Surgery, Gastroenterology and Oncology

|
|
Background: Alcohol consumption is increasing worldwide, as being the most popular drug used for recreational purposes. Excessive consumption leads to irreversible liver damage, and since 2015 alcoholic cirrhosis has become the main indication of liver transplantation (LT).
Methods: Our aim was to create the epidemiological profile, of the cirrhotic patient who consumes alcohol and is considered a candidate for LT. Evaluation of alcohol consumption by applying three screening questionnaires: CAGE, AUDIT-C and FAST. Survival rates and LT event during 12-month follow-up.
Results: In the prospective cohort study, we included >70% males, 76.6% of patients exposed to alcohol, disease severity at baseline was greater for those with alcohol exposure MELD 15 vs. 13 and MELD-Na 18 vs. 14, long-term abstinence 40.3% vs. 85.4% exposure to risky amounts vs. rational. Dependence or at-risk drinking scores were significantly more frequent in patients with alcohol exposure (c2 38.5-56.63; p < 0.001), but rather similar between patients with alcohol exposure alone vs. combined exposure (c2 0.01-0.29; p=0.585-0.916). Multivariate analysis highlights only 2 CAGE questionnaires (OR 8.71; 95% CI 2.70-28.12; p<0.001 and OR 6.97 95% CI 1.79-27.12; p=0.005) and AUDIT-C (OR 12.18; 95 % CI 4.42-33.57; p < .001 and OR 12.57; 95% CI 3.72-42.49; p < .001) as significant for quantifying alcohol consumption. AUDIT-C the most sensitive for alcohol exposure Se = 79.1%, while CAGE and FAST had the best specificity Sp = 90.24% and 92.68%. After 12 months, 50% on the waiting list were exposed to alcohol vs. 36.6% other etiologies.
Conclusion: One-year survival, combined alcohol exposure patients was similar to those with only alcohol exposure under conditions of sobriety. We recommend that patients with combined etiology to be evaluated first for alcohol consumption.
INTRODUCTION
Alcohol is part of the social routine in many communities and accompanies socialization, being the most popular drug used for recreational purposes. Its consumption is on rising worldwide, tending to exceed the limits above which it becomes abusive. Alcohol abuse is common in Europe especially in Eastern Europe countries with about 200 illnesses or injuries due or related to its consumption (mental and behavioral disorders, addiction syndrome and organic conditions cancer, liver cirrhosis, cardiovascular disease) (1).
In 2016, alcohol was reported as the 5th risk factor for premature death and illness in active adults globally, representing 1:20 of the total, deaths attributed to alcohol consumption (2).
The general consumption of alcohol in Romania is equal to the European Union (EU) average (9.6 liters per capita, compared to 10 liters in 2014). The mortality rate related to alcohol abuse in Romania is the highest among EU countries (42 per 100,000) (3).
Until 2015, viral cirrhosis predominated in most patients evaluated for liver transplantation (LT). With the availability of new antiviral therapies, the frequency of this cause has decreased and patients with alcohol-induced cirrhosis (AC) have been considered for listing. The American Association for the Study of the Liver Diseases (AASLD) and the European Association for the Study of the Liver Diseases (EASL) have issued a consensus for changing the minimum 6-month abstinence requirement to a nuanced assessment of prognostic factors for alcoholic liver disease, on the basis of the patient's history and social support. It is recommended to consider both active and abstinent drinkers at the time of presentation for preLT evaluation (4).
Depending on the amount of alcohol consumed, it is defined as heavy alcohol consumption more than 3 drinks per day for men and more than 2 drinks per day for women, amounts that lead to alcoholic cirrhosis in 10-15 years. Some of them do not recognize their harmful drinking because of the anxiety or depression or the stigma of being labeled as an alcoholic. On the other hand, occasional and moderate alcohol consumption is usually not harmful, as it is represented by small amounts and not consumed daily (5).
MATERIAL AND METHODS
The aim of the study was to outline the epidemiological and demographic profile of the cirrhotic patient with alcohol consumption and to highlight the differences between patients who consume risky/harmful versus low/no quantities of alcohol by using screening questionnaires. Which patients had to undergo the 6-month abstinence rule before being considered transplant candidates.
