Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
Assessment of Adherence to the Use of the World Health Organization Surgical Safety Checklist Among Medical Staff in Ain Shams University Hospital, Egypt
ABSTRACT
Introduction: Surgical services are considered one of the main and most important, fundamental health-care services provided in any health-care system. Annually, approximately 310 million operations are performed worldwide. The World Health Organization checklist is aimed at detecting potential safety hazards, improving communication among surgical staff, and decreasing the incidence of drug and surgical site errors.
We aim to assess the degree of adherence of medical staff to the safety checklist and to study the effect of supervision on adherence.
Methods: This study was conducted in the Department of Surgery, Ain shams University Hospital, between January 2017 and December 2018, and included all the patients who underwent either elective or emergency general surgical operations in the selected unit at Ain Shams University Hospital. The baseline pre-intervention phase of the study was conducted then the checklist was implemented for 4 months without supervision followed by another 4 months with supervision.
Results: We observed that the incidence of postoperative morbidities (21.40%) before implementation significantly decreased after implementation without (11.2%) and with supervision (4.7%). A significant improvement in adherence was observed in the three groups in terms of the number of patients with missed items in the checklist (10.9%) after implementation without (5.2%) and with supervision (7 patients, 1.6%).
Conclusion: Our results indicated that the implementation of the surgical safety checklist was associated with improved postoperative results and decreased postoperative morbidities linked to the surgery. Further research with a larger sample is needed to investigate the association between the checklist implementation and its effect on patient mortality and survival.
Keywords: surgical safety checklist, surgical services, effect of supervision on adherence
BACKGROUND
Surgical services are considered one of the main and most important, fundamental health-care services provided in any health-care system. Annually, approximately 280 to 310 million major surgical operations are performed worldwide, which means that >1 of every 25 living human beings will undergo a major surgical operation annually (1). Such a number is large and reflects the importance and significant outcomes of surgical operations on public health.
Surgical operations are associated with different outcomes such as increased risk of mortality and morbidity. Estimations of morbidity and mortality rates vary between different countries and types of surgical operations (2-4). Many published papers estimated that 75 million patients per year develop postoperative complications worldwide, which will eventually lead to >2 million deaths per year (5,6). Many previously published studies in the United Kingdom estimated that one of every six patients who underwent surgical operations had postoperative complications, half of which were avoidable medical mistakes. This costs the united kingdom approximately £1 billion every year (7-9). The numbers are more likely to be much higher in the developed country.
Most iatrogenic surgical adverse events and complications can be attributed to surgical site infections, drug errors such as drug allergies, anatomical site errors, surgical equipment malfunctioning, and retained surgical foreign bodies such as sponges (10). Checklists can be used worldwide to standardize the quality of medical services provided to patients. The World Health Organization (WHO) has created the “Safe surgery save lives” program, which is aimed at increasing the quality of surgical care provided worldwide. The WHO surgical safety checklist is now considered one of the most used surgical checklists in >4000 hospitals worldwide (11). The WHO checklist is aimed at detecting potential safety hazards, improving communication among surgical staff, and decrease the incidence of drug and surgical site errors (12).
Despite the numerous possible benefits of using the WHO checklist, many factors can contribute to its implementation, such as limited low-income settings, confusion about the aim and purpose of the checklist, and rejection by the surgical staff to use it (13-16).
To achieve successful implementation of the WHO Surgical safety checklist, all health-care providers included in the health system must adhere to the checklist, starting from the hospital manager; this can be achieved by creating a multidisciplinary environment, organizing training groups, and providing constructive feedback in the health-care system (17).
To our knowledge, Egypt is still lagging in the issue of surgical safety practice. Thus, in this study, we aimed to assess the adherence of medical staff to the surgical safety checklist and the effects of supervision on the implementation and patient outcomes, which is justified by the high global incidence of potentially preventable adverse events during surgery. In this study, we aimed to assess the degree of adherence of medical staff to the safety checklist and to examine the effect of supervision on adherence.
METHODS
This pre-intervention/post-intervention study conducted in a surgical unit in the Department of Surgery, Ain Shams University Hospital, between January 2017 and December 2018, and included all patients who underwent either elective or emergency general surgical operations in the selected unit at Ain Shams University Hospital. The final number of patients included was 408 patients.
The baseline pre-intervention phase of the study was conducted between January 2017 and May 2017 to assess the secondary postoperative outcomes before implementing the surgical safety checklist. In the first week of May 2017, all surgical operation teams had a 1-week training program on the safety checklist. Thereafter, the checklist was implemented for 4 months without supervision, followed by another 4 months with supervision. A circulating nurse was designated as the checklist coordinator after undergoing adequate training. Later, she was responsible for filling out the checklist, which was then integrated with the patient’s medical files. The coordinator nurse was in charge of checking the sign-in, timeout, and sign-out phases by interviewing the anesthetists and surgeon or/and operating nurses. Adherence was assessed every month by reviewing the checklist completeness.
