Surgery, Gastroenterology and Oncology

|
|
Introduction: We present an extremely rare case of gastric outlet obstruction (GOO) in a young male attributed to hydrops of the gallbladder resulting from recurrent episodes of acute acalculous cholecystitis. Remarkably, approximately one and half years prior to this presentation, the patient was diagnosed with confirmed acute acalculous cholecystitis and had tested positive for Covid 19 ,despite exhibiting no respiratory symptoms.
Case report: While it is established that Patients with acute acalculous cholecystitis can develop gallbladder mucoceles due to the mechanism akin to mechanical cystic duct obstructions. This functional condition leads to a non-emptying, distended gallbladder where biliary mucus replaces bile salts (1). Conventionally, hydrops of the gallbladder is associated with prolonged blockage of the cystic duct, often caused by an impacted gallstone in neck/cystic duct or a stricture in cystic duct. Bouveret’s Syndrome, characterized by gastric outlet obstruction (GOO) results from the impaction of a large gallstone in the duodenum or pyloric channel, typically secondary to a cholecystoenteric fistula (2), is a recognized rare entity. However, our case stands apart as it elucidates an infrequently reported cause of GOO-hydrops of gall bladder inducing extrinsic compression of the duodenum/pylorus and this case also emphasizes the distinction from Bouveret’s syndrome.
Conclusions: This case underscores the importance of considering unusual etiologies in the diagnosis of GOO and emphasizes the need for timely recognition and intervention in such rare instances to ensure optimal patient outcomes. Additionally, we provide a comprehensive review of existing literature, highlighting the scarcity of reported cases with such relevant presentations.
Introduction
The normal adult gallbladder typically measures 7-10 cm in length and 3-4 cm in transverse diameter (3). Gallbladder hydrops is characterized by overdistension of the gallbladder with mucoid or clear, watery contents over 1500 ML. Clinically, it is defined as gallbladder distention with an anterior-posterior diameter greater than 5 cm or enlargement surpassing 4 × 10 cm (4). The common cause of gallbladder hydrops is prolonged blockage of the cystic duct often attributed to impacted gallstone in the neck/cystic duct (5). Less frequent etiologies encompass cystic duct stricture, cystic fibrosis, tumours, kinking of the cystic duct, or external compression by inflammatory or neoplastic masses. In paediatric cases, gallbladder hydrops typically arises from acute processes associated with infectious diseases or inflammatory disorders, such as streptococcal infections, mesenteric adenitis, typhoid, leptospirosis, viral hepatitis, familial Mediterranean fever, and Kawasaki’s syndrome (4). The occurrence of GOO due to extrinsic compression of the pylorus/duodenum secondary to gallbladder hydrops is an exceedingly rare phenomenon, with only a handful of reported cases globally. The mechanism involves the mass and size of hydrops of the gallbladder compressing the neighbouring structures such as the pylorus/duodenum, ultimately resulting in GOO. Furthermore, if gallbladder hydrops is identified, establishing the underlying cause becomes imperative for effective management. This introduction sets the stage for the unique case presented, emphasizing the rarity of the condition and the importance of considering it in the diagnostic approach to GOO.
Figure 1 - Ultrasound scan abdomen showed hugely distended gallbladder with pericholecystic stranding

Case Report
We present a unique case of a 23-year-old male who initially sought medical attention in April 2021 with pain in right hypochondriac region. Clinical examination revealed localized tenderness in right hypochondriac region. Further evaluation, including blood tests and imaging, led to the diagnosis of Covid 19 induced acute acalculous cholecystitis. Notably, the patient had no respiratory symptoms, making this presentation exceptionally rare. His inflammatory markers were normal and so were liver function tests except ALT level which was moderately raised. Ultrasound scan abdomen showed hugely distended gallbladder with pericholecystic stranding (fig. 1). Then a CT scan abdomen and pelvis was done which reconfirmed ultrasound findings (fig. 2). We are aware that Covid 19 infection presenting as acute acalculous cholecystitis is extremely rare in the medical literature and only three cases have been reported in literature. The following findings in our case were very much favouring it being Covid 19 induced acute calculous cholecystitis, scan proven findings of acute acalculous cholecystitis (gallbladder distension, pericholecystic fluid, marked gallbladder wall thickening, no gallstones), normal inflammatory markers like CRP and WBC count normal Bilirubin and alkaline phosphatase, but moderately raised ALT, and being covid positive without any respiratory symptoms. He was managed conservatively and then discharged. He was followed up in the outpatient clinic with follow up MRCP scan which was reported as normal with optimally distended gallbladder (fig. 3).
Figure 2 - CT scan abdomen and pelvis was done which reconfirmed ultrasound findings
Following conservative management, the patient experienced intermittent pain associated with on and off nausea during outpatient follow ups. He was also offered upper GI endoscopy which was attempted but he could not tolerate.
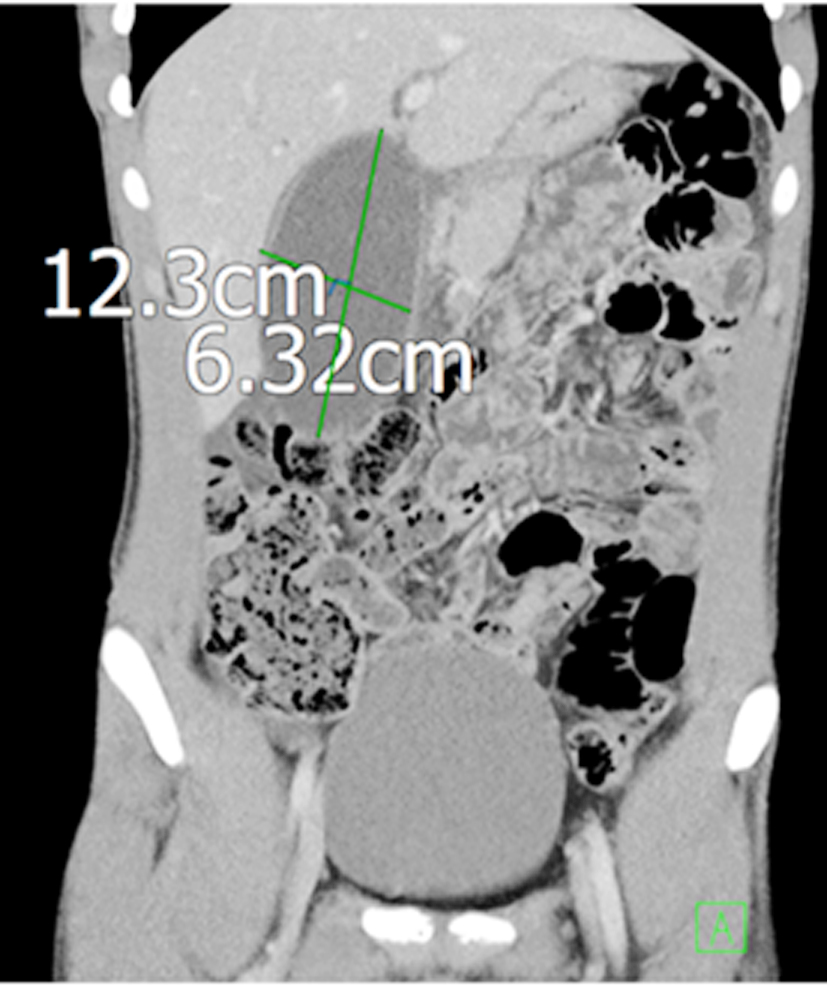
In September 2023 he returned with recurrent pain in right hypochondriac region associated with vomiting. On clinical examination he was tender in right hypochondriac region. He was evaluated with blood tests and imaging. His inflammatory markers were raised (WBC count and CRP). The contrast enhanced CT scan abdomen and pelvis revealed pericholecystic fluid and hugely distended gallbladder causing compression over the pylorus/duodenum thus causing mechanical gastric outlet obstruction (fig. 4). MRCP scan also reconfirmed the findings (fig. 5) and did not show any stones or strictures anywhere in the biliary tract.
Figure 3 - MRCP scan reported as normal with optimally distended gallbladder

Multidisciplinary team review confirmed the diagnosis of infected hydrops of the gallbladder causing features of gastric outlet obstruction, prompting a recommendation of cholecystectomy.
Cholecystectomy was offered to the patient with the aim of removing the potential source of GOO. An attempt was made for laparoscopic cholecystectomy and findings were confirmed; hugely distended gallbladder, omental wrapping, hepatic flexure was adherent and inseparable from the gallbladder due to dense adhesions and pylorus/first part of duodenum were also stuck to it. In view of these findings, it was converted to open exploration.
Figure 4 - The contrast enhanced CT scan abdomen and pelvis revealed pericholecystic fluid and hugely distended gallbladder causing compression over the pylorus/duodenum thus causing mechanical gastric outlet obstruction

Hugely distended gallbladder was aspirated to allow decompression of the gallbladder, and more than a litre of purulent mucoid bile was aspirated. Aspirated fluid sample sent for culture and sensitivity. Omentum and hepatic flexure were dissected off the gallbladder, then part of the gallbladder compressing the pylorus/duodenum was lifted away from them with fine dissection. Hepatocytic triangle could not be accessed as it was plastered. Finally, fundus first approach was used to dissect the gallbladder from the liver bed with bipolar diathermy. Further dissection was stopped above the sulcus of Rouvier and plane of R4U line. At this point the gall-bladder was opened and inspected from inside especially to visualise opening of neck/cystic duct interface. No impacted stones were found, and no cystic duct opening was visible. In view of these findings reconstructive near total cholecystectomy was performed and cuff of gallbladder covering CHD/ CBD was kept behind to prevent any damage to CBD/CHD. It was sutured with 3-0 continuous PDS stich.
The patient’s postoperative recovery was uneventful and follow up revealed complete resolution of symptoms. The histology of the gallbladder showed features consistent with infected hydrops of the gallbladder.
Figure 5 - MRCP scan also reconfirmed the findings and did not show any stones or strictures anywhere in the biliary tract

Discussion
Our case presents an extremely rare cause of gastric outlet obstruction (GOO) secondary to hydrops of the gallbladder resulting from recurrent acute acalculous cholecystitis. Hydrops or mucocele of the gallbladder is characterized by abnormal mucus accumulation causing excessive distension of gallbladder. The pathogenesis involves inflammatory changes in the gall bladder, altered secretions, reduced bile flow, impaired gall bladder motility and altered absorption of water from the lumen of gallbladder (6).
Notably, the patient had a history of possibly Covid 19 induced acute calculous cholecystitis a year and half before presenting with hydrops induced GOO. While Covid 19 primarily affects the respiratory system, its gastrointestinal (GI) involvements are also well-known, particularly hepatic involvement presenting as mild to moderate transaminitis. The occurrence of Covid -19 induced acalculous cholecystitis is exceedingly rare with only three reported cases in the literature (7).
The precise pathogenesis of Covid 19 associated acute acalculous cholecystitis remains unclear, but the virus has a demonstrated tropism for the liver. The virus’s entry into liver cells is facilitated through
interaction with the angiotensin-converting enzyme 2 receptor (ACE2), present in various tissues, including the liver and biliary ducts. Autopsies in SARS-CoV cases revealed viral RNA inside hepatocytes with diverse patterns of hepatic injuries (8).
It seems his intermittency of symptoms with episodes of vomiting followed by weeks of symptom relief exhibited that the features of GOO were initially waxing and waning and were getting precipitated by positional changes and fluctuations in the gallbladder size. It was only when he got a severe flareup one and half years after the first attack that the CT scan confirmed actually extrinsic compression of the pylorus /duodenum, thereby clinching this diagnosis.
The definitive treatment for this condition is cholecystectomy, with the choice of Laparoscopic or open approach depending on expertise or technical or anatomical considerations. Potential complications of cholecystectomy include bile leak, bleeding, infections, and injuries to nearby structures (9). Percutaneous cholecystostomy is reserved for unfit patients OR in unwell patients as a bridge to surgery at later date.
This case underscores the diagnostic challenges posed by rare presentations and emphasizes the role of surgery in managing such unusual complications, showcasing the importance of multidisciplinary approach in decision making.
Conclusion
In conclusion, while gallbladder hydrops secondary to recurrent acute acalculous cholecystitis is a rare phenomenon, our case underscores the significance of considering it in the differential diagnosis of gastric out let obstruction (GOO). The intermittent nature of symptoms and waxing and waning pattern observed in our patient highlight the diagnostic challenges posed by this uncommon condition. Establishing the cause of Gallbladder hydrops ,especially when associated with GOO, is crucial for appropriate management. This case also emphasizes the distinction from Bouveret’s syndrome. Our case introduces a novel cause of GOO, shedding light on the rarity of this presentation resulting from hydrops of the gall bladder secondary to recurrent acalculous cholecystitis.
Furthermore, the case emphasises the importance of multidisciplinary team management in navigating complex and unusual clinical scenarios. Timely recognition of such rare causes and prompt surgical intervention, when feasible, are crucial in achieving optimal patient outcomes.
Author’s contributions
AGH, AE &AJ: contributed to the clinical data collection; AGH and MZ: contributed to the design of the case report presentation; AGH, SIH, LS and BP: performed the final revision of the manuscript.
Conflict of interest
None declared.
Funding
No funding sources.
Ethical approval
Not required.
Acknowledgements
We acknowledge Tracy Bell-Surgical Secretary, for proof-reading this manuscript.
References
1. Clemente G, Fico V, De Sio D, De Rose AM. The Mucocele of the Gallbladder. J Gastrointest Surg. 2017;21(8):1366-1367.
2. Caldwell KM, Lee SJ, Leggett PL, Bajwa KS, Mehta SS, Shah SK. Bouveret syndrome: current management strategies. Clin. Exp. Gastroenterol. 2018;15(11):69–75.
3. Gallbladder. https://radiopaedia.org/articles/12413 2021
4. MacSween RNM, Burt AD, Portmann BC, Ishak KG, Scheuer PJ, Anthony PP. Pathology of the Liver. 4th ed. London: Churchill Livingstone; 2002.
5. Jones MW, Deppen JG. In: StatPearls. Treasure Island. Gallbladder Mucocele. FL: StatPearls Publishing; 2023 Jan.
6. Loh WL, Ng NZP, Kabir T, Chan CY. Rare case of gallbladder mucocele causing gastric outlet obstruction treated with cholecystectomy. Int J Surg Case Rep. 2019;57:84-87.
7. Balaphas A, Gkoufa K, Meyer J, Peloso A, Bornand A, McKee TA, et al. COVID-19 can mimic acute cholecystitis and is associated with the presence of viral RNA in the gallbladder wall. J Hepatol. 2020; 73(6):1566-1568.
8. Guo Y, Korteweg C, McNutt MA, Gu J. Pathogenetic mechanisms of severe acute respiratory syndrome. Virus Res. 2008;133(1):4-12.
9. Strasberg SM, Pucci MJ, Brunt LM, Deziel DJ. Subtotal cholecystectomy -"fenestrating" vs "reconstituting" subtypes and the prevention of bile duct injury: efinition of the optimal procedure in difficult operative conditions. J Am Coll Surg. 2016;222(1):89-96.
Full Text Sources:
Abstract:
Views: 7143

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.