The second objective was to assess the 12 months outcome in terms of survival rates and liver transplantation for each group of patients.
We conducted a prospective cohort study in which we included all the patients addressed to our clinic and diagnosed with cirrhosis to be evaluated and enrolled for LT. Therefore, we generated an electronic database where we entered the variables between June 2015 and May 2018, which had five moments surveillance of patients, first enrollment, 1, 3, 6, and 12 months, and adherence to surveillance was defined as an interval of maximum 6 months between examinations, and non-adherence included loss to follow-up after first or third month.
Inclusion criteria
Inclusion criteria were: first presentation in our clinic, gave the consent to be included in this study and agreed to answer the questions in 3 short screening questionnaires for alcohol consumption. The chosen questionnaires were CAGE, FAST and AUDIT-C. Next criteria were the presence of liver disease in cirrhotic stage, age over 20 years and the presence of hepato-cellular carcinoma (HCC) within the Milan criteria.
Exclusion criteria
Exclusion criteria were: patients who were previously included on the waiting list, cirrhosis recurrence after LT, HCC over Milan criteria, hepatic encephalopathy (unable to answer the questions), severe sepsis and disagreement to be included in the study.
The patients were divided into three groups depending on the admission diagnosis and alcohol consumption: cirrhosis due to alcohol consumption, viral or other liver cirrhosis with alcohol consumption and liver cirrhosis without or rational alcohol consumption.
The questionnaires were administered to each patient by the psychologist dedicated to addictions, staff from our hepatology department, after they were translated into Romanian. Patients were assured that responses would remain anonymous, confidential and participation is voluntary. Short, accessible, easy-to-use questionnaires with specific questions were chosen so that patients could answer them without much difficulty. Before starting the survey, it is recommended that the issue of alcohol consumption has not been discussed with the patients.
Because the AUDIT-C and FAST questionnaires have questions that refer to units of alcohol consumed, we searched for the significance of the standard unit. In the United States, a "standard drink" (or the equivalent of an alcoholic drink) contains about 14 g of pure alcohol (6,7), in contrast to European countries where the standard unit varies from 8 g to 16 g in different countries. For Romania, the standard drink is not yet defined, so we used the standard unit accepted in the United States.
Moderate alcohol consumption is limited to no more than 2 drinks per day for men and 1 drink or less per day for women on drinking days (8). Consumption above this threshold of two standard drinks per day appears to be associated with the risk of cirrhosis (9).
The 4-question CAGE questionnaire (awareness of reducing alcohol consumption, criticism of others, guilt and withdrawal syndrome) being an easy-to-use tool for detecting severe alcohol dependence. At a threshold of 2 points or more is considered clinically significant for alcohol dependence along with a yes answer to the last question denoting morning withdrawal syndrome (10).
AUDIT-C (AUDIT consumption) is the short version of the original AUDIT and includes the first 3 questions from ten questions AUDIT test. It became the screening tool of choice for busy practitioners. This questionnaire identifies the frequency, quantity and type of consumption and estimate hazardous alcohol consumption (11). The thresholds that indicate risky drinking are different for men (≥ 4 points) and for women (≥ 3 points) (12).
FAST, is a four-item questionnaire, it derived also from AUDIT, it screens and assess alcohol missuse without being a diagnostic test on its own. The scores are added up to obtaining a range from 0 to 16 points and the threshold > 3 points is considered significant for hazardous drinking (13). It was developed for use in busy medical units, with a high level of accuracy for alcohol consumption risk (14).
In order to obtain objective information about alcohol consumption, proper management of cirrhosis, assessment of the abstinence period and risk stratification for the next 12 months, all patients received questionnaires on the first day of admission. Using the questionnaire scores, we compared alcohol consumption between the 3 etiological groups.
Statistical analysis
All data were analyzed using SPSS statistical analysis software for Windows (Version 20.0). Continuous variables were expressed as median with interquartile range, categorical variables were expressed as frequency and percentages and compared using the chi-square test for categorical variables and Nonparametric Mann-Whitney U Test for Independent-Samples for continuous variables. The p-values for the comparison of two variables were significant for a value ≤ 0.05 and with marginal significance defined as the range 0.05–0.1. Univariate and multivariate models were used to identify predictors for the alcohol consumption in the case of multiple etiology. The accuracy of the questionnaires was indicated by the area under the ROC curve, sensitivity and specificity were calculated for each cut-off point and survival curves were obtained with Cox regression.