Patient outcomes were measured and compared with those in the pre-implementation phase.
Statistical analysis
The statistical analyses were performed using SPSS 23.0.A univariate analysis was performed to generate descriptive statistics for the defendant variables (adherence and patient outcomes) as continuous variables presented as mean ± SD. Descriptive statistics was used for the demographic variables such as age, weight, and body mass index. A bivariate analysis was conducted to examine the association between the checklist completeness and type, surgery duration and time, surgeon experience, and checklist fatigue using the chi-square test. To assess the relationship between adherence and patient outcome, patient outcomes before and after implementation, and adherence before and after supervision were evaluated.
The confidence interval was set at 95%, and the acceptable margin of error was set at 5%. Thus, the following p values were considered: >0.05, nonsignificant (NS); <0.05, significant (S); and <0.01, highly significant.
RESULTS
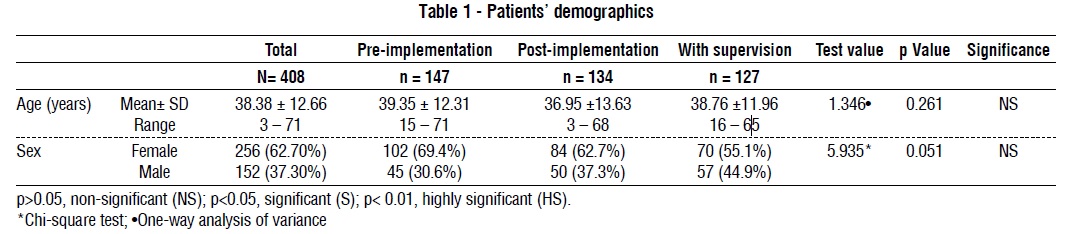
A total of 408 patients were included in the study. The mean age of the patients was 38.38 ± 12.66. Of the patients, 62.70% were women, and the rest were men. The patients’ characteristics are described in table 1.
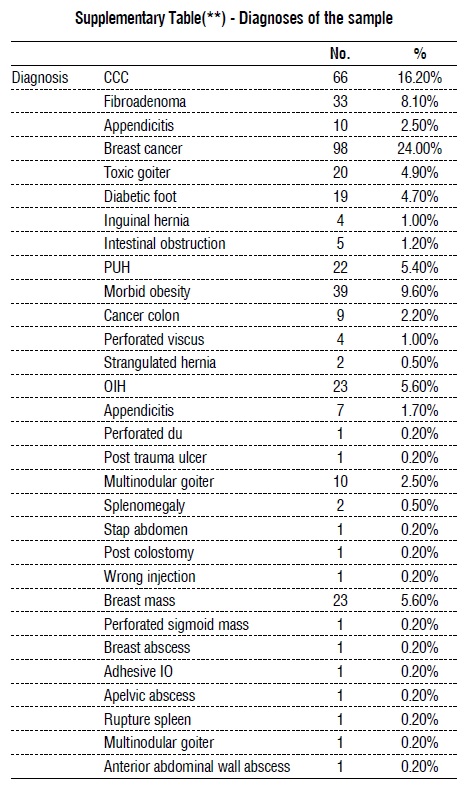
The different diagnoses and types of operation for the whole sample are shown in the supplementary table (*) and supplementary table (**).
