Surgery, Gastroenterology and Oncology
|
|
Inguinal hernia is a common surgical condition worldwide and involves protrusion of an organ or its fascia through the abdominal wall. The hernia contents may include omentum, colon, small bowel, or its mesentery, while less common contents such as the appendix, ovary, or fallopian tube can also be present. Amyand’s hernia, in which the appendix is found within the sac, is one such rare form. We present a case of a 48-year-old male with a long-standing history of reducible right inguinal hernia who presented with acute onset right inguinal scrotal pain requiring emergency open right hernioplasty. All preoperative investigations were unremarkable.Intra-operatively, the hernia contained the caecum, appendix, and terminal ileum. These structures were contused. The appendix was not inflamed and was not removed. The operation was completed with a simple right hernioplasty without appendicectomy. The patient was well postoperatively and was discharged on postoperative day one without any morbidity.
INTRODUCTION
Surgery for an inguinal hernia is one of the most common operations worldwide. Prevalence varies in the infant and elderly populations. Healthcare centers have increased in number over the years, making surgery more accessible. The operation can be elective or performed in an emergency, depending on the state of the hernia. A few surgical methods can be used: herniotomy, herniorrhaphy, or hernioplasty.
The diagnosis of an inguinal hernia is most often made by clinical examination. Rarely, imaging is required. Proper physical examination is usually sufficient. Imaging is useful when further assessment is needed. For example, in a giant inguinal hernia, a CT scan may be needed. It helps assess the contents, the defect size, and other concurrent pathology. This information helps the surgeon decide the surgical approach.
The hernia content cannot always be established preoperatively by physical examination. Most often, the contents are examined intraoperatively. Common contents include omentum, colon, and small bowel. Surgeons also encounter uncommon content, such as the ovary, bladder, fallopian tube, or appendix.
Amyand’s hernia is an uncommon variation of inguinal hernia. The appendix is found as the content of the sac. It was first described by C. Amyand in 1735 in an 11-year-old boy. The child was initially diagnosed with an incarcerated inguinal hernia. Intraoperatively, the appendix was found to have perforated within the hernia sac (1). After that, cases with the appendix in the hernia sac are named Amyand’s hernia. It is extremely rare, accounting for about 1% of all inguinal hernia patients (2-5).
The appendix within the sac can be either inflamed or normal. When inflamed, it typically presents as persistent pain in the inguinal region, and blood tests may show elevated septic markers. However, there are no proper guidelines for managing an inflamed appendix during Amyand’s hernia surgery. Instead, a few case reports describe how surgeons handle Amyand’s hernia with an inflamed appendix intra-operatively (6,7).
CASE PRESENTATION
A 48-year-old male with no underlying comorbidities presented to the surgical outpatient department. He was referred by a general practitioner for a symptomatic right inguinal hernia. He complained of right inguinal swelling for two months. The swelling was associated with on-and-off discomfort, especially when standing or walking. It was reducible. There was no history of heavy lifting, gym activities, lower urinary tract symptoms, or chronic cough. He smokes one pack per day. His job does not involve heavy lifting.
Clinical examination demonstrated a reducible, soft, and non-tender right inguinal hernia with a positive cough impulse. There were no skin changes and all other examinations were unremarkable.
An elective surgery was scheduled for two weeks after his initial clinic visit, and he was referred for pre-operative assessment in the anesthetics clinic, which was uneventful.
Two days before surgery admission, he developed sudden severe pain over the right inguinal swelling. The swelling became irreducible. He sought emergency department care. There was no clear aggravating factor for the pain. His pain score was 7 out of 10. He had no vomiting, no increased abdominal distension, no urinary tract symptoms, and no recent trauma. He could pass motion but reported minimal flatus.
On general examination, he appeared comfortable. Vital signs were normal. Physical examination showed an irreducible right inguinal swelling, about the size of a fist. It was mildly tender, soft, without skin changes, and with no bowel sound within the swelling. His abdomen was soft and not distended. Bowel sound was not hyperactive. Abdominal x-ray showed no dilated bowel (fig. 1). Blood parameters were normal. He was diagnosed with an irreducible right inguinal hernia and admitted for emergency right hernioplasty.
Figure 1 - Pre-operative abdominal x-ray

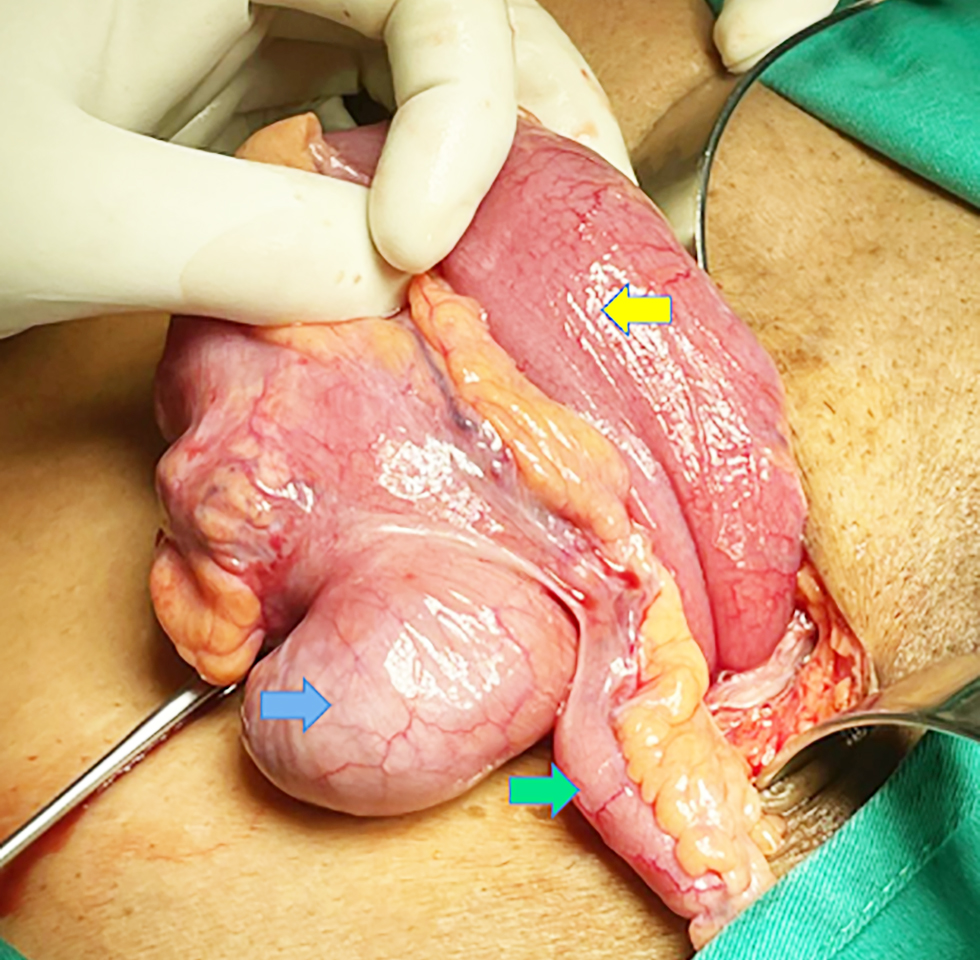
He underwent emergency open right hernioplasty the next day after adequate fasting. IV cloxacillin 1g stat was given on induction as prophylaxis. The operation was performed under spinal anesthesia. Intraoperatively, it was an irreducible indirect right inguinal hernia. The hernia contained the caecum, a small portion of contused small bowel, and a non-inflamed appendix (fig. 2). The fluid within the sac was straw-colored. The terminal ileum was also examined, but was unremarkable. All hernia contents were reduced into the abdominal cavity. The proximal sac was closed by the purse-string method using Vicryl 2/0. The distal sac was left within the scrotal sac, after ensuring hemostasis. Polypropylene mesh (15 by 7cm) was used and fixed with Prolene 3/0 to the conjoint tendon and inguinal ligament below the external oblique aponeurosis. The skin was closed in a subcuticular manner after closing the external oblique aponeurosis. The operation was uneventful. He recovered well post-operatively and was discharged the following day without any early postoperative complications. He was discharged from the surgical outpatient clinic three months after the operation. At follow-up, there was no recurrent hernia.
Figure 2 - Contents of the inguinal hernia sac, which includes the caecum (blue arrow), appendix (green arrow), and terminal ileum (yellow arrow)
DISCUSSION
Few studies have examined the best way to manage inguinal hernia. There are no proper guidelines for the exact management of inguinal hernia. Different centers practice differently.
A recent study by Gao detailed several strategies for managing inguinal hernia (8), which helps practitioners develop ideas for intraoperative management.
According to the retrospective study, total of six patients were included and analyzed. Each of them received different surgical approaches based of their clinical condition of appendix found during surgery. In general, non-inflamed appendix were not removed intraoperatively. This is similar to our case study as well, whereby normal appendix was left behind during surgery.
The condition of appendix when it is found within the hernia may be either inflamed or normal. There is no specific study to validate the definite management of normal or inflamed appendix found during Amyand’s hernia surgery. This is most probably due to its rare occurrence among inguinal hernia cases. Hence, not enough number of cases are available to be analysed and compared statistically.
Available published material regarding Amyand’s hernia nowadays mostly came from case reports (9,10). They described experience of medical centers engaging the situation when they are dealing with Amyand’s hernia intraoperatively. Some centers are lucky enough to have been able to perform CT prior surgery.
A systematic review recently mentioned that CT is the sole diagnostic imaging in diagnosing Amyand’s hernia preoperatively (11). CT is more superior compared to ultrasonography.
However, sometimes Amyand’s hernia on CT can be missed since the density of small bowel and appendix is hard to be differentiated. Ultrasound might be helpful in preoperative setting. However, its sensitivity depends on the operator. It is almost impossible to diagnose Amyand’s hernia solely by physical examination preoperatively, as presentation is very similar to classical inguinal hernia. Therefore, some medical practitioners believe that the best way to diagnose Amyand’s hernia is during intraoperative. In our case report, we did not perform neither ultrasound nor CT prior surgery as the patient presented with symptomatic irreducible inguinal hernia and the surgery need to be perform as emergency. In this case, ultrasound or CT might not change the subsequent management for this patient.
The pathogenesis of Amyand’s hernia remains poorly understood. Amyand’s hernia can be grouped into four types based on the patient’s clinical condition at presentation and the appendix’s intraoperative condition (table 1) (12). For type 1 Amyand’s hernia, a normal appendix is to be found within the hernia sac. Whilst in type 2 Amyand’s hernia, the appendix found within the hernia sac is inflamed and only confined to the sac. As for type 3 Amyand’s hernia, the appendix within the hernia sac is not only inflamed, but it has already perforated or caused abdominal wall or peritoneal infection. Finally, for type 4 Amyand’s hernia, the inflamed appendix within the hernia sac is related to other abdominal pathology.
Table 1 - Four types of Amyand’s hernia
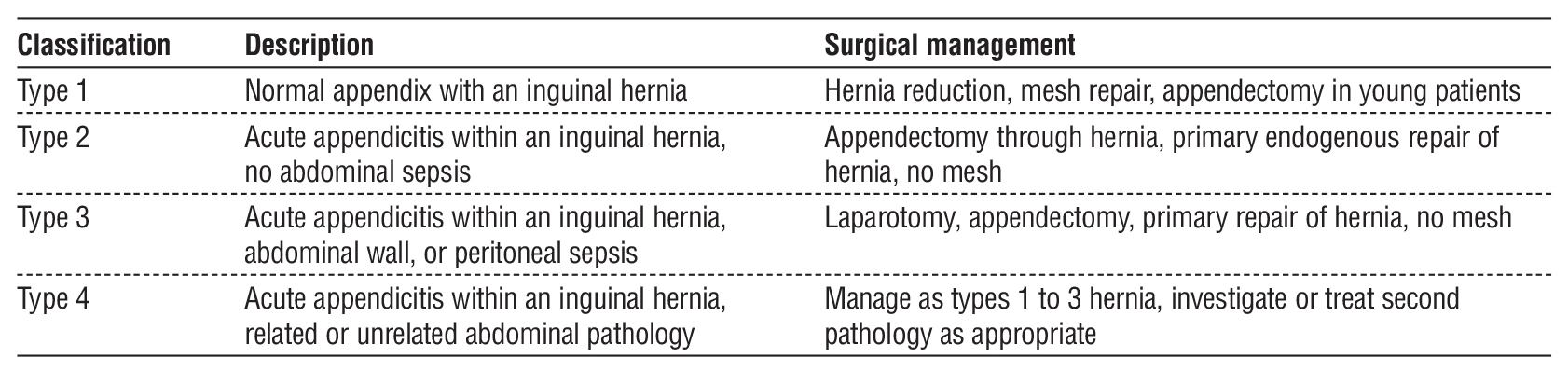
In our case report, the patient was found to have Type 1 Amyand’s hernia, whereby he was managed similarly to simple inguinal hernioplasty. His appendix was not removed in view of his presenting age; it is uncommon to get acute appendicitis as compared to adolescents. Furthermore, we did not want to take a risk of mesh infection following appendicectomy. Some case reports by other centers practice the removal of the appendix during surgery despite a normal-looking appendix. The outcomes were promising as none of the patients developed any complications following surgery. No mesh infection or sepsis was reported postoperatively in their studies (9,10).
Furthermore, the intact appendix during hernia surgery can be later on used for other surgery such as urinary diversion tract surgery or extrahepatic biliary tract surgery (6,7).
Several measures can be done to prevent mesh infection post-operatively following Amyand’s hernia repair with appendicectomy. Routinely, all surgeons administer prophylactic antibiotics prior to skin incision. It is advisable to thoroughly wash the wound bed after securing the appendix stump before fixing the mesh. The use of antibiotics postoperatively may help reduce the risk of infection. However, no specific study has determined its efficacy. We believe that the decision for post-operative antibiotics mostly depends on the operating surgeon.
CONCLUSION
Amyand’s hernia is an uncommon type of inguinal hernia, for which making a preoperative diagnosis is often difficult. Preoperative CT and ultrasound might be helpful, but the diagnosis is best made during intraoperative. The management of Amyand’s hernia should be guided by the patient’s clinical condition and the specific type of hernia present. It is not advisable to perform an appendicectomy on a white appendix if mesh is to be implanted.
Large-scale studies are needed to evaluate the relationship between mesh application and the risk
of infection following appendicectomy in Amyand’s hernia repair.
Conflict of Interests
There is no conflict of interest for this case report.
Ethics of Approval
Ethical approval was waived by the local ethics committee, as this is a case report and does not require ethical approval, and the procedures performed were routine and part of standard practice.
REFERENCES
1. Amyand C. Of an inguinal rupture, with a pin in the appendix coeci, incrusted with stone; and some observations on wounds in the guts. Phil Trans R Soc Lond. 1735;39: 329-42.
2. Mewa Kinoo S, Aboobakar MR, Singh B. Amyand’s Hernia: a serendipitous diagnosis. Case Rep Surg. 2013;2013:12509.
3. Morales-Cárdenas A, Ploneda-Valencia CF, Sainz-Escárrega VH, Hernández-Campos AC, Navarro-Muñiz E, López-Lizarraga CR, et al. Amyand hernia: Case report and review of the literature. Ann Med Surg (Lond). 2015;4(2):113-5.
4. Hiatt JR, Hiatt N. Amyand’s hernia. N Engl J Med. 1988;318(21): 1402.
5. Okur MH, Karaçay S, Uygun I, Topçu K, Öztürk H. Amyand’s hernias in childhood (a report on 21 patients): a single-centre experience. Pediatr Surg Int. 2013;29(6):571-4.
6. Martín NS, Guillermo MM, Rodney S, Rodrigo VC, Matías RM, Carolina TZ, et al. Hernia de Amyand: presentación de un caso y revisión de la literatura. Revista Chilena De Cirugía. 2007;59(2):142–4.
7. Ofili OP. Simultaneous appendectomy and inguinal herniorrhaphy could be beneficial. Ethiop Med J. 1991;29(1):37-8.
8. Gao Y, Zhang T. Amyand’s hernia: a 10-year experience with 6 cases. Gao et al. BMC Surg (2021) 21:315
9. Widiono ES, Mulyasari PD, Kurniawan R, Tambunan CA, Suhono U. A male patient with amyand hernia: A case report and literature review. Indian J Case Reports. 2023;9(3):68-70.
10. Aldosari DM, Alaboon NK, Mojammami MY, Aqeeli MO, Aldhafeeri OA, Theban AA, et al. Inguinal Hernia Containing an Inflamed Appendix: A Case of Amyand Hernia. Cureus. 2022;14(1):e21121. Retraction in: Cureus. 2024;16(1):r126.
11. Papaconstantinou D, Garoufalia Z, Kykalos S, Nastos C, Tsapralis D. Implications of the presence of the vermiform appendix inside an inguinal hernia (Amyand’s hernia): a systematic review of the literature. Hernia. 2020;24(5):951
12. Losanoff JE, Basson MD. Amyand hernia: a classification to improve management. Hernia. 2008;12(3):325–6.
Full Text Sources:
Abstract:
Views: 274

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.