RESULTS
Descriptive analysis: 175 patients referred to our clinic with a diagnosis of liver cirrhosis accepted to be included in the study. Of these, 82 were still on the waiting list at 12 months, 26 died during the study, 47 were excluded from the study due to non-adherence to periodic evaluation and 20 were transplanted. In the group, 136 (77.71%) were male and only 39 (22.29%) were female. The diagnosis at the first admission, 134 (76.6%) only the alcoholic component or associated with: virus (B, C, D or coinfection) or other causes and 41 of the patients (23.4%) cirrhosis without mentioning the alcoholic cause.
The patients with alcohol consumption in quantities above the risk value were younger, with a median age of 53 years, they come from the south of the country, from the urban environment. Alcohol consumers also had the highest MELD and MELD-Na score, those having abstinence for less than 6 months (59.7%) (table 1).
Table 1 - Demographic and epidemiological cohort data

Based on the admission diagnosis, the patients were divided into two groups: those with alcohol exposure 134 (76.7%) and those without alcohol exposure 41 (23.4%).
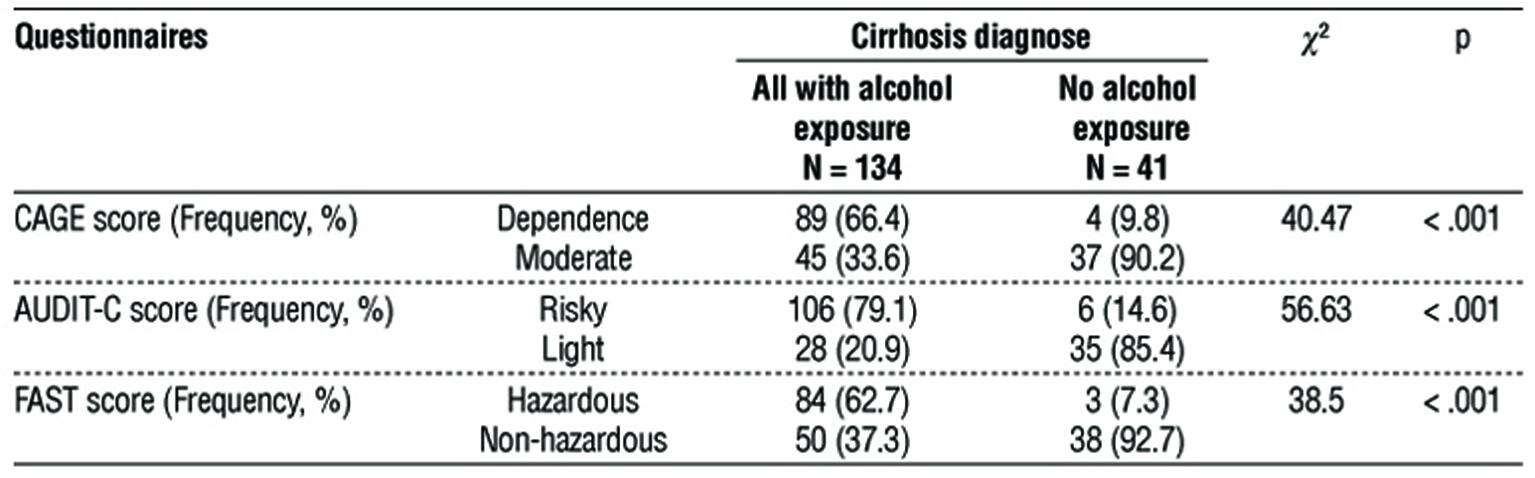
The initial statistical processing was to compare the questionnaire scores of patients with alcohol exposure to those of patients without exposure according to initial diagnosis. All three questionnaires reached statistical significance for patients with scores above the cutoff values, with p < 0.001 (table 2).
Table 2 - Comparison between all patients with alcohol exposure and patients not exposed to alcohol admission cirrhosis diagnose, according to the threshold of the questionnaires.
