Surgery, Gastroenterology and Oncology

|
|
Introduction: Anorectal cancer (ARC) associated with Crohn’s disease (CD) is a rare but serious complication, with limited data available in the literature. Objective: To evaluate the incidence and clinical characteristics of ARC in patients with CD.
Methods: A systematic review was conducted following PRISMA guidelines. A PubMed search (2014–2024) identified studies using the keywords “anorectal cancer”, “Crohn’s disease”, and “inflammatory bowel disease”. Articles in English and Portuguese, or with an English abstract containing extractable data, were included. Variables analyzed included age at diagnosis, tumor type, fistula characteristics, symptoms, treatment, and survival. Study quality was assessed using the Newcastle-Ottawa Scale.
Results: Eight studies (6 retrospective, 2 case reports) with 87 patients were included. ARC incidence among CD patients ranged from 0.54% to 0.8%. Most cases occurred in males (61.2%) with early CD diagnosis (mean age 21–25.5 years). ARC was diagnosed at a mean age of 46.7 years, with a mean interval of 25.6 years from CD diagnosis. Tumors were mainly adenocarcinomas (52.6%–85.7%). Diagnosis often followed biopsy of asymptomatic chronic perianal fistulas (47.4%–81.3%). Metastasis was present at diagnosis in 36.8%. Most patients underwent radical surgery. Recurrence occurred in 35.7%, and overall survival was 68.3%.
Conclusion: ARC in CD is rare but aggressive. Early diagnosis is challenging, especially in chronic perianal fistulas. Prolonged surveillance and effective screening are crucial.
INTRODUCTION
The reported incidence of cancer among patients with Crohn’s disease (CD) ranges between 0.6% and 3.1% in Western countries; however, anorectal cancer (ARC) arising in association with CD represents a rare and distinct complication that remains insufficiently characterized in the literature (1,2,3). Only a limited number of case series have documented sporadic occurrences of perianal carcinoma developing within Crohn’s - related fistulas, resulting in the absence of clear recommendations for screening and management of patients at risk (4,5).
