative surgery.
CASE REPORT
The patient was a 57-year-old male who was found to have an incidental tumor in the pancreatic tail, detected on enhanced computed tomography (CT) during an annual follow-up of a renal cyst
(fig. 1).
 The tumor was strongly enhanced in the early phase, and the enhancement was prolonged in the delayed phase. The maximum diameter of the tumor was 28 mm. On magnetic resonance imaging (MRI), the tumor margin was well-demarcated, with a low signal on T1-weighted images, a bright high signal on T2-weighted images, and a small high signal area of suspected internal necrosis. Diffusion-weighted MRI showed a high tumor signal intensity (fig. 2). Positron emission tomography showed that the tumor had high fluorine-18-deoxyglucose accumulation, with a maximum standardized uptake value of up to 8.8 (fig. 3). Serum gastrointestinal hormone testing revealed a slight elevation in serum glucagon, whereas other gastrointestinal hormones such as gastrin, insulin, vasoactive intestinal peptide, and serotonin were within normal ranges.
The tumor was strongly enhanced in the early phase, and the enhancement was prolonged in the delayed phase. The maximum diameter of the tumor was 28 mm. On magnetic resonance imaging (MRI), the tumor margin was well-demarcated, with a low signal on T1-weighted images, a bright high signal on T2-weighted images, and a small high signal area of suspected internal necrosis. Diffusion-weighted MRI showed a high tumor signal intensity (fig. 2). Positron emission tomography showed that the tumor had high fluorine-18-deoxyglucose accumulation, with a maximum standardized uptake value of up to 8.8 (fig. 3). Serum gastrointestinal hormone testing revealed a slight elevation in serum glucagon, whereas other gastrointestinal hormones such as gastrin, insulin, vasoactive intestinal peptide, and serotonin were within normal ranges.
Figure 1 - On CT, the tumor was located at the pancreatic tail. This tumor was strongly enhanced at the early phase.

Figure 2 - On MRI, the tumor presented a slightly high signal on T2-weighted images, and a high signal intensity on diffusion-weighted images.
Figure 3 - Positron emission tomography showed that the tumor had a high fluorine-18-deoxyglucose accumulation.

The patient was suspected of having a primary pancreatic glucagonoma; thus, distal pancreatectomy and lymph node dissection were performed. The operative time and intraoperative bleeding volume were 114 min and 25 mL, respectively.
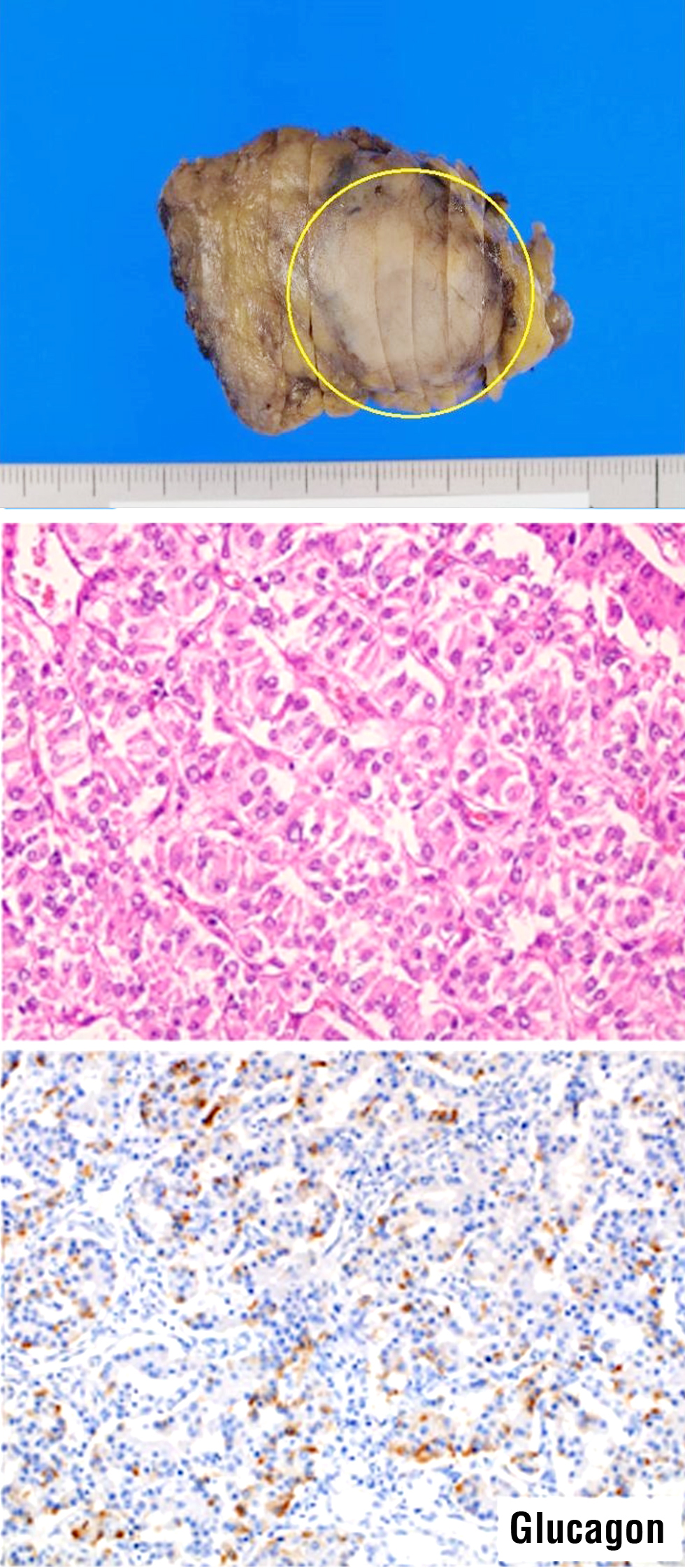