The next step was to compare the score of patients exposed only to alcohol with the score obtained by patients with other causes of cirrhosis where we obtained statistically significant differences (table 3).
Table 3 - Comparison between patients with only alcoholic and nonalcoholic etiology of cirrhosis according to the threshold level of the three questionnaires.

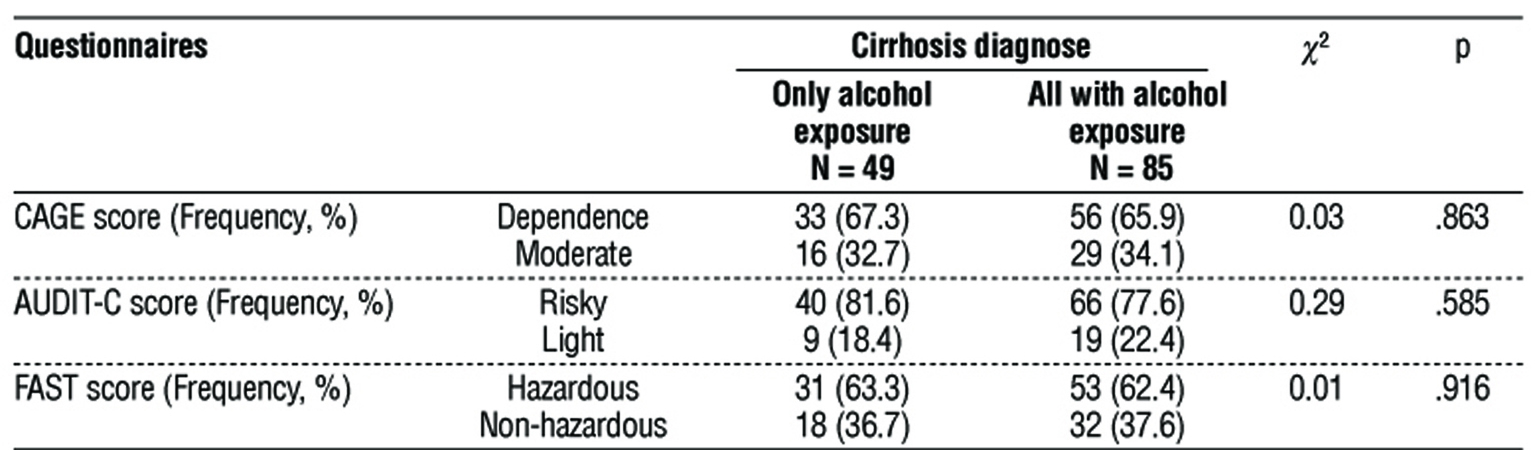
In the last comparison, we looked for the score difference between patients exposed only to alcohol and those with complex exposure to alcohol associated with other causes. The result was that there are no statistically significant differences (table 4).
Table 4 - Comparison between patients with only exposure to alcohol and those with alcohol associated with other causes, using the same threshold level of the three questionnaires.
In the univariate analysis, each applied questionnaire was an independent predictor for alcohol abuse, with statistical significance p < .001: the CAGE prediction score was 76.6%; OR 18.29 (95% CI 6.14-54.53); AUDIT-C with a prediction score of 80.6%; OR 22.08 (95% CI 8.45-57.73); FAST with prediction score 76.7% OR 21.28 (95% CI 6.24-72.54).
The multivariate analysis showed an increase of the prediction score to 86.3% when applying all three questionnaires to the patients, but statistical significance was obtained only for CAGE and AUDIT-C p < .001 (table 5, table 6).
Table 5 - Univariate and multivariate analysis of the three questionnaires for the prediction of alcohol abuse in advanced liver disease with alcohol exposure comparison with low or no alcohol exposure.

Table 6 - Univariate and multivariate analysis of questionnaire results between the group of patients with cirrhosis due to only alcohol exposure and those with cirrhosis low or no alcohol exposure.

We evaluated the performance of the model by applying the three questionnaires for the prediction of dangerous/harmful alcohol consumption, using the validated cut-off values in our patient group, sensitivity and specificity, positive and negative predictive values, prevalence and accuracy. The probability of being correctly diagnosed was over 80% for AUDIT-C and over 70% for CAGE. For the cut-off values validated in the literature, all questionnaires had good specificity and the highest sensitivity was obtained with AUDIT-C (table 7, table 8).