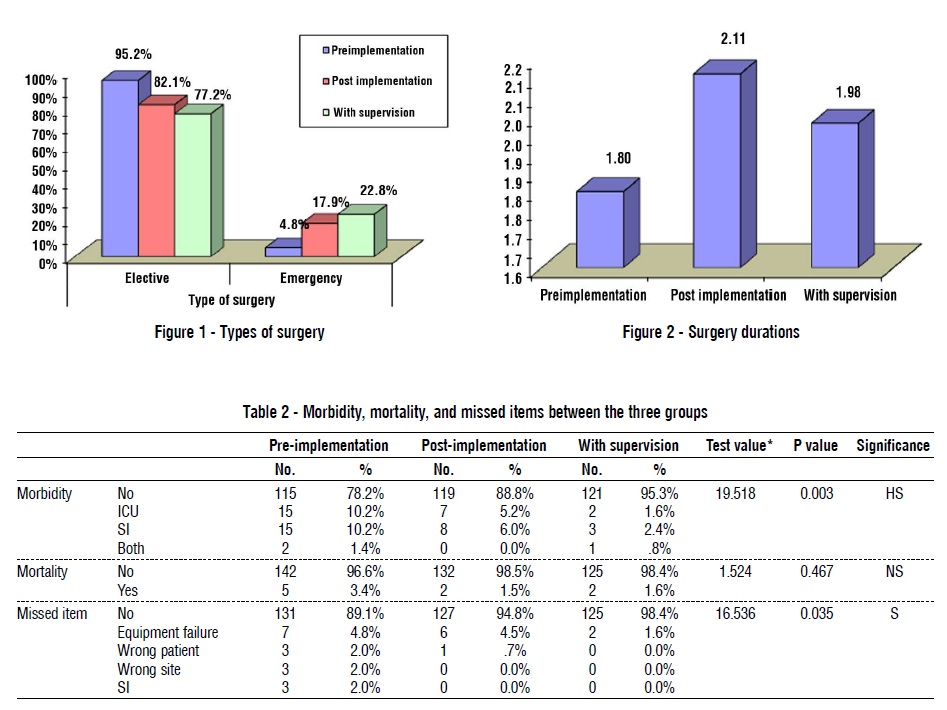
Of the patients, 348 (85.30%) underwent elective surgery, while the other 60 (14.70%) underwent emergency surgery, with a median surgery duration of 1.96 ± 0.84 hours. Of the total surgeries, 407 were performed under general anesthesia, and only 1 operation was performed under spinal anesthesia (figs. 1, 2). The total number of mortalities was 6 (2.20%), with only 25 cases (6.10%) of reported missed items in the checklist (table 2).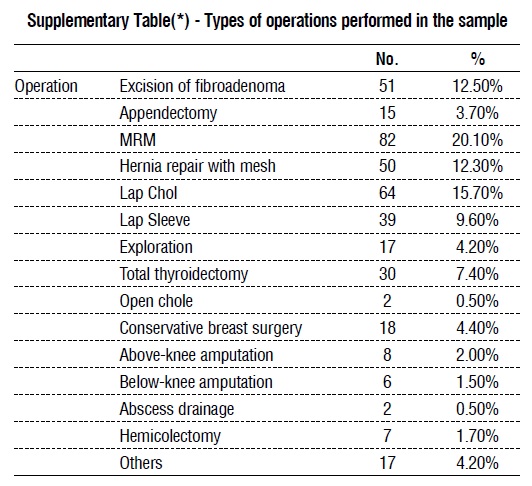
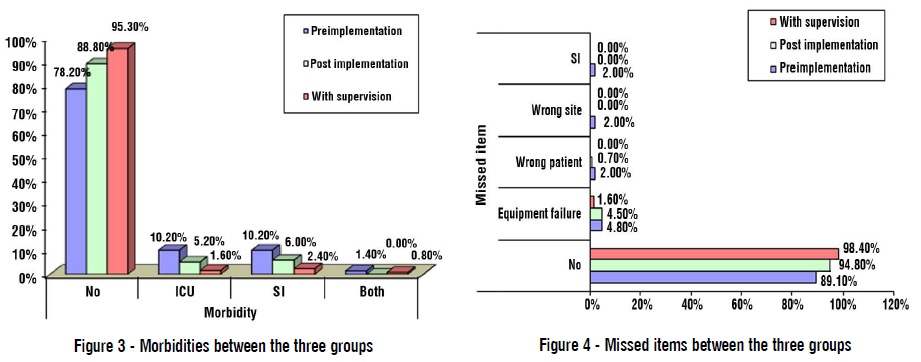
When comparing the postoperative complications among the three phases of the study, we found a significant decrease in the incidence of postoperative morbidities, in which postoperative morbidities occurred in 32 patients (21.40%) before implementation and in 15 patients (11.2%) after implementation without supervision and in 4 patients (4.7%) before implementation with supervision (p=0.003; fig. 3).
A significant improvement in adherence was also observed in the three groups in terms of having the number of patients with missed items in the checklist, with 16 patients (10.9%) before implementation and 7 patients (5.2%) after implementation without supervision and 2 patients (1.6%) after implementation with supervision (p=0.035; fig. 4). No significant difference in mortality rate was found among the three groups (table 2).

