Surgery, Gastroenterology and Oncology

|
|
Introduction: Neuroendocrine neoplasms (NENs) originate from neuroendocrine cells
diffusing throughout the body. They are a heterogeneous group of tumors with neuro-endocrine function and malignant potential. They manifest themselves in various and
complex clinical manifestation and localization, mostly affecting the GIT(gastrointestinal tract), the pancreas (GEP) and the bronchopulmonary system. The incidence of colon and rectum NEN (r-NEN) tumors has increased significantly over the last decade, partly as a result of improved diagnostic methods. Most commonly they are highly differentiated tumors with small size and good prognosis. Most of them are non-functioning and the diagnosis is made in advanced stages when the patients develop clinical symptoms from the GIT-anemia, hematochezia, obsruction. The rectal NENs represent 1-2% of all rectal tumors.
Methods: We report a retrospective cohort single center study of patients diagnosed with NENs who underwent surgical interventions in our department between 2010-2022.
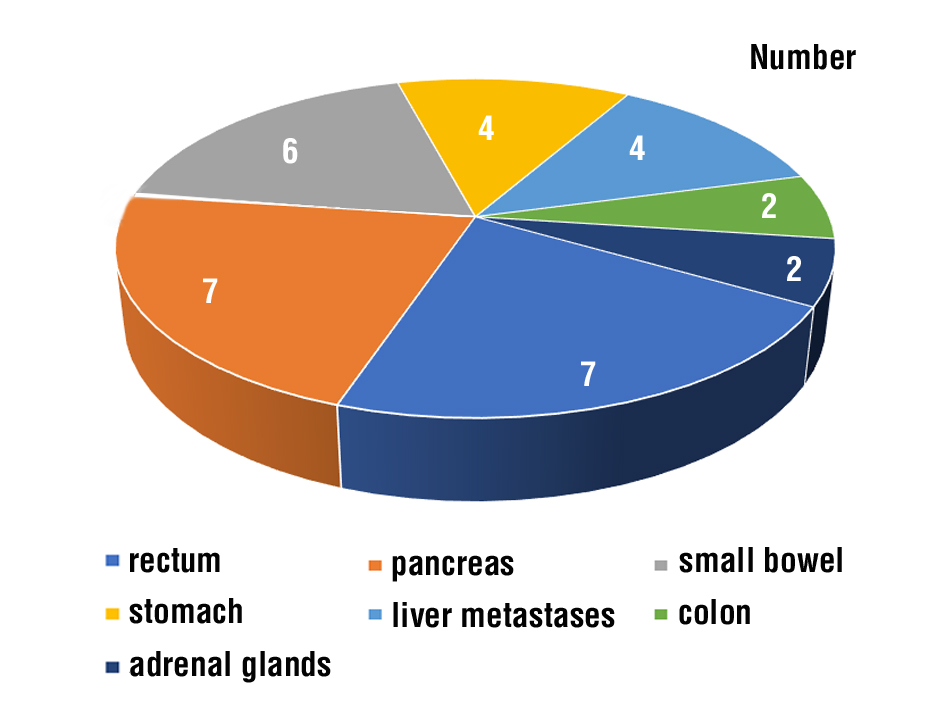
Results: 32 patients (19 women and 13 men) participated in the study. The locations of the neuroendocrine tumors were: colon and rectum - 9 patients, small intestine - 6 patients, stomach - 4 patients, pancreas - 7 patients, adrenal glands - 2 patients, liver metastases - 4 patients. The histological type was: neuroendocrine tumor – 27, Insulinoma – 3, pheochromocytoma – 2.
Conclusions: R- NENs and small bowel NENs are the most frequent NENs of the digestive system. Their incidence has hugely increased due to widespread use of endoscopic screening for colorectal cancer. Highly differentiated rectal tumors (< 2 cm) are indicated for endoscopic resection. Tumors larger than 2 cm are suggested for surgical resection with higher risk for distant metastases. The best results in the treatment of NETs are achieved in highly specialized centers, with the participation of endoscopists and surgeons.
INTRODUCTION
Neuroendocrine tumors (NETs) or neuroendocrine neoplasms (NENs) are a heterogeneous group of tumors with neuroendocrine function and malignant potential. The first description of a neuroendocrine tumor was in 1867 when Theodor Langhans described a polyp of the small intestine that appeared poorly differentiated on histology but without evidence of invasion (1). In 1907 Oberdorfner described these tumors of the small intestine that appeared histologically malignant but acted clinically benign (2).