Table 7 - Diagnostic value of questionnaires according to ROC curve analysis for hazardous alcohol consumption in patients with all etiologies including alcohol exposure according to the validated cut-off

Table 8 - Diagnostic value of questionnaires according to ROC curve analysis for hazardous alcohol consumption in patients with only alcoholic etiology, according to the validated cut-off

Survival of patients with cirrhosis due to alcohol consumption alone and those with alcohol consumption associated with other etiologies at the end of the study was almost similar (p = 0.597), but compared to patients who did not have alcohol exposure achieve at limit statistical significance (p = 0.057 vs p = 0.062). Also those with alcohol exposure as the sole cause of cirrhosis, as well as those in which it is associated with other causes, have a significantly better 12-month survival prognosis if they become abstinent. For those without alcohol exposure or with combined exposure, the evolution is more difficult with a higher mortality due to the persistence of the pathogen (fig. 1).
Figure 1 - Cox regression survival curves compare alcohol consumers (only or in combination with other causes) with non-consumers and alcohol consumers between only and combined to other causes.

DISCUSSION
Inclusion on the waiting list for LT of patients with cirrhosis and alcohol consumption is still conditional on abstinence for more than 6 months, this period is still controversial in the medical literature (15,16), but is highly recommended in clinical guidelines for the management of patients with active alcohol consumption the cause of cirrhosis. Abstinence from alcohol under 6 months being presented as the strongest risk factor for post-LT recidivism (17). Our cohort, similar to other studies in the literature, included mostly men (18), the alcohol consumers being younger and having abstinence for less than 6 months or being active consumers.
Our center was easily accessible for patients from the southern part of the country and 2/3 of them live in the urban environment. In the literature, there are equivocal data regarding the association of a certain type of alcohol with increased risk for liver damage (19). However, in our group of patients we found certain differences between the type of alcohol preferred and the cause of cirrhosis. Patients with alcohol exposure only preferred strong drinks, those with alcohol exposure and other causes consumed all types of alcohol, and those with occasional and rational consumption preferred beer and wine.
Clinical practice must be based on objective data on alcohol consumption, not just patient statements. In the diagnosis of cirrhosis at admission, mention of the alcoholic cause is avoided, as this represents a stigma for the patient, therefore DMS-5 recommends using the expression severe alcohol consumption disorder instead of the old name of alcoholic cirrhosis (20). Applying the 3 screening tests from the first admission, we obtain objective information about the amount of alcohol consumed (moderate and risky or harmful consumption), the frequency of consumption, alcohol dependence and how aware they are of the danger produced by alcohol (21).
The fact that alcohol exposure is self-assessed by each patient is considered a limitation of this study. Another limitation is denial of alcohol use or abuse or underestimation of amount and frequency, very common among heavy drinkers, who often overestimate actual alcohol consumption.
For inclusion and prioritization on the waiting list, the MELD score for severity of liver disease with a cutoff greater than 15 points and MELD-Na with a cutoff of 21 points are used, the latter providing a more accurate prediction of survival than MELD alone (22). At the first presentation, patients exposed to alcohol had higher MELD and MELD-Na liver disease severity scores than those not exposed to alcohol consumption.
Survival analysis at one year of follow-up found a mortality of 15% per year, and just 11% received a liver graft in the entire cohort. More than a quarter of patients (27%) left the study and 82 (46.9%) were still on the waiting list after 12 months, of which 67 (50%) exposed to alcohol and 15 (36.6%) without exposure to alcohol. Deaths were twice as high in the group of those not exposed to alcohol. The evolution of patients with short-term exposure to alcohol for 12 months was better, contrary to the fact that at admission the MELD and MELD-Na scores were higher. So abstinence from alcohol significantly improves survival in one year.
The results obtained from the 3 questionnaires had significant differences in the volume of alcohol consumed in all patients with alcohol exposure, compared to those without or moderate alcohol exposure. When analyzing the answers to the three questionnaires using validated cut-offs, all patients with alcohol exposure had scored above the threshold in a proportion of > 60% compared to those without alcohol exposure who scored below the threshold value in a proportion > 85%. Roughly equal proportions of harmful alcohol consumption or addiction were obtained when comparing patients with only alcohol to those who associate other causes. Although the literature shows that the AUDIT-C performs better than the CAGE in identifying alcohol abuse, in our study there were no significant differences between these two tests (23).
Each questionnaire was found, in the univariate analysis, to be a significant predictor of the heavy alcohol consumption, bringing important information about the frequency, quantity and quality of life of those who consume large amounts of alcohol and how aware they are of the risk of their habit. In clinical practice, each of these three questionnaires could be independently applied for more accuracy on alcohol consumption in cirrhotic patients.
The multivariate analysis showed that there was an improvement in the prediction when we used two questionnaires at the same time CAGE and AUDIT-C, which had statistical significance.
The most sensitive test was AUDIT-C in our study for alcohol exposure with the highest accuracy > 80%, followed by CAGE with a high positive predictive value of > 89% for identifying abuse or dependence (24) and the last but not the least one FAST test with the highest specificity > 91%. AUDIT-C and FAST are short versions of the same 10 questions AUDIT test, but they are complementary (23). Literature presents AUDIT-C having 73% sensitive and 89% specific for alcohol use disorder, and for alcohol dependence it has 85% sensitivity and 89% specificity (25), values that are similar to those obtained in our study for only alcohol exposure a sensitivity of 81.6% and 79.1% for combined. The literature finds for the CAGE questionnaire very wide ranges of sensitivities in a meta-analysis of 21-94% and specificities of 77-97% for alcohol abuse/or dependence at a threshold of 2 (25). The sensitivity and specificity of the CAGE questionnaire for our group of patients was 67.3% for only alcohol and 66.4% for combined.
And the FAST Alcohol Screening Test for a cut-off of 3 points performed worse with only a sensitivity of 63.3% and 62.7% for only alcohol and combined, in our study. Gomez et al. (26) in 2005 included primary care patients reporting 0.80 sensitivity and 0.94 specificity for FAST in detection of hazardous drinking and Hodgson et al. (27) in 2003 showed better results with a sensitivity and specificity of 0.93 and 0.88, respectively.
By ceasing consumption and achieving long-term abstinence, patients who have, only or associate alcohol exposure as cause of liver disease will have a better outcome compared to those who have persistent causes (viral or other) in the absence of etiological treatment.
CONCLUSION
For the screening of alcohol consumption at the first hospitalization in the hepatology department for transplantation, the use of the CAGE and AUDIT-C questionnaires in patients who are to be included on the waiting list proves to be sufficient. Cirrhotic patients who have combined exposure to alcohol and viruses or others and who obtain a score of dependence or at-risk alcohol consumption in these questionnaires will have to be included in a psychological counseling program to achieve and maintain abstinence from alcohol similar to those with only exposure to alcohol. It is necessary to observe the 6 months of abstinence before they can be proposed for TH. Their survival will improve 12 months after achieving abstinence compared to those not exposed to alcohol.
Conflict of interest
All authors declare no conflict of interest.
Funding
No funding.
Ethical statement
The study protocol conforms to the 1975 Declaration of Helsinki and was approved by the Fundeni Clinical Institute Review Board.
REFERENCES
- World health statistics 2019: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2019. Available from: https://www.who.int/publications/i/item/ 9789241565707
2. Alcohol Facts and Statistics; NIH Turning Discovery Into Health®, National Institute on Alcohol Abuse and Alcoholism. Available from: https://www.niaaa.nih.gov/alcohols-effects-health/alcohol-topics/alcohol-facts-and-statistics.
3.OECD/European Observatory for Health Systems and Policies (2017), Romania: Health Profile by Country 2017, The State of Health in the EU, OECD Publishing, Paris/European Observatory for Health Systems and Policies, Brussels. Available from: http://dx.doi. org/10.1787/9789264283534-en
4.Wong RJ, Singal AK. Trends in Liver Disease Etiology Among Adults Awaiting Liver Transplantation in the United States, 2014-2019. JAMA Netw Open. 2020;3(2):e1920294.
5.Axley PD, Richardson CT, Singal AK. Epidemiology of Alcohol Consumption and Societal Burden of Alcoholism and Alcoholic Liver Disease. Clin Liver Dis. 2019;23(1):39-50.
6.https://www.niaaa.nih.gov/alcohols-effects-health/overview-alcohol-consumption/what-standard-drink
7. Kalinowski A, Humphreys K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction. 2016;111(7):1293-1298.
8. Snetselaar LG, de Jesus JM, DeSilva DM, Stoody EE. Dietary Guidelines for Americans, 2020-2025: Understanding the Scientific Process, Guidelines, and Key Recommendations. Nutr Today. 2021;56(6):287-295.
9. Louvet A, Trabut JB, Moreno C, Moirand R, Aubin HJ, Ntandja Wandji LC, et al. Management of alcohol-related liver disease: the French Association for the Study of the Liver and the French Alcohol Society clinical guidelines. Liver Int. 2022;42(6):1330-1343.
10. Williams N. The CAGE questionnaire. Occup Med (Lond). 2014; 64(6):473-474.
11. Khadjesari Z, White IR, McCambridge J, Marston L, Wallace P, Godfrey C, et al. Validation of the AUDIT-C in adults seeking help with their drinking online. Addict Sci Clin Pract. 2017;12(1):2.
12. Reinert DF, Allen JP. The alcohol use disorders identification test: an update of research findings. Alcohol Clin Exp Res. 2007;31(2):185-199.
13. Williams N, The FAST questionnaire, Occupational Medicine. 2014;64(7);559-560.
14. John B, Newstead S, Heirene R, Hodgson R, Roderique-Davies G. Does the Fast Alcohol Screening Test Accurately Distinguish Between Harmful and Severely Dependent Tiers of Alcohol Misuse? Alcohol Alcohol. 2021;56(6):737-745.
15. Dew MA, DiMartini AF, Steel J, De Vito Dabbs A, Myaskovsky L, Unruh M, et al. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transpl. 2008;14(2):159-172.
16. Marroni CA. Management of alcohol recurrence before and after liver transplantation. Clin Res Hepatol Gastroenterol. 2015;39 Suppl 1: S109-S114.
17. Yu TW, Chen YM, Wang CC, Lin CC, Huang KT, Liu YW, et al. Incidence and Risk Factors of Alcohol Relapse after Liver Transplantation: Analysis of Pre-Transplant Abstinence and Psychosocial Features. J Clin Med. 2020;9(11):3716.
18. Legaz I, Navarro-Noguera E, Bolarín JM, García-Alonso AM, Luna Maldonado A, Mrowiec A, et al. Epidemiology, Evolution, and Long-Term Survival of Alcoholic Cirrhosis Patients Submitted to Liver Transplantation in Southeastern Spain. Alcohol Clin Exp Res. 2016; 40(4):794-805.
19. Crabb DW, Im GY, Szabo G, Mellinger JL, Lucey MR. Diagnosis and Treatment of Alcohol-Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology. 2020;71(1):306-333.
20. Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry. 2015;72(8):757-766.
21. Serier KN, Venner KL, Sarafin RE. Evaluating the Validity of the DSM-5 Alcohol Use Disorder Diagnostic Criteria in a Sample of Treatment-seeking Native Americans. J Addict Med. 2019;13(1): 35-40.
22. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J Hepatol. 2016;64(2): 433-485.
23. Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007;31(7):1208-1217.
24. Malet L, Schwan R, Boussiron D, Aublet-Cuvelier B, Llorca PM. Validity of the CAGE questionnaire in hospital. Eur Psychiatry. 2005;20(7):484-489.
25. Torruellas C, French SW, Medici V. Diagnosis of alcoholic liver disease. World J Gastroenterol. 2014;20(33):11684-11699.
26. Gómez A, Conde A, Santana JM, Jorrín A. Diagnostic usefulness of brief versions of Alcohol Use Disorders Identification Test (AUDIT) for detecting hazardous drinkers in primary care settings. J Stud Alcohol. 2005;66(2):305-308.
27. Hodgson RJ, John B, Abbasi T, Hodgson RC, Waller S, Thom B, et al. Fast screening for alcohol misuse. Addict Behav. 2003;28(8): 1453-1463.
Full Text Sources:
Abstract:
Views: 1959

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.