After pathological examination, the final diagnosis was a grade 2 PNET (Ki-67, 3%). Immunohistochemical analysis revealed that the tumor was glucagon-positive (fig. 4).
Figure 4 - Cylindrical tumor cells positive for chromogranin A and synaptophysin were arranged in a cord-like pattern. Immunostaining was positive for glucagon, and pancreatic glucagonoma was diagnosed.
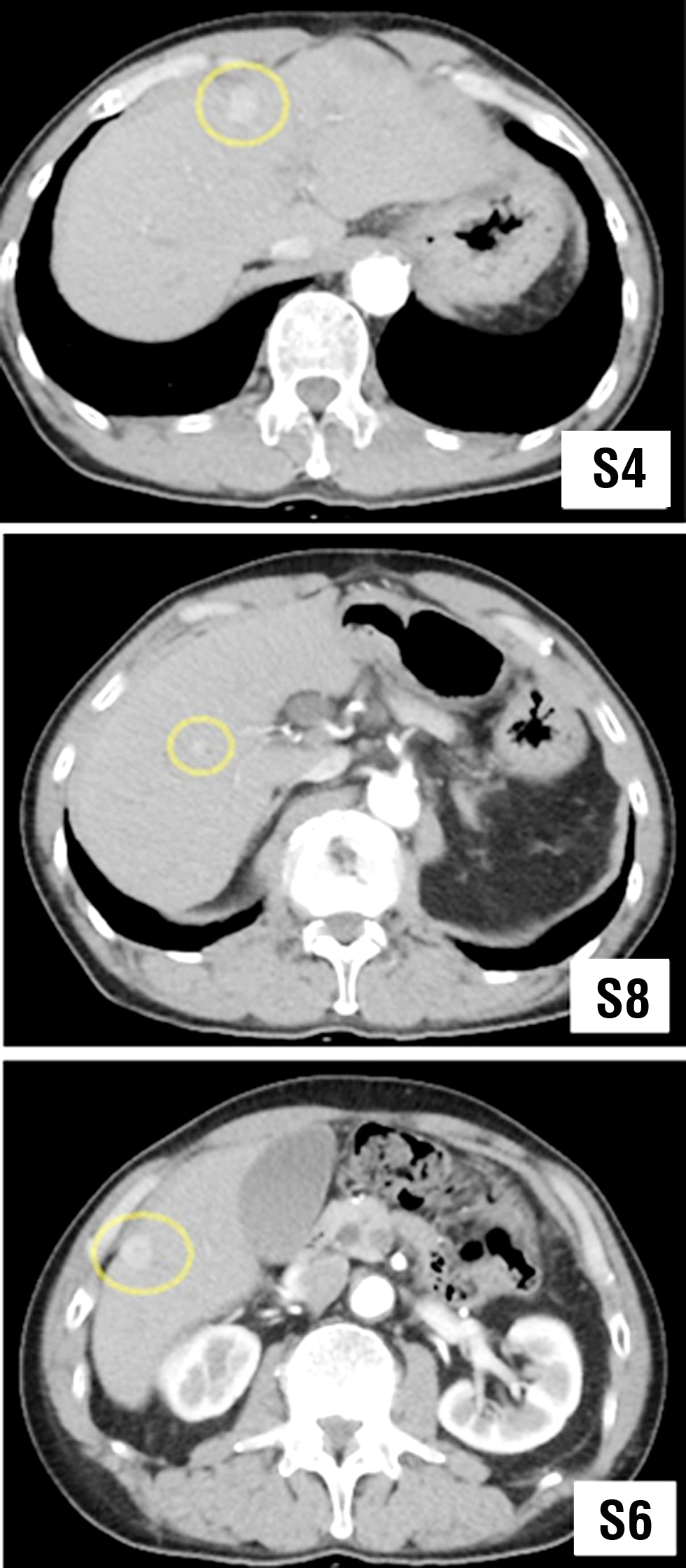
Five years after surgery, the patient developed a metastatic tumor at each of the liver segments (S) 4, 7, and 8, with a maximal size of 10 × 10 mm. Radiological examination revealed that all tumors were typical metastatic NETs (fig. 5). Considering the sudden multiple recurrence pattern, the patient was administered pharmacological therapy with SSA, with no upfront surgery to confirm the tumor response. During the SSA treatment, tumor growth was remarkably slow. Except for one new small metastatic lesion in S6, neither extrahepatic metastasis nor massive growth of the liver metastatic tumors was detected (fig. 6). Liver function was well preserved as Child-Pugh grade A, liver damage A.
Figure 5 - CT demonstrated tumors in liver S4 and S8, strongly contrasted in the early phase and faintly contrasted in the late phase, suggesting the possibility of liver metastasis of NET.