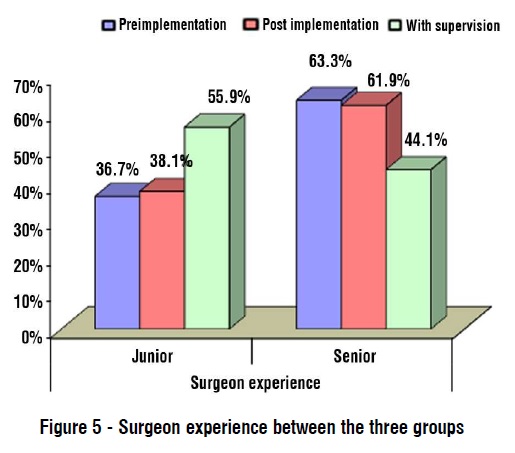
Regarding surgeon experience, a significant increase in the experience of junior surgeons was observed after the implementation of the checklist, with an increase in the number of junior surgeons conducting surgical operations under the supervision of less senior surgeons (p = 0.002; table 3 and fig. 5).
DISCUSSION
In this study, we found statistically significant decreases in the incidence rates of postoperative morbidities and missed items in the checklist with the progression of the study into the second and third phases. The WHO safety checklist implementation with supervision was associated with the lowest incidence rates of morbidities and missed items, followed by that without supervision.
The superior survival results associated with the implementation of the surgical safety checklist are attributable to the direct influence on surgery and the surgeon, such as marking the right surgical site. Another aspect of the surgical checklist is increasing the communication and teamwork between surgical staff to create a better environment during the operation.
Such findings may lead to the assumption that the implementation of the WHO safety checklist is associated with better health-care services, which leads to decreased postoperative mortalities and morbidities.
Many previously published studies have associated the implementation of the surgical safety checklist with improved mortality and morbidity outcomes. In 2014, a European multicentric study reported that the implementation of a safety checklist was associated with 19% lower risk of postoperative hospital mortality (18). Another study conducted in South America reported a 27% decrease in postoperative mortality after implementing the surgical safety checklist (19).
Middle- or low-income countries have less reported evidence of the advantages of implementing a surgical safety checkbox in the routine workup in surgery departments (20).
In contrast to our findings, those of one of the largest multicentric studies to evaluate the effect of implementing a surgical safety checklist in Canada reported no beneficial gains associated with the implementation of the checklist after comparing the data of >200,000 patients (21). Such results may be attributed to the excellent, high-quality health-care system in Canada, where everyone is covered by health insurance, which may cause fewer comorbidities that lead to less postoperative complications and mortality.
In a previously published meta-analysis conducted in multiple low- and middle-income countries, the implementation of the safety checklist was associated with lower postoperative mortality, even with the significantly lower use frequency of the safety checklist in the lower-income countries (22). This indicates the positive effect of implementing a checklist on surgical outcomes and highlights the importance of spreading the use of the checklist in less developed countries. In such countries, the importance of the checklist may not be brought to the attention of health-care providers; thus, more governmental and academic efforts must be made to generalize the use of a safe surgical checklist in the routine workup of patients undergoing surgery.
In our study, >85% of the surgical operations performed were elective surgeries. This may indicate that the implementation of a checklist may be neglected in the workup for emergency surgeries, with less time allocated for the preparation of patients, and the importance of the time asset in such settings. The Global Surg study focused more on emergency laparotomy operations and reported that the checklist can be used in the setting of emergency surgery, and the implementation of the checklist was associated with superior results regarding the morbidity and mortality of patients (22).
Many studies have linked the incidence of postoperative complications to the incidence of postoperative mortality and an increased period of hospitalization (23,24). The use of the safety checklist is aimed at reducing the incidence of possibly preventable surgical errors, thus reducing the incidence of postoperative complications associated with increased hospitality time and mortality. By contrast, a previous study reported the implementation of the checklist to be associated with increased postoperative complications; this can be explained by the fact that in a safer, wellcontrolled, and supervised environment, the chance of early detection of any postoperative complication is increased and will lead to less mortality and shorter hospitalization time, and reduced incidence of readmission after discharge.
In our study, we reported no significant association between postoperative mortality and the implementation of the surgical safety checklist. In contrast to our findings, most findings of the previous papers associated the implementation of the checklist with reduced postoperative mortality. One explanation of our result can be our relatively small sample size and different operations performed with different risks of complications and mortality. As the increased number of easy, low-risk operations may lower the incidence of pre-implementation mortality, the difference between the pre- and post-implementation mortality rates may decrease.
In our study, the implementation of the checklist was associated with more involvement of junior surgeons and decreased involvement of senior surgeons, who were only supervising and ensuring that the junior surgeons adhered to the checklist. The incidence of missed items was lowest in the third phase of our study, when the junior surgeons were under the supervision of the senior surgeons. Some of the weak points of this study are the relatively small number of patients included in the final analysis, the fact that the study was conducted in only one surgical unit in Ain Shams University Hospital. Thus, it would be difficult to generalize the outcomes of this study.