In 1963, Williams and Sandler broadened the term carcinoid to include other functional tumors with similar clinical and biochemical findings and categorized carcinoid tumors by embryologic origin. The foregut carcinoid tumors include those arising from the bronchus, stomach, pancreas, and proximal to the mid-duodenum. Midgut carcinoids arise in the mid-duodenum, jejunum, ileum, and mid-transverse colon. Hindgut carcinoids arise from the descending colon and rectum (3-5). NENs develop slowly and asymptomatically or with nonspecific symptoms, which are determined by the localization of the tumor process and could be: abdominal pain, obstruction, nausea, vomiting, bleeding, jaundice.
Capella et al. recommended replacing the term “carcinoid” with “neuroendocrine tumor” to describe tumors originating from neuroendocrine cells which exist at the neuronal and endocrine interface and are defined by their secretory products (6).
The term neuroendocrine neoplasm includes well-differentiated NETs and poorly-differentiated neuro-endocrine carcinomas (NECs)(7).
METHODS
Thirty-two patients with NENs were admitted in Second Department of Surgery between 2010-2022 presented with abdominal pain, ileus, jaundice and hematochesia. All patients signed an inform consent approved by our hospital. After imaging procedures: ultrasound, X-ray, and CT scan and fibrocolonoscopy the patients were operated. The specimens were sent for pathomorphological and immunohistochemical examination by protocol. Diagnosis was established after the histological results.
Figure 1 - Location of the NEN in the abdominal cavity
Statistical analisys
Microsoft Excel 2019 and SPSS (Statistical Package for Social Science) v16.0 software products were applied in connection with data processing. The level of significance was set at < 0.05.
RESULTS
The patients with rNEN will be considered and compared with other patients with NEN.
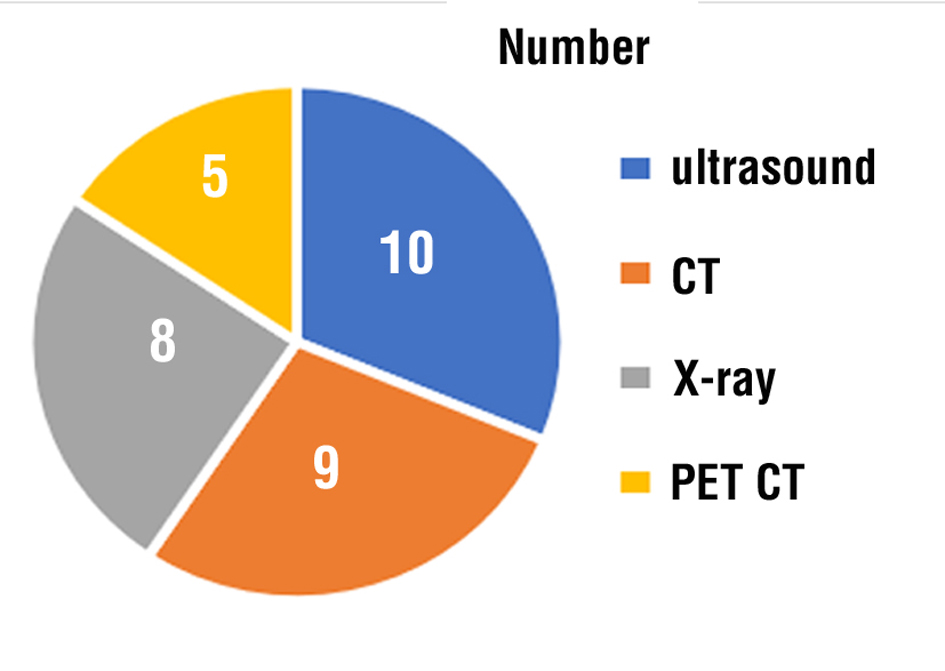
Imaging procedures were performed to all of the patients with NEN shown on figs. 1, 2.
Figure 2 - Imaging procedures
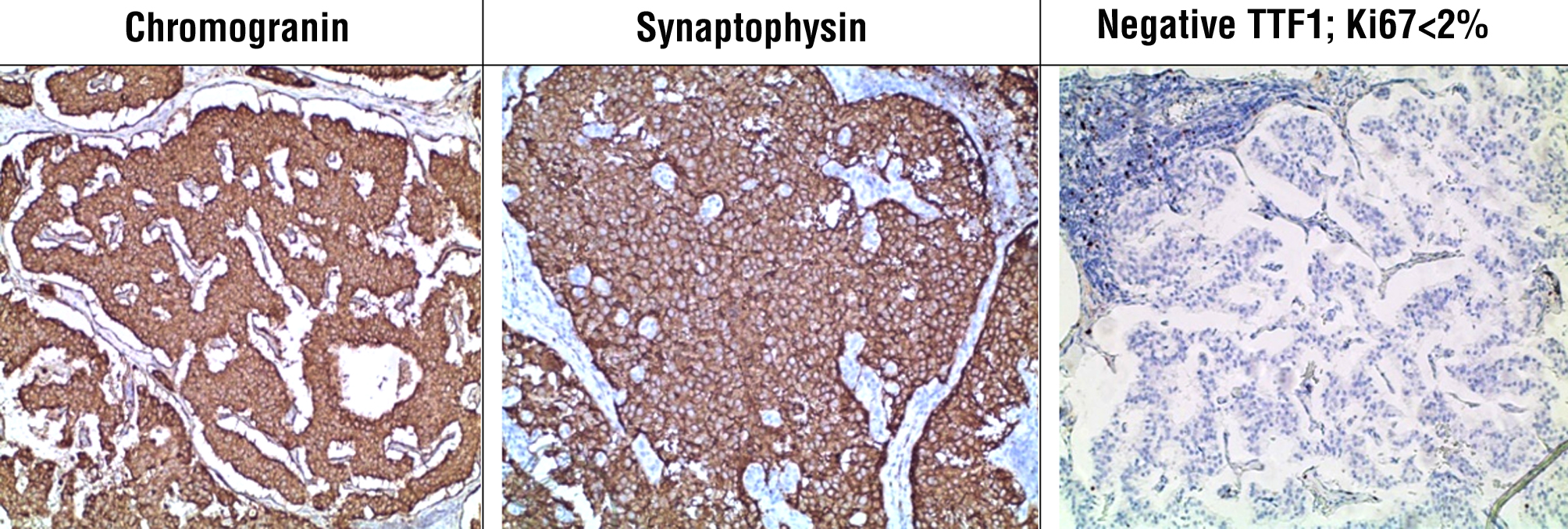
Colonoscopy was done on seven patients, gastroscopy on 4 patients. In three patients the colonoscopy revealed a full (complete) obstruction at rectum level between 7 and 12 cm from the anal line. In two patients, at the level of the ascending colon tumor, a formation was located with image of recent bleeding and insignificant bleeding after biopsy. Two of the patients were operated in emergency because of a clinical presentation of few days’ ileus proven by the X-ray and CT scan. A Hartmann procedure was made and liver biopsy was taken. The CT scan showed a presence of metastases in both patients with rectal NEN and in the patients with colonic NEN. The other patients were admitted in the clinic for elective surgery. Immunohistochemical study finding out that tumor cells show cytoplasmic expression of Chromogranin A, Synaptophysin, and negative TTF1; Ki67 < 2% (fig. 3).
Figure 3 - Cytoplasmic expression
DISCUSSION
In 2010, the WHO classification defined this group of tumors as NEN - neuroendocrine neoplasms and divided them into neuroendocrine tumors and carcinomas (8).
Neuroendocrine tumors of the gastro-entero-pancreatic system have different components, clinical manifestations and prognostic indexes according to their anatomical locations, which requires different diagnostic and therapeutic strategies (4).
In order to achieve the most optimal prognosis, both TNM and WHO classification are applied at the same time, increasing specificity and sensitivity of the index (9).
The reasons for these characteristics are associated with the following factors: neuroendocrine cells are produced by immature stem cells and the cancer cells themselves can release certain substances that stimulate growth, proliferation and dissemination of the tumor cells.
The rectum takes second place (27.4%) after the small intestine in NETs of GIT (4,10). In most cases, r-NETs are asymptomatic and are diagnosed incidentally during FCS. Less commonly, r-NETs may present themselves with anal discomfort, rectal bleeding, and lower dyspeptic syndrome (11). Most r-NETs which arise from neuroendocrine epithelial cells appear as small round polypoid lesions characterized by smooth, normal or yellow-stained mucosa, with a round pit shape /Kudo classification type I/, or invisible vessels as described by Sano as type I (12,13). R-NETs are found between 4 and 10 cm above the dentate line, along the anterior or lateral wall of the rectum (14).
A comprehensive literature search of PubMed, MEDLINE of Collected Reviews was performed to identify all of the English language publications related to neuroendocrine tumors in the abdominal cavity in 2001 to 2022. The subject of most publications is a literature review of data, long-term results and systemic management based without presenting their own patients with NENs, except one Chinese study describing the treatment in 58 patients in three medical centers (15). Furthermore these researches are
separated by the location of the NENs, pancreas, (16-19) small intestine (20-25) and rectum (5, 26-31).
Our study showed that seven of our patients with rNENs (77.8%) had symptoms typical for rectal cancer with (the) diagnosis being established after operation and immunochemistry of the specimen were performed. The other two patients (22.2%) were admitted and operated in emergency with a clinical presentation of ileus. Besides the enlarged large bowel, CT scan revealed the tumor and lymph nodes and the presence of liver metastases. During the Hartmann procedure a biopsy was taken from the liver. Histopathology form both the tumor and the metastases confirmed the diagnosis of a r-NEN and metastases from r-NEN. After the operation patients were subjected to chemotherapy. The patients with NEN of the small intestine were also admitted in emergency with a clinical presentation of ileus which was confirmed via X-ray and CT scan of the abdomen. We can say that all of the patients with NEN were admitted too late in surgery and all the modern techniques for early diagnosis couldn’t be applied because the patients needed emergency surgical treatment in the first place. From other point of view the complaints of the patients were not specific and for that reason the medical personnel outside the hospital couldn’t recognize the early symptoms of NEN. Suspicion of rNENs before their resection is very important from a clinical standpoint. The main goal is R0 resection and lymph node dissection.
CONCLUSION
Rectal NETs are among the most common NETs of the GI tract, along with small bowel NETs. Their incidence has increased significantly in the last few years due to the wide useof endoscopic screening for colorectal cancer and the improvement in endoscopic techniques. There is still an underestimation of the frequency and prevalence of these neoplasms as they are difficult to be diagnosed by the endoscopist.
The diagnosis and treatment of NETs is a multi-disciplinary process. The surgical treatment of NETs should be discussed in carefully selected patients with functional tumors, especially in the cases when they can be safely removed.
Conflict of interests
The authors have no conflict of interests to declare.
Funding
No funding or financial assistance was received bythe authors.
REFERENCES
1.Langhans T Über einen Drüsenpolyp im ileum. Virchows Archiv. 1867;38(4):559–560.
2.Oberndorfer S Karzinoide tumoren des dunndarms. Frankfurt Z Path. 1907;1:426–432.
3.Williams ED, Sandler M. The classification of carcinoid tumours. Lancet. 1963;1(7275):238–239.
4.Gavrilescu MM, Hutanu I, Filip B, Anitei MG, Buna-Arvinte M, et al. Hindgut and Midgut Neuroendocrine Tumors – Therapeutic Approach. Chirurgia (Bucur). 2019;114(2):243-250.
5.Osagiede O, Habermann E, Day C, Gabriel E, Merchea A, Lemini R, et al. Factors associated with worse outcomes for colorectal neuroendocrine tumors in radical versus local resections. J Gastrointest Oncol 2020;11:836-846.
6.Capella C, Heitz PU, Hofler H, Solcia E, Kloppel G. Revised classification of neuroendocrine tumours of the lung, pancreas and gut. Virchows Arch. 1995;425(6):547–560.
7.Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76(2):182–188.
8.Chablaney S, Zator ZA, Kumta NA. Diagnosis and Management of Rectal Neuroendocrine Tumors. Clin Endosc. 2017;50(6):530-36.
9.Shim KN, Yang SK, Myung SJ, Chang HS, Jung SA, Choe JW, et al. Atypical endoscopic features of rectal carcinoids. Endoscopy 2004; 36: 313-316 [PMID: 15057680 DOI: 10.1055/s-2004-814202
10.Fraenkel M, Kim M, Faggiano A, de Herder WW, Valk GD; Knowledge NETwork. Incidence of gastroenteropancreatic neuroendocrine tumours: a systematic review of the literature. Endocr Relat Cancer 2014;21:R153-R163
11.Gut P, Waligorska-Stachura J, Czarnywojtek A, Sawicka-Gutaj N, B?czyk M, Ziemnicka K, et al. Hindgut neuroendocrine neoplasms - characteristics and prognosis. Arch Med Sci. 2017;13(6):1427-32.
12.D?bkowskibkowski K, Szczepkowski M, Kos-Kud?a B, Starzynska T. Endoscopic management of rectal neuroendocrine tumours. How to avoid a mistake and what to do when one is made? Endokrynol Pol. 2020;71(4):343-349.
13.Park SB, Kim DJ, Kim HW, Choi CW, Kang DH, Kim SJ, Nam HS. Is endoscopic ultrasonography essential for endoscopic resection of small rectal neuroendocrine tumors? World J Gastroenterol 2017; 23: 2037-2043.
14.Sorbye H, Strosberg J, Baudin E, Klimstra DS, Yao JC. Gastro-enteropancreatic high-grade neuroendocrine carcinoma. Cancer 2014;120:2814-2823.
15.Wang Z, Liu Z, Wen Z, Li R, An K, Mei S, et al. Evaluation of radical surgical treatment in the management of 58 locally advanced rectal neuroendocrine neoplasms, one multicenter retrospective study. Eur J Surg Oncol. 2021;47(12):3166-3174.
16.Chang A, Sherman SK, Howe JR, Sahai V. Progress in the Management of Pancreatic Neuroendocrine Tumors. Annu. Rev. Med. 2022.73:213–29
17.Concors SJ, Sinnamon AJ, Ecker BL, Metz DC, Vollmer CM, Fraker DL, et al. The impact of surgery for metastatic pancreatic neuro-endocrine tumor: a contemporary evaluation matching for chromogranin A level. HPB (Oxford). 2020; 22(1):83-90.
18.Yang M, Zeng L, Ke N-W, Tan CL, Tian Bl, Liu XB, et al. 2020. World Health Organization grading classification for pancreatic neuro-endocrine neoplasms: a comprehensive analysis from a large Chinese institution. BMC Cancer. 2020;20(1):906.
19.Howe JR, Merchant NB, Conrad C, Keutgen XM, Hallet J, Drebin JA, et al. 2020. The North American Neuroendocrine Tumor Society Consensus Paper on the Surgical Management of Pancreatic Neuroendocrine Tumors. Pancreas. 2020;49(1):1-33.
20.Keck KJ, Maxwell JE, Utria AF, Bellizzi AM, Dillon JS, O’Dorisio TM, et al. The Distal Predilection of Small Bowel Neuroendocrine Tumors. Ann Surg Oncol. 2018;25(11):3207-3213.
21.Hernandez-Trejo JA, Suarez-Perez D, Gutierrez-Martinez IZ, Femandez-Vargas OE, Serrano C, Candelario-Martinez AA, et al. The pro-inflammatory cytokines IFNgamma/TNFalpha increase chromogranin A-positive neuroendocrine cells in the colonic epithelium. Biochem J. 2016;473(21):3805–18.
22.Trana CG, Shermanb SK, Howeb JR. Small Bowel Neuroendocrine Tumors. Curr Probl Surg. 2020;57(12):100823.
23.Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, P Schirmacher, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76(2):182–188.
24. Tran CG, Sherman SK, Scott AT, Ear PH, Chandrasekharan C, Bellizzi AM, et al. It Is Time to Rethink Biomarkers for Surveillance of Small Bowel Neuroendocrine Tumors. Ann Surg Oncol. 2021;28(2):732-741.
25. Scott AT, Howe JR. Management of Small Bowel Neuroendocrine Tumors. Surg Oncol Clin N Am. 2020;29(2):223–241.
26. Bruera G, Giuliani A, Romano L, Chiominto A, Di Sibio A, Mastropietro S, et al. Poorly differentiated neuroendocrine rectal carcinoma with uncommon immuno- histochemical features and clinical presentation with a subcutaneous metastasis, treated with first line intensive triplet chemotherapy plus bevacizumab FIr-B/FOx regimen: an experience of multidisciplinary management in clinical practice. BMC Cancer. 2019;19(1):960.
27. Gallo C, Rossi RE, Cavalcoli F, Barbaro F, Boškosk Ii, Invernizzi P, et al. Rectal neuroendocrine tumors: Current advances in management, treatment, and surveillance World J Gastroenterol. 2022; 28(11):1123-1138.
28. Wang XY, Chai NL, Linghu EQ, Li HK, Zhai YQ, Feng XX, et al. Efficacy and safety of hybrid endoscopic submucosal dissection compared with endoscopic submucosal dissection for rectal neuro-endocrine tumors and risk factors associated with incomplete endoscopic resection. Ann Transl Med. 2020;8(6):368.
29. Volante M, Grillo F, Massa F, Maletta F, Mastracci L, Campora M, et al. Neuroendocrine neoplasms of the appendix, colon and rectum. Pathologica. 2021;113(1):19-27.
30. Mestier L, Lorenzo D, Fine C, Cros J, Hentic O, Walter T, et al. Endoscopic, transanal, laparoscopic, and transabdominal management of rectal neuroendocrine tumors. Best Pract Res Clin Endocrinol Metab. 2019;33(5):101293.
31. Kojima M, Chen Y, Ikeda K, Tsukada Y, Takahashi D, et al. Recommendation of long-term and systemic management according to the risk factors in rectal NETs patients. Sci Rep. 2019; 9(1):2404.
Full Text Sources:
Abstract:
Views: 6840

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.