Given that anal and perianal manifestations of Crohn’s disease are frequently accompanied by chronic inflammation of the rectal mucosa, individuals with long-standing anal and/or perianal CD may also carry an elevated risk of developing rectal carcinoma (6,7,8).
Despite advances in the understanding and management of Crohn’s disease, there remains a lack of standardized recommendations for surveillance and early detection of anorectal carcinoma in this high-risk population. This review therefore seeks not only to summarize the available epidemiological evidence but also to highlight clinical patterns and outcomes that may guide early diagnosis and treatment strategies in patients with concomitant ARC and CD (9,10,11).
MATERIALS AND METHODS
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
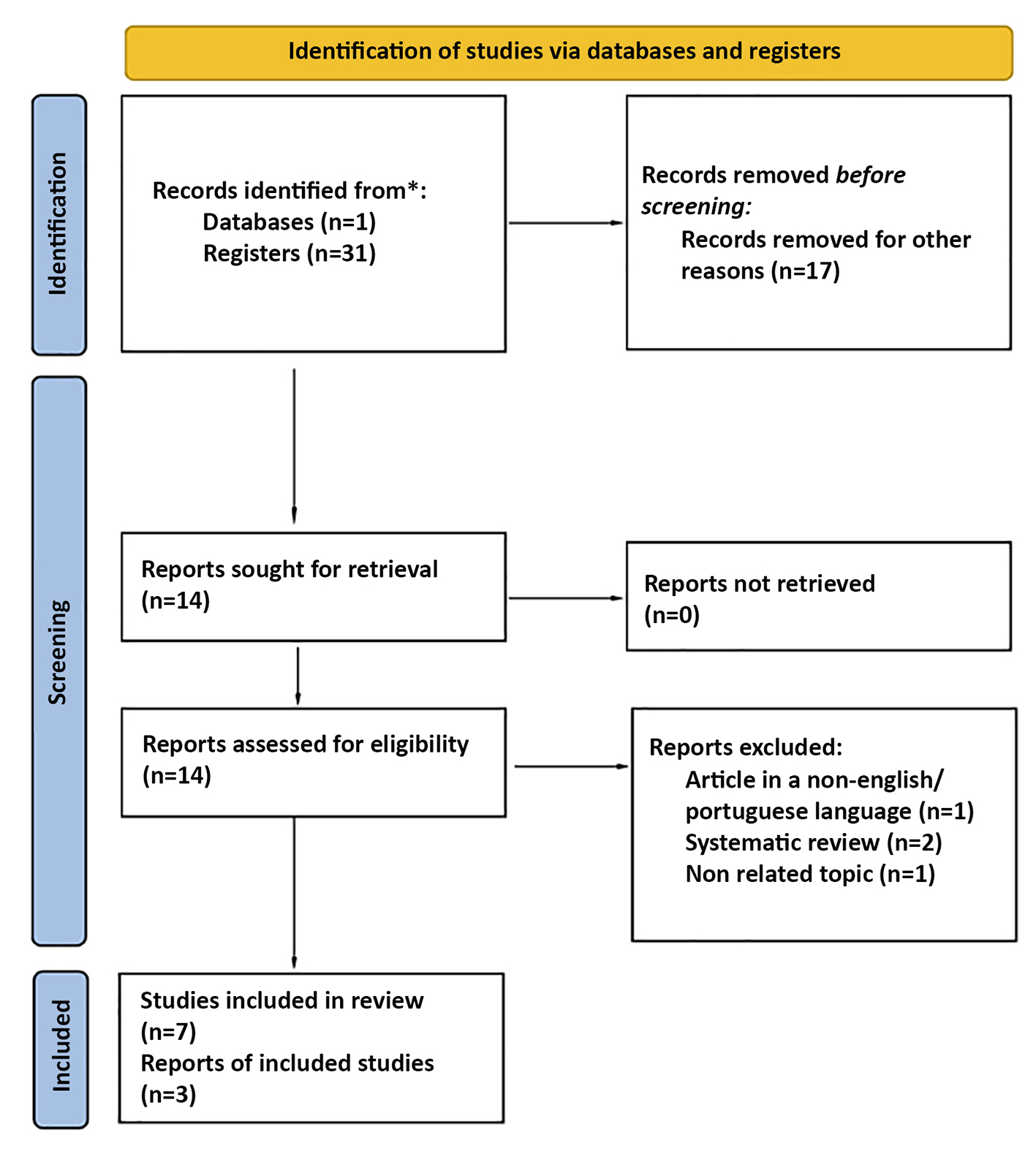
A bibliographic search was performed on the PubMed database over the last ten years (from 2014 to October 2024), using the keywords “anorectal cancer”, “Crohn’s disease”, and “Inflammatory bowel disease”. Articles in Portuguese and English were included. Articles in other languages were also included if an English abstract with extractable data was available. Additionally, the reference lists of each selected study were analyzed individually to identify potentially eligible studies through cross-referencing. Exclusion criteria comprised review articles, editorials, studies lacking extractable clinical data, and those focusing exclusively on colorectal cancer without specific reference to anorectal involvement. During the selection process, duplicate articles were removed, and studies not meeting the inclusion criteria after full-text review were excluded. A total of 31 records were initially identified, of which 23 were excluded based on title, abstract, or data insufficiency, resulting in 8 studies meeting the inclusion criteria for final analysis.
The variables analyzed included age at CD and ARC diagnosis, interval between fistula and ARC, sex, family history, tumor type, fistula type, symptoms, treatment, and survival rates.
Study Quality Assessment
The methodology and risk of bias of the studies were systematically evaluated by two independent reviewers.
Study quality was assessed using the Newcastle-Ottawa (NO) scoring tool (table 1). Total scores ranged from 0 (worst) to 9 (best), with a score ?6 indicating high quality.
Table 1 - Newcastle-Ottawa Scale
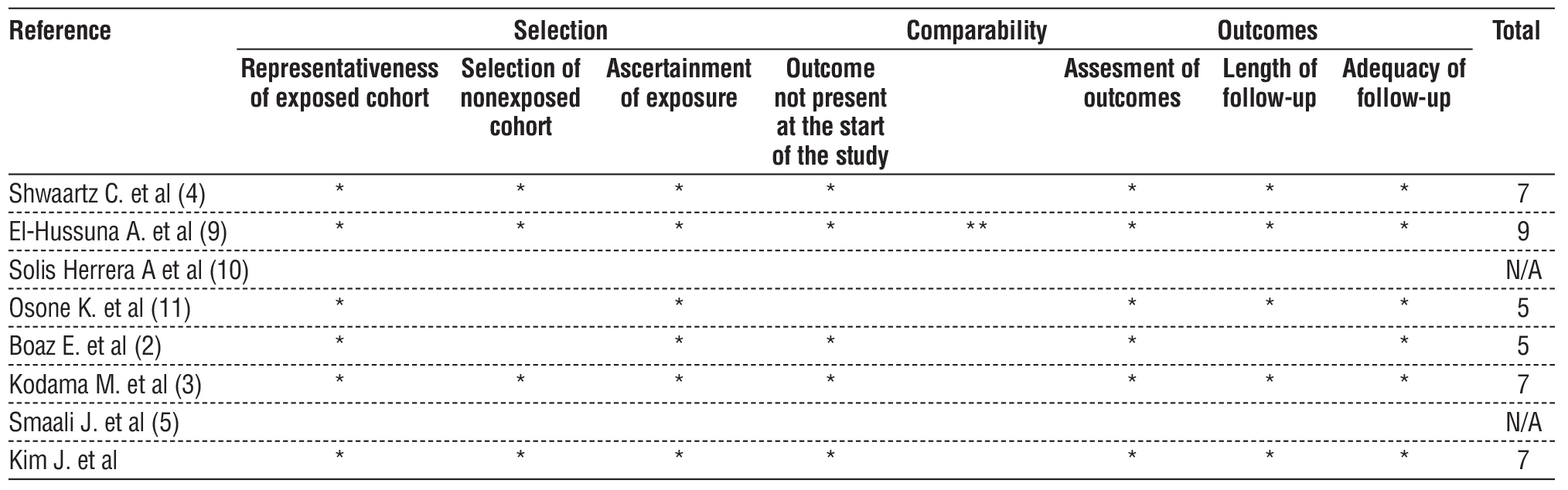
Discrepancies between reviewers were resolved through discussion. In the case of persistent disagreement, a third reviewer was consulted.
Statistical Analysis
Analysis was performed using Medcalculate and Stats to Do software. Continuous variables were expressed as mean and standard deviation, and categorical variables were described as percentages with 95% confidence intervals.
RESULTS
Out of 31 articles, 8 were included [6 retrospective observational studies and 2 case reports (2-8)], com-prising a total of 87 patients with CD and ARC (fig. 1).
Figure 1 - Study Selection Flow Chart
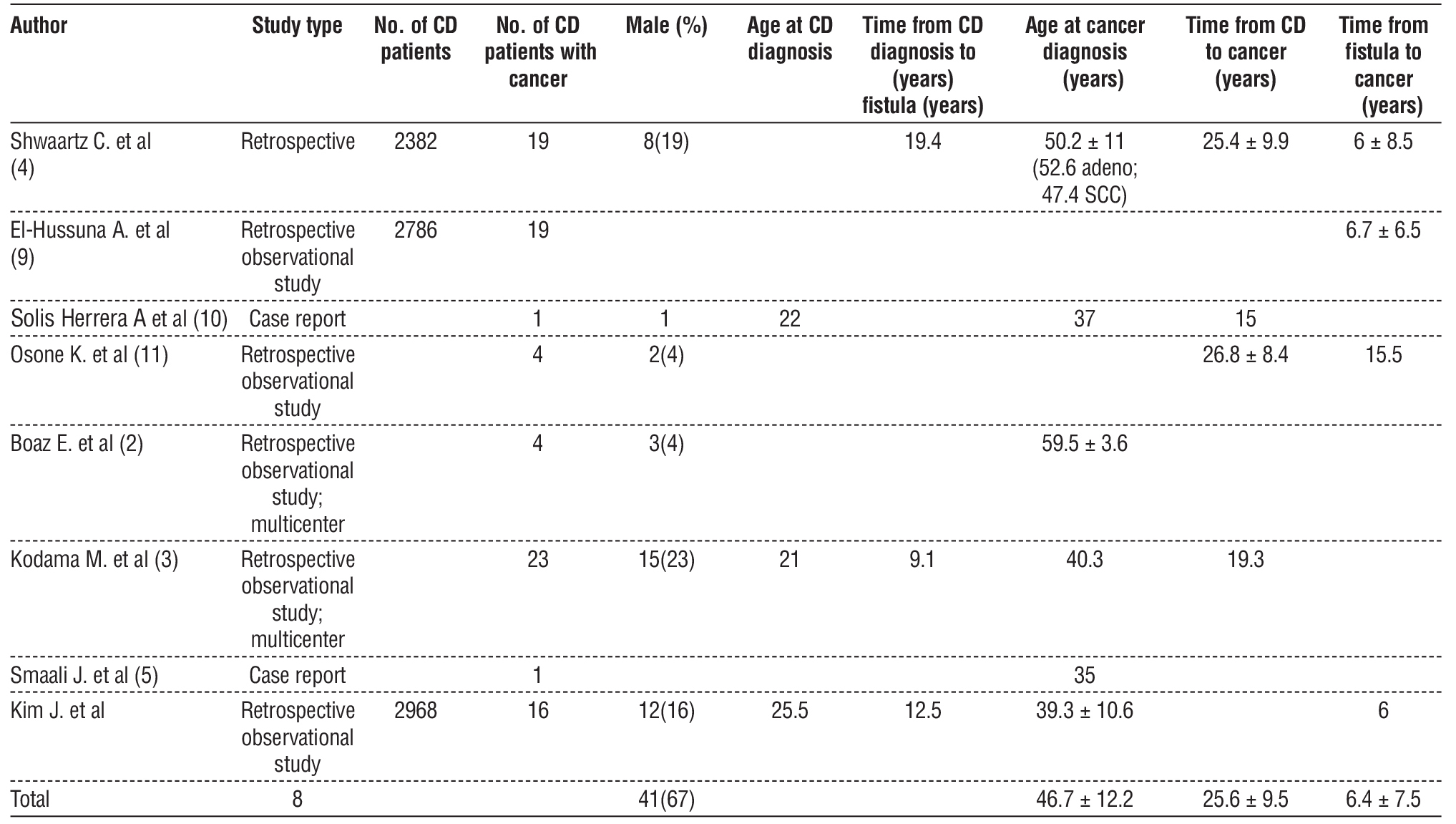
The incidence of ARC in CD patients ranged from 0.54% to 0.8%. ARC occurred more frequently in men (61.2%) and was associated with early CD diagnosis (21–25.5 years). The mean age at ARC diagnosis was 46.7 ± 12.2 years, and the mean interval between CD and ARC diagnosis was 25.6 ± 9.5 years (table 2).
Table 2 – Population demographics
The included studies demonstrated heterogeneity regarding study design, sample size, and geographic distribution. Most were retrospective single-center studies conducted in tertiary care hospitals across Europe and Asia. The total sample of 87 patients reflects the rarity of ARC in the context of CD, yet consistent clinical patterns emerged. In nearly all studies, the presence of chronic perianal fistulas preceded the diagnosis of cancer by more than two decades, and mucinous or tubular adenocarcinomas were the predominant histologic subtypes. These findings reinforce the hypothesis that chronic inflammation and epithelial regeneration within long-standing fistulous tracts contribute to carcinogenesis.
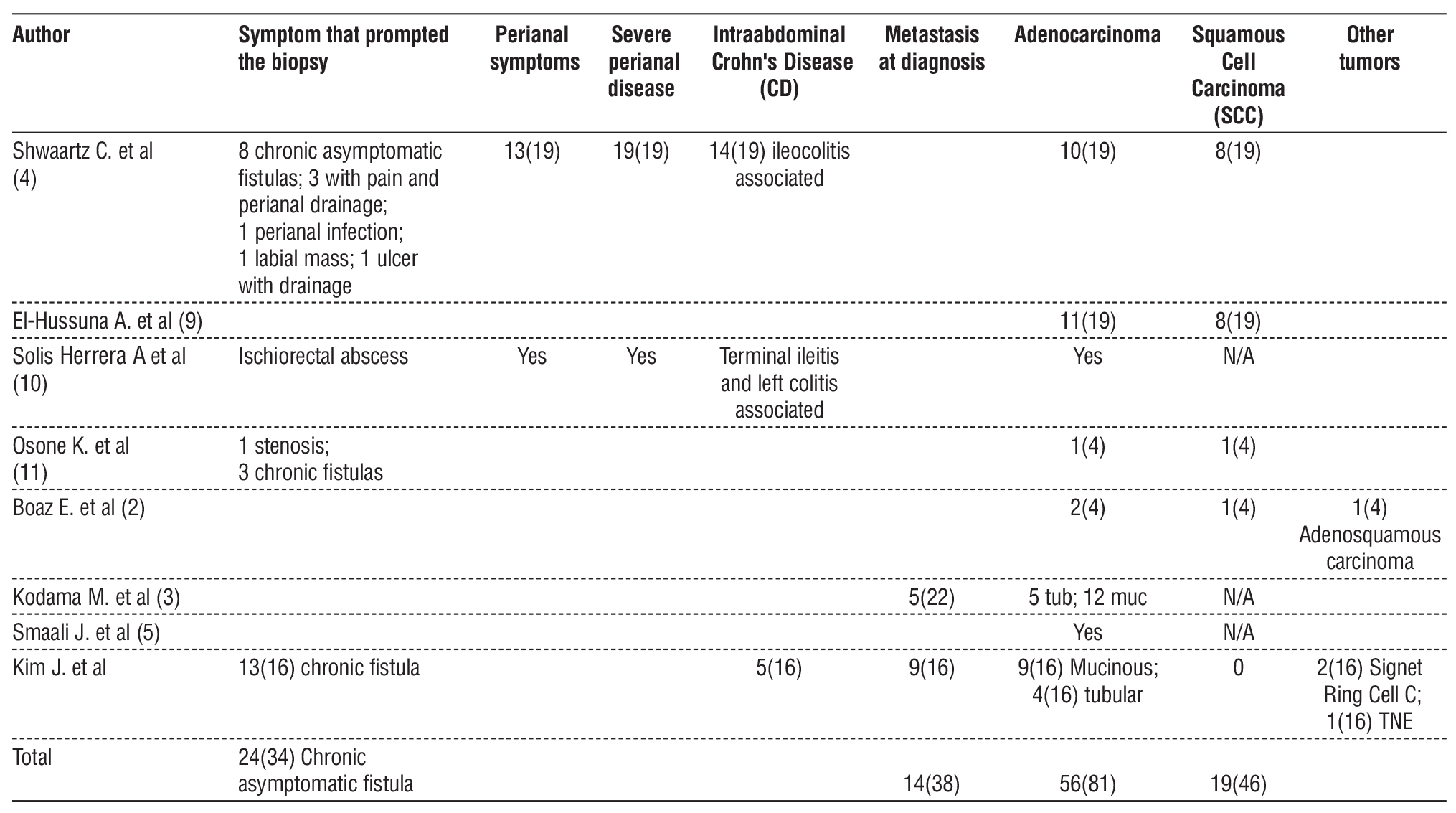
Most patients underwent biopsy in the context of an asymptomatic chronic fistula (47.4% – 81.3%). At diagnosis, 36.8% had metastases. The majority of tumors were adenocarcinomas (52.6% – 85.7%), either mucinous or tubular (table 3).
Table 3 – Cancer characteristics at diagnosis
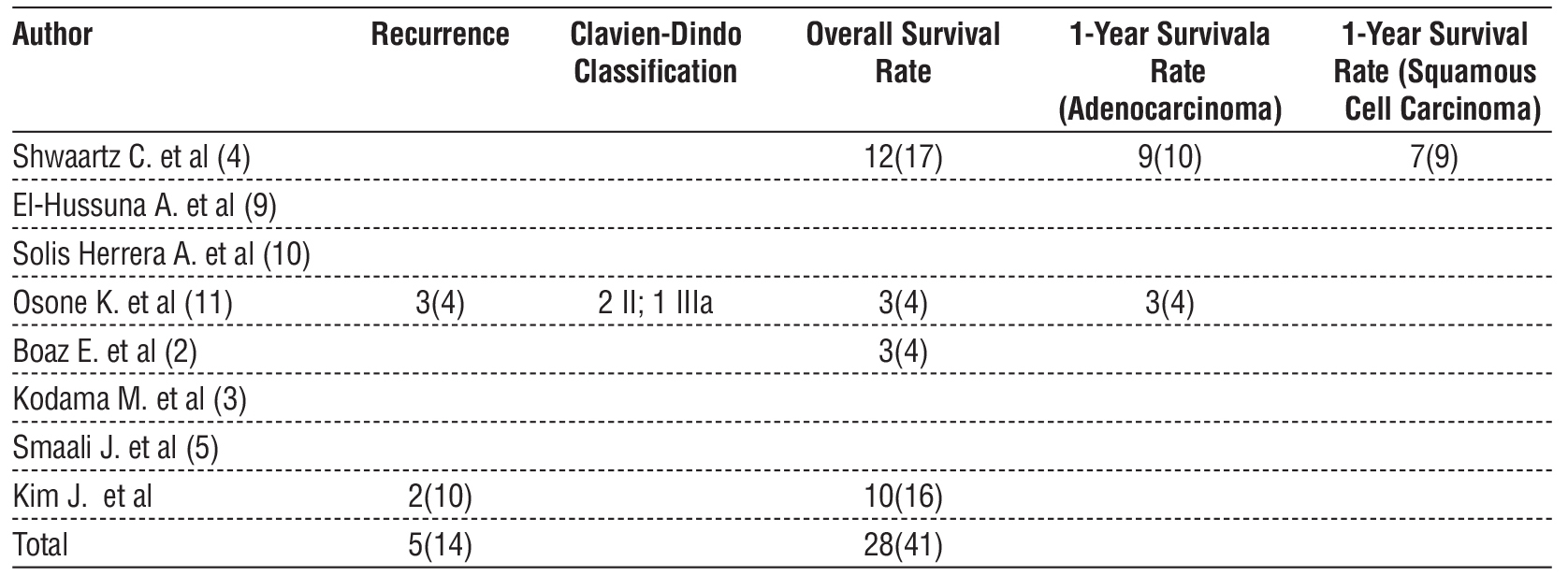
Most patients (57.8% – 100%) underwent extensive surgery, mainly abdominoperineal amputation. The recurrence rate was 35.7%.
One-year survival rates ranged from 85.7% to 90% in adenocarcinoma cases and 77.8% in squamous cell carcinoma. Overall survival was 68.3% (table 4).
Table 4 – Treatment outcomes
DISCUSSION
Anorectal cancer (ARC) associated with Crohn’s Disease (CD) is a rare entity, with an estimated incidence ranging from 0.54% to 0.8% in patients with CD, according to the studies analyzed. The findings of this systematic review highlight the complexity of diagnosing and treating this condition, emphasizing the need for a high index of clinical suspicion for early detection.
The data show that ARC occurs predominantly in males (61.2%) and is associated with early CD diagnosis, typically between 21 and 25.5 years of age. The mean interval between CD diagnosis and ARC development was 25.6 ± 9.5 years, a significant duration that underscores the importance of long-term clinical follow-up. These findings align with previous studies pointing to persistent chronic inflammation, particularly in the context of long-standing perianal fistulas, as a predisposing factor for carcinogenesis.
Most ARC cases were identified through biopsies performed on asymptomatic chronic fistulas (47.4% – 81.3%). This underscores the need for a proactive approach in the surveillance of perianal fistulas in CD patients, as these lesions may conceal carcinoma. Furthermore, 36.8% of patients presented with metas-tases at diagnosis, reflecting the tumor’s aggressiveness and reinforcing the importance of early screening.
The results also indicate that adenocarcinomas (52.6% – 85.7%) are the most frequent histological sub-types, followed by squamous cell carcinomas. These findings are consistent with the existing literature, in which adenocarcinoma is the predominant form of ARC associated with CD, particularly in patients with chronic inflammation and long-standing fistulas.
Regarding treatment, most patients (57.8% – 100%) underwent extensive surgeries, primarily abdomino-perineal amputation, reflecting the disease's severity and the challenge of achieving an adequate oncological resection. The high recurrence rate (35.7%) is concerning, highlighting the need for rigorous post-operative monitoring and consideration of adjuvant and neoadjuvant therapies.
In terms of survival, the one-year survival rate ranged from 85.7% to 90% for adenocarcinoma and 77.8% for squamous cell carcinoma, with an overall survival rate of 68.3%. These results reflect the disease’s guarded prognosis, especially in cases diagnosed late or with metastases at presentation.
This systematic review presents several limitations that must be considered when interpreting its findings. First, the number of studies and patients included is small, reflecting the rarity of this condition. Most of the available data derive from retrospective studies and case reports, which are subject to selection bias and incomplete data reporting. Additionally, the methodological heterogeneity across studies — including variations in diagnostic criteria, follow-up duration, and treatment approaches — limits the ability to perform quantitative synthesis or meta-analysis. Finally, the lack of molecular and genetic analyses in the included studies restricts the understanding of the pathophysiological mechanisms underlying ARC development in CD.
Future research should focus on multicenter prospective studies with larger sample sizes to establish standardized surveillance protocols for patients with long-standing perianal Crohn’s disease. Molecular and genomic profiling may help identify biomarkers predictive of malignant transformation, enabling earlier diagnosis. Additionally, developing consensus guidelines for biopsy timing, imaging follow-up, and treatment strategies could significantly improve patient outcomes and reduce diagnostic delay. Collaborative registries across referral centers would also enhance data collection and allow for more robust epidemiological and clinical analysis.
CONCLUSION
Anorectal cancer associated with Crohn’s disease represents a significant clinical challenge due to its low incidence, delayed diagnosis, and poor prognosis. The findings of this systematic review underscore the need for rigorous, long-term clinical follow-up, particularly in patients with chronic perianal fistulas, given their association with carcinogenesis. The high rate of metastasis at diagnosis and the complexity of treatment - often requiring radical surgery - highlight the importance of effective screening strategies.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or notforprofit sectors.
Ethical Consideration
As this study is a systematic review of previously published data, no ethical approval or informed consent was required.
REFERENCES
1. Yukiko H, Kitaro F, Daijiro H, Koji M, Takafumi M. Anorectal cancer surveillance in Crohn's disease. J Anus Rectum Colon. 2018;2(4): 145-154.
2. Boaz E, Freund MR, Harbi A, Dagan A, Gilshtein H, Reissman P, et al. Anorectal Malignancies Presenting as a Perianal Abscess or Fistula. Am Surg. 2023;89(6):2572-2576.
3. Kodama M, Kobayashi D, Iihara K, Abe K, Sahara R, Sassa M, et al, Adenocarcinoma within anorectal fistulae: different clinicopathological characteristics between Crohn’s disease-associated type and the usual type. Mod Pathol. 2019;32(2):314-325.
4. Shwaartz C, Munger JA, Deliz JR, Bornstein JE, Gorfine SR, Chessin DB, et al. Fistula-Associated Anorectal Cancer in the Setting of Crohn’s Disease. Dis Colon Rectum. 2016;59(12):1168-1173.
5. Smaali J, Sekkach Y. Adénocarcinome ano-réctal après traitement par Infliximab pour une maladie de Crohn fistulisante. Pan Afr Med J. 2017;26:172. French
6. Beaugerie L, Carrat F, Nahon S, Zeitoun JD, Sabaté JM, Peyrin-Biroulet L, et al. High Risk of Anal and Rectal Cancer in Patients With Anal and/or Perianal Crohn’s Disease. Clin Gastroenterol Hepatol. 2018;16(6):892-899.e2.
7. Wisniewski A, Fléjou JF, Siproudhis L, Abramowitz L, Svrcek M, Beaugerie L. Anal Neoplasia in Inflammatory Bowel Disease: Classification Proposal, Epidemiology, Carcinogenesis, and Risk Management Perspectives. J Crohns Colitis. 2017;11(8):1011-1018.
8. Ruel J, Ko HM, Roda G, Patil N, Zhang D, Jharap B, et al. Anal Neoplasia in Inflammatory Bowel Disease Is Associated With HPV and Perianal Disease. Clin Transl Gastroenterol. 2016;7(3):e148.
9. El-Hussuna A, Lemser CE, Iversen AT, Højgaard Allin K, Jess T. Risk of anorectal cancer in patients with Crohn's disease and perianal fistula: a nationwide Danish cohort study. Colorectal Dis. 2023; 25(7):1453-1459.
10. Solis Herrera A, del Carmen Arias M, Solís Aris RI, Solís Arias MP. The unsuspected source of oxygen in Crohn's disease. AJMCRR. 2024;3(3):1-20.
11. Osone K, Ogawa H, Katayama C, Shibasaki Y, Suga K, Komine C, et al. Outcomes of surgical treatment in patients with anorectal fistula cancer. Surg Case Rep. 2021;7(1):32.
Full Text Sources:
Abstract:
Views: 560

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.