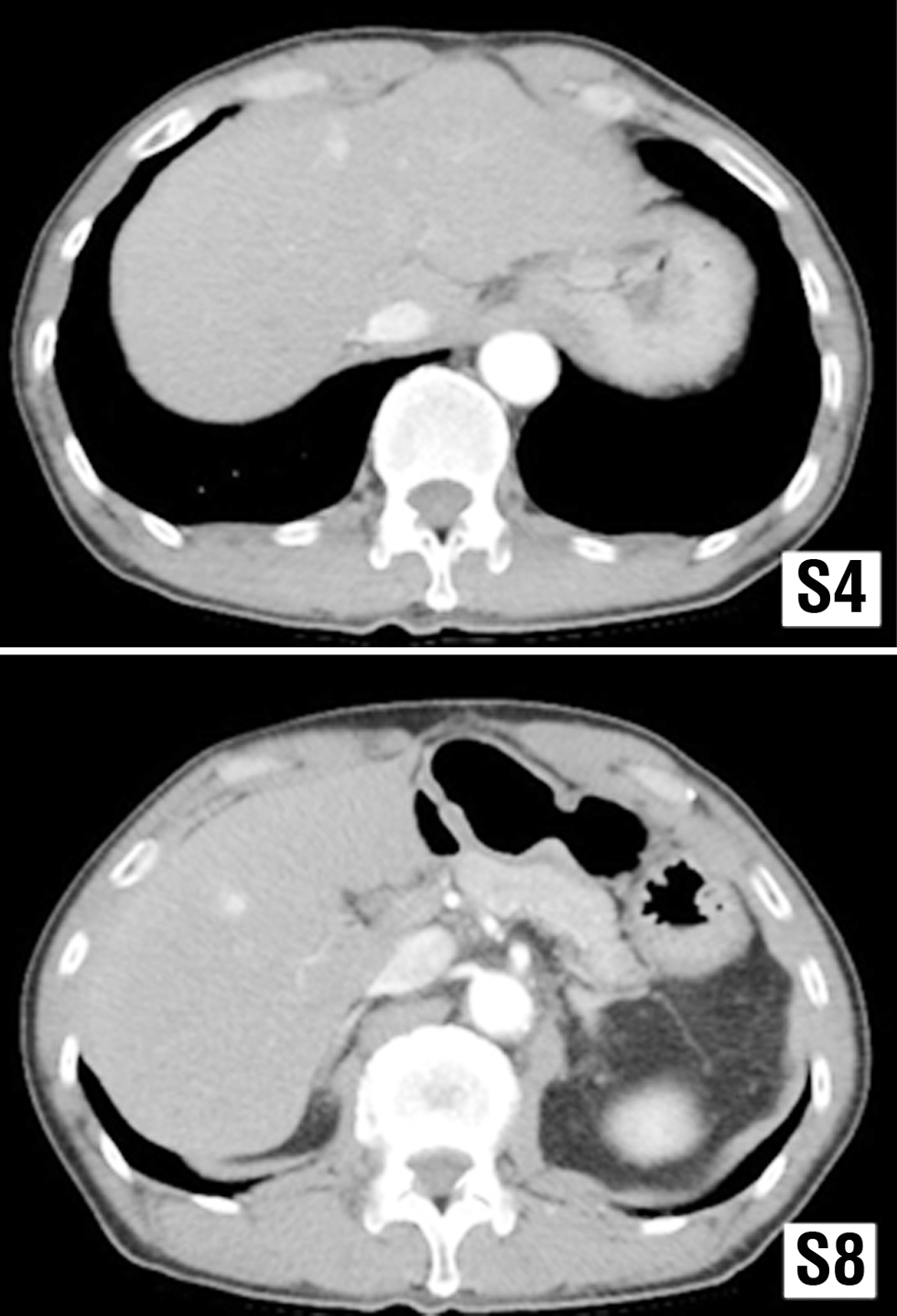
Figure 6 - CT showed tumor recurrence in the S6 of the liver. This tumor was strongly enhanced in the early phase.
Curative surgery consisting of S4, S7, and S8 partial hepatectomy with S6 subsegmentectomy was
performed after two and a half years of SSA treatment (fig. 7). The patient was discharged without complications. Analysis of the specimens revealed that all tumors were metastases of pancreatic glucagonoma (grade 2 PNET; Ki-67, 3.5%).
Figure 7 - An intrahepatic mass was observed, and histology revealed foci of tumor cells with eosinophilic cytoplasm and uniform nuclei, which were found to be metastases of glucagonoma.

After radical surgery, the patient was followed without medication. No tumor recurrence was observed one year after hepatectomy for liver metastasis.
DISCUSSIONS
We present the case of a 57-year-old male with hepatic metastases five years after distal pancreatectomy for pancreatic glucagonoma. During a 2.5-year SSA therapy period, the metastatic tumors progressed very slowly. No new distant extrahepatic metastases emerged. A curative hepatectomy was performed safely, and the postoperative course was uneventful.
Glucagonoma is a rare hormonally active NET that causes excess glucagon secretion, with an incidence of 1 in 20 million people worldwide (6). Pancreatic glucagonoma accounts for only 2–7% of PNETs. The most frequent site of this tumor is not the pancreatic head but the body and tail of the pancreas (7). The symptoms that emerge in symptomatic (functional) PNETs are key to the diagnosis of this disease. However, asymptomatic (nonfunctional) glucagonomas account for 26.7% of all cases (7), and early diagnosis of asymptomatic cases is generally difficult. In addition, because the initial symptoms of glucagonoma syndrome are often subtle and nonspecific, the diagnosis is typically made when metastases in the liver, regional, or cervical lymph nodes (8), bones, or lungs (9) have already developed.
Although our patient was asymptomatic, the tumor was discovered incidentally on a CT scan; thus, the patient underwent tumor resection surgery, which allowed us to diagnose the disease at an early stage. Patients with pancreatic glucagonomas often achieve prolonged survival with multidisciplinary treatment, even in the presence of distant metastases (10)—up to 21 years in one published case (11). Two approved SSAs (lanreotide and octreotide) are recommended for the initial treatment of functional pancreatic neuro-endocrine neoplasms, except for carcinoid syndromes, gastrinomas, insulinomas, and adreno-corticotropinomas (12). With the use of SSAs, the rashes and NME can be controlled in 50–90% of cases, and glucagonoma syndromes, such as weight loss, abdominal pain, and diarrhea, usually improve (12). One study also measured tumor size before and during treatment to determine whether SSA affected tumor growth and found that tumors stabilized in 14 patients and increased only in the remaining two (13). Although it is difficult to determine whether the stability of tumor size in most patients is directly related to the administration of SSAs, this association cannot be completely ruled out.
In the present case, the patient had recurrent liver metastases after radical surgery, but SSA enabled stable control of the tumor size for more than two years. A previous study has suggested that in patients with PNETs and unresectable liver metastases, primary tumor resection is associated with improved survival (14). Further, preoperative or postoperative radical and debulking procedures are considered important for the long-term prognosis of PNETs (15).
An established treatment strategy for pancreatic glucagonoma recurrence remains controversial. Aggressive resection is considered beneficial when technically feasible (16). No evidence exists for hepatic resection of glucagonomas with liver metastases. However, liver resection has been found to improve cancer-specific survival (CSS) and OS in patients with PNETs with simultaneous hepatic metastases. In a previous study, 1-year CSS rates were 95.5% and 74%, and 3-year OS rates were 95.5% and 48.5% in surgery and non-surgery groups, respectively (17).
Currently, no strict criteria exist for the optimal timing from drug therapy to surgery for liver metastases after surgery of the primary glucagonoma. Moreover, while resection without residuals on imaging may have an impact on prognosis, it is important to confirm long-term prognosis after hepatic resection. Taking advantage of our multidisciplinary expertise, we decided on surgery based on the absence of distant metastases outside of the liver following long-term chemotherapy. To date, the patient has had no recurrence, but further long-term follow-up is needed.
CONCLUSIONS
Multidisciplinary treatment using both pharmaco-therapy and surgery for pancreatic glucagonoma is important to achieve a long-term favorable prognosis. Curative surgery may be considered for patients with recurrent liver metastases from PNETs.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest and Source of Funding
There is no conflict of interest in this study.
REFERENCES
1.Ito T, Sasano H, Tanaka M, Osamura RY, Sasaki I, Kimura W, et al. Epidemiological study of gastroenteropancreatic neuroendocrine tumors in Japan. J Gastroenterol. 2010;45(2):234-43.
2. Song X, Zheng S, Yang G, Xiong G, Cao Z, Feng M, et al. Glucagonoma and the glucagonoma syndrome. Oncol Lett. 2018;15(3):2749-55.
3. Cao X, Wang X, Lu Y, Zhao B, Shi J, Guan Q, et al. Spleen-preserving distal pancreatectomy and lymphadenectomy for glucagonoma syndrome: A case report. Medicine (Baltimore) 2019; 98(38):e17037.
4. Watt DG, Pandanaboyana S, Herrington CS, Tait IS. Pancreatic glucagonoma metastasising to the right ovary five years after initial surgery: a case report. JOP. 2013;14(5):510-4.
5. Schurr PG, Strate T, Rese K, Kaifi JT, Reichelt U, Petri S, et al. Aggressive surgery improves long-term survival in neuroendocrine pancreatic tumors: an institutional experience. Ann Surg. 2007; 245(2):273-81.
6. Al-Faouri A, Ajarma K, Alghazawi S, Al-Rawabdeh S, Zayadeen A. Glucagonoma and Glucagonoma Syndrome: A Case Report with Review of Recent Advances in Management. Case Rep Surg. 2016; 2016:1484089.
7. Nishiya K, Nishimura M, Iwata T, Urushibara T, Yokoyama K. A case of asymptomatic glucagonoma of the pancreas: A review of the reported case of pancreatic glucagonoma 2.0cm or less in diameter in Japan. Suizo. 2005;20:407-13. Japanese
8. Butte JM, Montero PH, Solar A, Torres J, Olmos PR, Goñi I, et al. Cervical metastases of glucagonoma in a patient with multiple endocrine neoplasia type 1: report of a case. Surg Today. 2008; 38(12):1137-43.
9. Pinto Marín A, Hernández Agudo E, Feliú J, González Barón M. Pancreatic glucagonoma presenting as a pulmonary mass. Clin Transl Oncol. 2009;11(1):60-2.
10. Chu QD, Al-kasspooles MF, Smith JL, Nava HR, Douglass HO, Jr., Driscoll D, et al. Is glucagonoma of the pancreas a curable disease? Int J Pancreatol. 2001;29(3):155-62.
11. Dourakis SP, Alexopoulou A, Georgousi KK, Archimandritis AJ, Delladetsima JK, Tolis G. Glucagonoma Syndrome: Survival 21 Years With Concurrent Liver Metastases. Am J Med Sci. 2007; 334(3):225-7.
12. Ito T, Igarashi H, Jensen RT. Pancreatic neuroendocrine tumors: clinical features, diagnosis and medical treatment: advances. Best Pract Res Clin Gastroenterol. 2012;26(6):737-53.
13. Tomassetti P, Migliori M, Corinaldesi R, Gullo L. Treatment of gastroenteropancreatic neuroendocrine tumours with octreotide LAR. Aliment Pharmacol Ther. 2000;14(5):557-60.
14. Bertani E, Fazio N, Botteri E, Chiappa A, Falconi M, Grana C, et al. Resection of the primary pancreatic neuroendocrine tumor in patients with unresectable liver metastases: possible indications for a multimodal approach. Surgery. 2014;155(4):607-14.
15. Sarmiento JM, Que FG, Grant CS, Thompson GB, Farnell MB, Nagorney DM. Concurrent resections of pancreatic islet cell cancers with synchronous hepatic metastases: outcomes of an aggressive approach. Surgery. 2002;132(6):976-82; discussion 982-3.
16. Aoki T, Kubota K, Kiritani S, Arita J, Morizane C, Masui T, et al. Survey of surgical resections for neuroendocrine liver metastases: A project study of the Japan Neuroendocrine Tumor Society (JNETS). J Hepatobiliary Pancreat Sci 2021;28(6):489-97.
17. Lianyuan Tao DX, Abuduhaibaier Sadula, Chen Ye, Qing Chen, Hanyan Wang, Zhipeng Zhang, Lingfu Zhang, Ming Tao, Chunhui Yuan. Surgical resection of primary tumor improves survival of pancreatic neuroendocrine tumor with liver metastases. Oncotarget. 2017;8(45):79785-92.
Full Text Sources:
Abstract:
Views: 2878

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.