CONCLUSION
In this study, our results indicated that the implementation of the surgical safety checklist was associated with better postoperative results and decreased postoperative morbidity linked to the surgery. Further research is needed with a larger sample to investigate the association between checklist implementation and its effect on patient mortality and survival.
Conflicts of interest and Source of Funding>
This work was funded by the National Institute of Health, Fogarty International Center, USA, through grant No. 2D43TW007296.
Authors declare no conflict of interest.
Ethics approval
• The Institutional Review Board (IRB) of Ain Shams University, Cairo, Egypt.
Date: 5-3-2017 Reference: IRB 00006379
• The Institutional Review Board (IRB) of University of Maryland, Baltimore, USA Date: Reference: HP-00062968
REFERENCES>
1. Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe- Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015; 385 Suppl 2:S11.
2. Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012; 380(9847):1059-65.
3. Kable AK, Gibberd RW, Spigelman AD. Adverse events in surgical patients in Australia. Int J Qual Health Care. 2002;14(4):269-76.
4. Mullen R, Scollay JM, Hecht G, McPhillips G, Thompson AM. Death within 48 h--adverse events after general surgical procedures. Surgeon. 2012;10(1):1-5.
5. International Surgical Outcomes Study group. Global patient outcomes after elective surgery: prospective cohort study in 27 low-, middle- and high-income countries [published correction appears in Br J Anaesth. 2017 Sep 1;119(3):553]. Br J Anaesth. 2016;1.
6. Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, William R Berry 3, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008; 372(9633):139-144.
7. Abbott TE, Ahmad T, Phull MK, Fowler AJ, Hewson R, Biccard BM, et al. The surgical safety checklist and patient outcomes after surgery: a prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018;120(1):146-155.
8. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126(1):66-75.
9. Panesar SS, Cleary K, Sheikh A, Donaldson L. The WHO checklist: a global tool to prevent errors in surgery. Patient Saf Surg. 2009;3(1):9.
10. NCEPOD. Knowing the Risk: A review of Knowing the Risk: A review of the peri-operative care of surgical patients. UK: National Confidential Enquiry into Patient Outcome and Death, 201111] Hornpout LH, de Bruijne MC, Wagner C, et al. Direct medical costs o.
11. Putnam LR, Levy SM, Sajid M, Dubuisson DA, Rogers NB, Kao LS, et al. Multifaceted interventions improve adherence to the surgical checklist. Surgery. 2014;156(2):336-344.
12. WHO surgical safety checklist. 2008 (Available from:) http://www. who.int/patientsafety/safesurgery/checklist/en/ Date accessed: May 9, 2017.
13. Close KL, Baxter LS, Ravelojaona VA, Rakotoarison HN, Bruno E, Herbert A, et al. Overcoming challenges in implementing the WHO Surgical Safety Checklist: lessons learnt from using a checklist training course to facilitate rapid scale up in Madagascar. BMJ Glob Health. 2017;2(Suppl 4):e000430.
14. Aveling EL, McCulloch P, Dixon-Woods M. A qualitative study comparing experiences of the surgical safety checklist in hospitals in high-income and low-income countries. BMJ Open. 2013;3(8): e003039.
15. Kasatpibal N, Senaratana W, Chitreecheur J, Chotirosniramit N, Pakvipas P, Junthasopeepun P. Implementation of the World Health Organization surgical safety checklist at a University Hospital in Thailand. Surg Infect (Larchmt). 2012;13(1):50-6.
16. Lilaonitkul M, Kwikiriza A, Ttendo S, Kiwanuka J, Munyarungero E, Walker IA, et al. Implementation of the WHO Surgical Safety Checklist and surgical swab and instrument counts at a regional referral hospital in Uganda – a quality improvement project. Anaesthesia. 2015;70(12):1345-55.
17. Hales BM, Pronovost PJ. The checklist is a tool for error management and performance improvement. J Crit Care. 2006;21(3):231-5.
18. Jammer I, Ahmad T, Aldecoa C, Koulenti D, Goranovi? T, Grigoras I, et al. Point prevalence of surgical checklist use in Europe: relationship with hospital mortality. Br J Anaesth. 2015;114(5):801-7.
19. Lacassie HJ, Ferdinand C, Guzman S, Camus L, Echevarria GC. World Health Organization (WHO) surgical safety checklist implementation and its impact on perioperative morbidity and mortality in an academic medical center in Chile. Medicine (Baltimore). 2016; 95(23):e3844.
20. Chaudhary N, Varma V, Kapoor S, Mehta N, Kumaran V, Nundy S. Implementation of a surgical safety checklist and postoperative outcomes: a prospective randomized controlled study. J Gastrointest Surg. 2015;19(5):935-42.
21. Urbach DR, Govindarajan A, Saskin R, Wilton AS, Baxter NN. Introduction of surgical safety checklists in Ontario, Canada. N Engl J Med. 2014;370(11):1029-38.
22. GlobalSurg Collaborative. Pooled analysis of WHO Surgical Safety Checklist use and mortality after emergency laparotomy. Br J Surg. 2019;106(2):e103-e112.
23. Borgi J, Rubinfeld I, Ritz J, Jordan J, Velanovich V. The differential effects of intermediate complications with postoperative mortality. Am Surg. 2013;79(3):261-6.
24. Khan NA, Quan H, Bugar JM, Lemaire JB, Brant R, Ghali WA. Association of postoperative complications with hospital costs and length of stay in a tertiary care center. J Gen Intern Med. 2006; 21(2):177-180.
Full Text Sources:
Abstract:
Views: 1903

Introduction: Surgical services are considered one of the main and most important, fundamental health-care services provided in any health-care system. Annually, approximately 310 million operations are performed worldwide. The World Health Organization checklist is aimed at detecting potential safety hazards, improving communication among surgical staff, and decreasing the incidence of drug and surgical site errors.
We aim to assess the degree of adherence of medical staff to the safety checklist and to study the effect of supervision on adherence.
Methods: This study was conducted in the Department of Surgery, Ain shams University Hospital, between January 2017 and December 2018, and included all the patients who underwent either elective or emergency general surgical operations in the selected unit at Ain Shams University Hospital. The baseline pre-intervention phase of the study was conducted then the checklist was implemented for 4 months without supervision followed by another 4 months with supervision.
Results: We observed that the incidence of postoperative morbidities (21.40%) before implementation significantly decreased after implementation without (11.2%) and with supervision (4.7%). A significant improvement in adherence was observed in the three groups in terms of the number of patients with missed items in the checklist (10.9%) after implementation without (5.2%) and with supervision (7 patients, 1.6%).
Conclusion: Our results indicated that the implementation of the surgical safety checklist was associated with improved postoperative results and decreased postoperative morbidities linked to the surgery. Further research with a larger sample is needed to investigate the association between the checklist implementation and its effect on patient mortality and survival.
Keywords: surgical safety checklist, surgical services, effect of supervision on adherence
BACKGROUND
Surgical services are considered one of the main and most important, fundamental health-care services provided in any health-care system. Annually, approximately 280 to 310 million major surgical operations are performed worldwide, which means that >1 of every 25 living human beings will undergo a major surgical operation annually (1). Such a number is large and reflects the importance and significant outcomes of surgical operations on public health.
Surgical operations are associated with different outcomes such as increased risk of mortality and morbidity. Estimations of morbidity and mortality rates vary between different countries and types of surgical operations (2-4). Many published papers estimated that 75 million patients per year develop postoperative complications worldwide, which will eventually lead to >2 million deaths per year (5,6). Many previously published studies in the United Kingdom estimated that one of every six patients who underwent surgical operations had postoperative complications, half of which were avoidable medical mistakes. This costs the united kingdom approximately £1 billion every year (7-9). The numbers are more likely to be much higher in the developed country.
Most iatrogenic surgical adverse events and complications can be attributed to surgical site infections, drug errors such as drug allergies, anatomical site errors, surgical equipment malfunctioning, and retained surgical foreign bodies such as sponges (10). Checklists can be used worldwide to standardize the quality of medical services provided to patients. The World Health Organization (WHO) has created the “Safe surgery save lives” program, which is aimed at increasing the quality of surgical care provided worldwide. The WHO surgical safety checklist is now considered one of the most used surgical checklists in >4000 hospitals worldwide (11). The WHO checklist is aimed at detecting potential safety hazards, improving communication among surgical staff, and decrease the incidence of drug and surgical site errors (12).
Despite the numerous possible benefits of using the WHO checklist, many factors can contribute to its implementation, such as limited low-income settings, confusion about the aim and purpose of the checklist, and rejection by the surgical staff to use it (13-16).
To achieve successful implementation of the WHO Surgical safety checklist, all health-care providers included in the health system must adhere to the checklist, starting from the hospital manager; this can be achieved by creating a multidisciplinary environment, organizing training groups, and providing constructive feedback in the health-care system (17).
To our knowledge, Egypt is still lagging in the issue of surgical safety practice. Thus, in this study, we aimed to assess the adherence of medical staff to the surgical safety checklist and the effects of supervision on the implementation and patient outcomes, which is justified by the high global incidence of potentially preventable adverse events during surgery. In this study, we aimed to assess the degree of adherence of medical staff to the safety checklist and to examine the effect of supervision on adherence.
METHODS
This pre-intervention/post-intervention study conducted in a surgical unit in the Department of Surgery, Ain Shams University Hospital, between January 2017 and December 2018, and included all patients who underwent either elective or emergency general surgical operations in the selected unit at Ain Shams University Hospital. The final number of patients included was 408 patients.
The baseline pre-intervention phase of the study was conducted between January 2017 and May 2017 to assess the secondary postoperative outcomes before implementing the surgical safety checklist. In the first week of May 2017, all surgical operation teams had a 1-week training program on the safety checklist. Thereafter, the checklist was implemented for 4 months without supervision, followed by another 4 months with supervision. A circulating nurse was designated as the checklist coordinator after undergoing adequate training. Later, she was responsible for filling out the checklist, which was then integrated with the patient’s medical files. The coordinator nurse was in charge of checking the sign-in, timeout, and sign-out phases by interviewing the anesthetists and surgeon or/and operating nurses. Adherence was assessed every month by reviewing the checklist completeness.
Patient outcomes were measured and compared with those in the pre-implementation phase.
Statistical analysis
The statistical analyses were performed using SPSS 23.0.A univariate analysis was performed to generate descriptive statistics for the defendant variables (adherence and patient outcomes) as continuous variables presented as mean ± SD. Descriptive statistics was used for the demographic variables such as age, weight, and body mass index. A bivariate analysis was conducted to examine the association between the checklist completeness and type, surgery duration and time, surgeon experience, and checklist fatigue using the chi-square test. To assess the relationship between adherence and patient outcome, patient outcomes before and after implementation, and adherence before and after supervision were evaluated.
The confidence interval was set at 95%, and the acceptable margin of error was set at 5%. Thus, the following p values were considered: >0.05, nonsignificant (NS); <0.05, significant (S); and <0.01, highly significant.
RESULTS
A total of 408 patients were included in the study. The mean age of the patients was 38.38 ± 12.66. Of the patients, 62.70% were women, and the rest were men. The patients’ characteristics are described in table 1.
The different diagnoses and types of operation for the whole sample are shown in the supplementary table (*) and supplementary table (**).
Of the patients, 348 (85.30%) underwent elective surgery, while the other 60 (14.70%) underwent emergency surgery, with a median surgery duration of 1.96 ± 0.84 hours. Of the total surgeries, 407 were performed under general anesthesia, and only 1 operation was performed under spinal anesthesia (figs. 1, 2). The total number of mortalities was 6 (2.20%), with only 25 cases (6.10%) of reported missed items in the checklist (table 2).
When comparing the postoperative complications among the three phases of the study, we found a significant decrease in the incidence of postoperative morbidities, in which postoperative morbidities occurred in 32 patients (21.40%) before implementation and in 15 patients (11.2%) after implementation without supervision and in 4 patients (4.7%) before implementation with supervision (p=0.003; fig. 3).
A significant improvement in adherence was also observed in the three groups in terms of having the number of patients with missed items in the checklist, with 16 patients (10.9%) before implementation and 7 patients (5.2%) after implementation without supervision and 2 patients (1.6%) after implementation with supervision (p=0.035; fig. 4). No significant difference in mortality rate was found among the three groups (table 2).
Regarding surgeon experience, a significant increase in the experience of junior surgeons was observed after the implementation of the checklist, with an increase in the number of junior surgeons conducting surgical operations under the supervision of less senior surgeons (p = 0.002; table 3 and fig. 5).
DISCUSSION
In this study, we found statistically significant decreases in the incidence rates of postoperative morbidities and missed items in the checklist with the progression of the study into the second and third phases. The WHO safety checklist implementation with supervision was associated with the lowest incidence rates of morbidities and missed items, followed by that without supervision.
The superior survival results associated with the implementation of the surgical safety checklist are attributable to the direct influence on surgery and the surgeon, such as marking the right surgical site. Another aspect of the surgical checklist is increasing the communication and teamwork between surgical staff to create a better environment during the operation.
Such findings may lead to the assumption that the implementation of the WHO safety checklist is associated with better health-care services, which leads to decreased postoperative mortalities and morbidities.
Many previously published studies have associated the implementation of the surgical safety checklist with improved mortality and morbidity outcomes. In 2014, a European multicentric study reported that the implementation of a safety checklist was associated with 19% lower risk of postoperative hospital mortality (18). Another study conducted in South America reported a 27% decrease in postoperative mortality after implementing the surgical safety checklist (19).
Middle- or low-income countries have less reported evidence of the advantages of implementing a surgical safety checkbox in the routine workup in surgery departments (20).
In contrast to our findings, those of one of the largest multicentric studies to evaluate the effect of implementing a surgical safety checklist in Canada reported no beneficial gains associated with the implementation of the checklist after comparing the data of >200,000 patients (21). Such results may be attributed to the excellent, high-quality health-care system in Canada, where everyone is covered by health insurance, which may cause fewer comorbidities that lead to less postoperative complications and mortality.
In a previously published meta-analysis conducted in multiple low- and middle-income countries, the implementation of the safety checklist was associated with lower postoperative mortality, even with the significantly lower use frequency of the safety checklist in the lower-income countries (22). This indicates the positive effect of implementing a checklist on surgical outcomes and highlights the importance of spreading the use of the checklist in less developed countries. In such countries, the importance of the checklist may not be brought to the attention of health-care providers; thus, more governmental and academic efforts must be made to generalize the use of a safe surgical checklist in the routine workup of patients undergoing surgery.
In our study, >85% of the surgical operations performed were elective surgeries. This may indicate that the implementation of a checklist may be neglected in the workup for emergency surgeries, with less time allocated for the preparation of patients, and the importance of the time asset in such settings. The Global Surg study focused more on emergency laparotomy operations and reported that the checklist can be used in the setting of emergency surgery, and the implementation of the checklist was associated with superior results regarding the morbidity and mortality of patients (22).
Many studies have linked the incidence of postoperative complications to the incidence of postoperative mortality and an increased period of hospitalization (23,24). The use of the safety checklist is aimed at reducing the incidence of possibly preventable surgical errors, thus reducing the incidence of postoperative complications associated with increased hospitality time and mortality. By contrast, a previous study reported the implementation of the checklist to be associated with increased postoperative complications; this can be explained by the fact that in a safer, wellcontrolled, and supervised environment, the chance of early detection of any postoperative complication is increased and will lead to less mortality and shorter hospitalization time, and reduced incidence of readmission after discharge.
In our study, we reported no significant association between postoperative mortality and the implementation of the surgical safety checklist. In contrast to our findings, most findings of the previous papers associated the implementation of the checklist with reduced postoperative mortality. One explanation of our result can be our relatively small sample size and different operations performed with different risks of complications and mortality. As the increased number of easy, low-risk operations may lower the incidence of pre-implementation mortality, the difference between the pre- and post-implementation mortality rates may decrease.
In our study, the implementation of the checklist was associated with more involvement of junior surgeons and decreased involvement of senior surgeons, who were only supervising and ensuring that the junior surgeons adhered to the checklist. The incidence of missed items was lowest in the third phase of our study, when the junior surgeons were under the supervision of the senior surgeons. Some of the weak points of this study are the relatively small number of patients included in the final analysis, the fact that the study was conducted in only one surgical unit in Ain Shams University Hospital. Thus, it would be difficult to generalize the outcomes of this study.
CONCLUSION
In this study, our results indicated that the implementation of the surgical safety checklist was associated with better postoperative results and decreased postoperative morbidity linked to the surgery. Further research is needed with a larger sample to investigate the association between checklist implementation and its effect on patient mortality and survival.
Conflicts of interest and Source of Funding>
This work was funded by the National Institute of Health, Fogarty International Center, USA, through grant No. 2D43TW007296.
Authors declare no conflict of interest.
Ethics approval
• The Institutional Review Board (IRB) of Ain Shams University, Cairo, Egypt.
Date: 5-3-2017 Reference: IRB 00006379
• The Institutional Review Board (IRB) of University of Maryland, Baltimore, USA Date: Reference: HP-00062968
REFERENCES>
1. Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe- Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015; 385 Suppl 2:S11.
2. Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012; 380(9847):1059-65.
3. Kable AK, Gibberd RW, Spigelman AD. Adverse events in surgical patients in Australia. Int J Qual Health Care. 2002;14(4):269-76.
4. Mullen R, Scollay JM, Hecht G, McPhillips G, Thompson AM. Death within 48 h--adverse events after general surgical procedures. Surgeon. 2012;10(1):1-5.
5. International Surgical Outcomes Study group. Global patient outcomes after elective surgery: prospective cohort study in 27 low-, middle- and high-income countries [published correction appears in Br J Anaesth. 2017 Sep 1;119(3):553]. Br J Anaesth. 2016;1.
6. Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, William R Berry 3, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008; 372(9633):139-144.
7. Abbott TE, Ahmad T, