Surgery, Gastroenterology and Oncology

|
|
Introduction: In all pathologic types of gastric cancer, adenocarcinoma is the most common, whereas the incidence of adenosquamous carcinoma (ASC) remains extremely low, accounting for less than 1% of total gastric malignancies. Due to the rarity of ASC, limited data are available to conclude the histogenesis, clinicopathologic characteristics, optimal treatment strategies, and prognosis. This rare clinical entity exhibits a higher prevalence in men, particularly in Asians, and typically manifests at advanced stages.
Case report: In this report, we describe the case of an 88-year-old Caucasian man, an ex-smoker with chronic alcohol abuse and high-grade urothelial carcinoma, who developed upper gastrointestinal bleeding and anemia in December 2021. Upper gastrointestinal endoscopy revealed an ulcer-vegetative lesion next to the pylorus, confirmed pathologically as gastric carcinoma. A staging thoracic-abdominopelvic computed tomography scan excluded distant metastatic disease or other suspicious lesions. In February 2022, he underwent a sub-total distal gastrectomy with a Billroth type-2 anastomosis without complications. In the postoperative period, he developed pneumonia from which he recovered with antibiotics. The pathological examination identified an ulcer-infiltrative lesion in the antrum, infiltrating the gastric wall to the serosal layer, classifying it as a gastric adenosquamous carcinoma (pT4aN0R0).
Conclusion: ASC represents a rare histological type of gastric carcinoma, especially in Western populations. The etiopathogenesis of this tumor remains incompletely understood and has a poor prognosis because presents at advanced staging and with frequent venous and lymphatic invasion. So, clinicians should be aware of this type of gastric carcinoma so as not to delay diagnosis and treatment, reducing survival.
INTRODUCTION
Gastric cancer (GC) persists as the second leading cause of cancer-related mortality globally and is concurrently identified as the fifth most frequently diagnosed cancer (1). In 2020, GC accounted for over one million new cases and an estimated 770,000 deaths (2).
Among the various pathologic types of GC, adenocarcinoma (AC) is the most common, whereas the incidence of adenosquamous carcinoma (ASC) is extremely low, accounting for less than 1% of total gastric malignancies (3). There are fewer than one hundred published cases in the literature, with the first documented by Rolleston and Trevor in 1905 (4). Due to the rarity of ASC, existing knowledge is primarily derived from case reports and case series with a small number of patients, which have been insufficient in drawing conclusions regarding the histogenesis, clinicopathologic characteristics, optimal treatment strategies, and prognosis.
Although previous studies have shown that primary gastric ASC demonstrates early tumor progression and poorer prognosis compared to typical gastric AC, the available data remain sparse and inconclusive (1). Gastric ASC tends to have a higher prevalence in men particularly in Asian populations, and typically presents at advanced stages (5). In this paper, we present a rare case of gastric ASC in a Caucasian man.
CASE REPORT
We describe a case of an 88-year-old Caucasian man, with a previous history of arterial hypertension, overweight, chronic alcohol abuse, ex-smoker, chronic kidney disease, and degenerative joint disease. Regarding prior malignancies, he underwent a trans-urethral resection of bladder tumor and intravesical Bacillus Calmette-Guérin (BCG) therapy for a high-grade pT1 urothelial carcinoma in 2014.
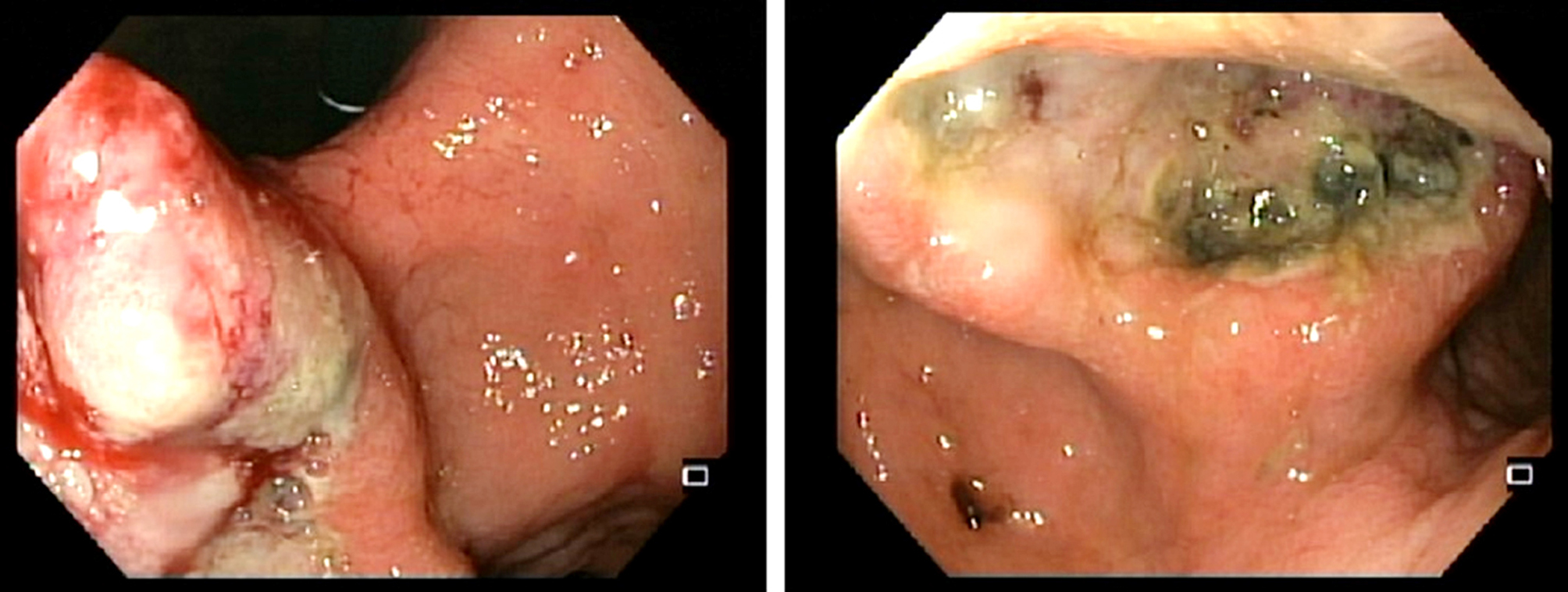
In December 2021, he came to the emergency department of our hospital with hematemesis and melena. On arrival, he was pale, underweight, asthenic, and the abdominal examination was painless and without palpable masses. The laboratory tests revealed a hemoglobin of 95 g/L and acute kidney injury classified as AKIN 1. Upper gastrointestinal endoscopy revealed an ulcer-vegetative lesion next to the pylorus, without reaching the cardia, and with a clot but without active bleeding (fig. 1). Lesion biopsy confirmed the diagnosis of gastric carcinoma.
Figure 1 - On the anterior surface of the distal antrum, there is an ulcerative-vegetative neoformation with hematic pigment, but without active hemorrhage. The lesion is located near the pylorus without involving it and does not reach the cardia.
A staging thoracic-abdominopelvic computed tomography scan identified a 28 mm ulcerative lesion in the greater curvature of the gastric antrum, with no serosal extension and no evidence of distant metastatic disease or other suspicious lesions (cT3-4N0M0). The patient was discharged after 10 days, with no gastro-intestinal bleeding, no need for blood transfusions, stabilized renal function, and awaiting treatment decision by the oncology surgery group.
In February 2022, the patient underwent a sub-total distal gastrectomy with a Billroth type-2 anastomosis, without complications. Postoperatively, he developed pneumonia, which resolved with antibiotic therapy. Discharged after one month on a soft diet and symptom-free.
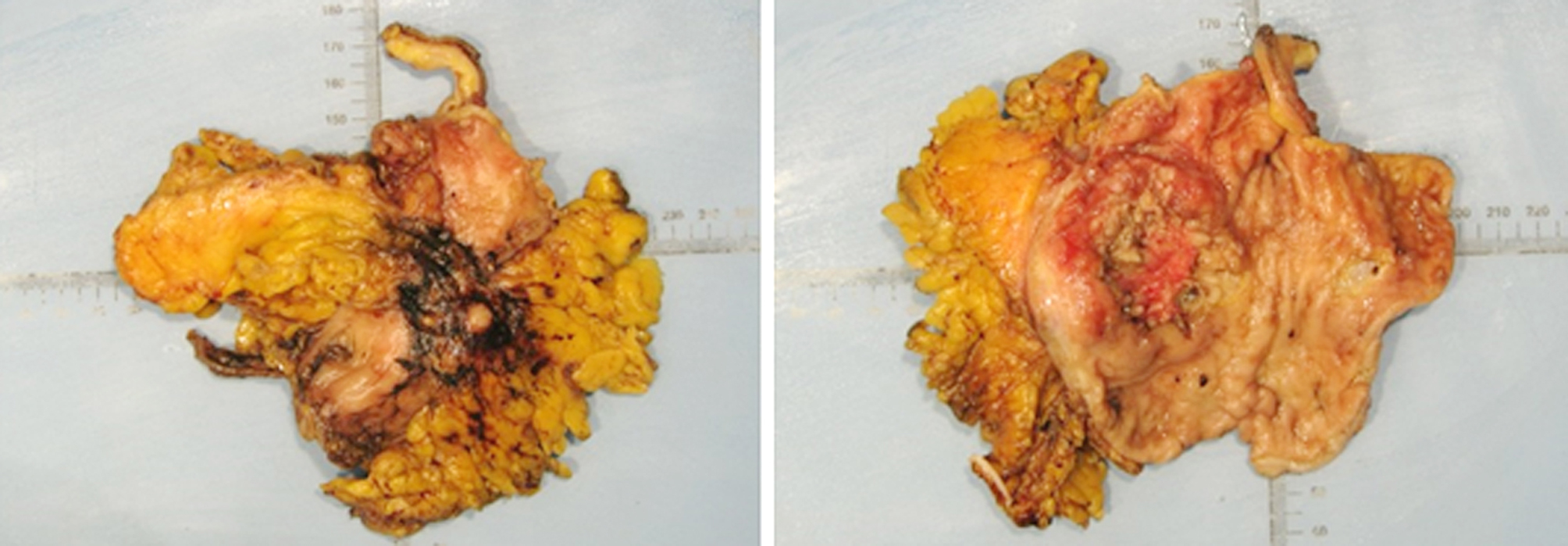
The macroscopic examination revealed an ulcer-infiltrating neoplasm that develops in the antrum/ pyloric canal and the histological examination identified gastric adenosquamous carcinoma. The tumor invaded the serosa, but without metastatic involvement in the sixteen identified lymph nodes and tumor-free surgical margins. No lymphatic or perineural invasion or peritoneal implants were observed, although venous invasion was confirmed. The remaining gastric mucosa exhibited changes consistent with low-grade dysplasia and chronic atrophic gastritis with intestinal metaplasia (pT4aN0M0R0, stage IIB) (fig. 2).
Figure 2 - An ulcer-infiltrating tumor is observed in the lower third stomach (antrum/pylorus), measuring 4.7 x 5.5 x 1.2 cm. There was no invasion of the margins, lymphovascular invasion, or lymph node metastasis (0/16).
At the 6 months follow-up, the patient remained asymptomatic and in good health.
DISCUSSION
Gastric ASC is a rare and aggressive histological type of gastric carcinoma, accounting for less than 1% ofgastric cancer (3, 6-8). The ASC is a mixed neoplasia, and the diagnosis requires the coexistence of an adenocarcinoma and squamous cell components, the latter must be present in > 25% of the primary tumor (3,7, 10). Faria et al. added that the ASC should be outside the cardia, without esophageal involvement and adenosquamous carcinoma in other organs (9).
Gastric ASC is more prevalent in men (male-to-female ratio 4:1), especially in Asian populations, and it peaks in the sixth decade of life (5,9). ASC is most frequently located in the lower third – the distal stomach (antrum/pylorus) (3,7), although some studies suggest upper third lesions, with limited patient inclusion (7). Clinical presentations of gastric ASC can resemble those of other gastric cancers, including epigastric pain, dysphagia, acid regurgitation, nausea, and vomiting (6,8). Li et al. suggested that the SCC component in gastric ASC grows faster and invades deeper, leading to advanced disease and complications such as ulcers and hemorrhages (6). As demonstrated in this clinical case, the presentation of ASC in our patient is upper gastrointestinal bleeding.
Some previous studies report that the biological behavior and prognosis are determined by the adenocarcinoma component (6). Although the SCC component is theoretically more aggressive, the AC component seems to play a more critical role, even in the minority within the primary tumor (6). The AC component is predominantly present in hematogenous and hepatic metastases (10). However, ASC exhibits characteristics associated with a worse prognosis, such as poorer differentiation, advanced staging at diagnosis, lymphovascular invasion, synchronous and meta-chronous lymph node involvement, and distant metastasis (3,6,8). The diagnosis is usually accompanied by distant metastasis, especially to the liver and peritoneum (3,8).
The etiopathogenesis of this tumor remains incompletely understood and controversial. Five hypotheses have been proposed for its origin: 1) squamous metaplastic transformation of AC; 2) oncogenic transformation of ectopic squamous epithelium; 3) cancerization of metaplastic squamous epithelium in the gastric mucosa; 4) collision of AC and SCC; and 5) stem cell of the gastric mucosa that differentiated toward both cellular lines (3,8,9). Currently, the first hypothesis is favored by many scholars due to 1) the majority of the SCC component is located in the deep layers, unlike the AC; 2) the ASC presents an obvious area of transition between the two components; 3) the positiveexpression of CK7 and CEA in the SCC component and 4) the identical levels of the p53 gene in both components (3,8).
Standard treatment for ASC gastric cancer has not yet been established, however, as with most solid tumors, radical surgery with curative intent remains the best treatment for local disease without distant metastases (3,6,8). Despite complete surgical resection (R0), most patients experience rapid deterioration within a few months postoperatively (8). Chemotherapy remains the primary treatment for advanced disease but may not improve survival for patients undergoing potentially curative surgery (6). Some studies state that radiotherapy could also be used as an adjuvant treatment since the SCC component of gastric ASC would be theoretically sensitive (3). However, due to the more accepted histogenesis, treatment should focus on the AC component, potentially explaining why radiotherapy was not clinically effective in previous studies (6). Cheng-Han Wu et. al. demonstrated that, compared to other histological subtypes, gastric ASC has a higher proportion of positive surrogate biomarkers in immunotherapy (11). Thus, immunotherapy may be a treatment of choice for patients with gastric ASC, especially for those with a high positivity rate of prediction markers in the tumor (11).
In this clinical case, there is a gastric ASC located in the antrum/pylorus, with invasion of the serosa. However, it does not spread to the lymph nodes or adjacent organs, thus classifying it as pT4aN0M0. Since the standard treatment had not yet been defined, the patient was proposed for primary surgery with curative intent, and an R0 resection was possible. Following the surgery, the decision of the oncology group was to maintain clinical and analytical surveillance. In the literature, it is evident that overall survival (OS) at 3 years ranges from 15.4% to 32.4% (3,8), and the median OS varies between 9.9 and 22 months (5,8). Limited research has been conducted to identify prognostic factors for gastric ASC. In a study by Feng et al., which involved 109 gastric ASC patients, it was reported that invasion depth and TNM stage are significantly related to OS (3).
CONCLUSIONS
In conclusion, we present a rare clinical case of gastric adenosquamous carcinoma with serosal invasion but without local or distant metastasis in a Caucasian man. Due to the rarity of this entity and, consequently, the limited number of retrospective studies, established guidelines for screening and treatment are still lacking. Therefore, centralized, and collaborative large-sample investigations are necessary to characterize this aggressive tumor and optimize the treatment plan.
Conflict of interest and source of funding
All authors declare no sources of funding received for the research and no conflicts of interest.
Ethical approval
For this case, ethical approval was obtained.
Author’s contributions
All authors had been actively involved in the reported case and took full responsibility for the content of this article.
REFERENCES
1. Chu YX, Gong HY, Hu QY, Song QB. Adenosquamous carcinoma may have an inferior prognosis to signet ring cell carcinoma in patients with stages I and II gastric cancer. World J Gastrointest Oncol. 2020;12(1):101-12.
2. Morgan E, Arnold M, Camargo MC, Gini A, Kunzmann AT, Matsuda T, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020-40: A population-based modelling study. EClinicalMedicine. 2022;47:101404.
3. Feng F, Zheng G, Qi J, Xu G, Wang F, Wang Q, et al. Clinicopathological features and prognosis of gastric adenosquamous carcinoma. Sci Rep. 2017;7(1):4597.
4. Ajoodhea H, Zhang RC, Xu XW, Jin WW, Chen K, He YT, et al. Fever as a first manifestation of advanced gastric adenosquamous carcinoma: a case report. World J Gastroenterol. 2014;20(29):10193-201.
5.Akce M, Jiang R, Alese OB, Shaib WL, Wu C, Behera M, et al. Gastric squamous cell carcinoma and gastric adenosquamous carcinoma, clinical features and outcomes of rare clinical entities: a National Cancer Database (NCDB) analysis. J Gastrointest Oncol. 2019; 10(1):85-94.
6.Li HS, Liu X, Zhang MY, Cheng K, Chen Y, Zhou YW, et al. Clinicopathologic characteristics, survival, and treatments for gastric adenosquamous carcinoma: a population-based study. Curr Oncol. 2020;27(6):e527-e36.
7.Ge Y, Lin L, Ma X, Luo D, Shi L, Jiang M, et al. Adenosquamous Carcinoma of the Stomach: A Population-based Study from the SEER Database. J Cancer. 2019;10(23):5705-13.
8.Chen H, Shen C, Yin R, Yin Y, Chen J, Han L, et al. Clinicopathological characteristics, diagnosis, treatment, and outcomes of primary gastric adenosquamous carcinoma. World J Surg Oncol. 2015;13:136.
9.Faria GR, Eloy C, Preto JR, Costa EL, Almeida T, Barbosa J, et al. Primary gastric adenosquamous carcinoma in a Caucasian woman: a case report. J Med Case Rep. 2010;4:351.
10.Chen YY, Li AF, Huang KH, Lan YT, Chen MH, Chao Y, et al. Adenosquamous carcinoma of the stomach and review of the
literature. Pathol Oncol Res. 2015;21(3):547-51.
11. Wu CH, Lai CL, Teng CJ, Fang WL, Huang KH, Fen-Yau Li A, et al. Immunoprofile of adenosquamous carcinoma in gastric cancer. J Chin Med Assoc. 2023;86(6):542-8.
Full Text Sources:
Abstract:
Views: 2760

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.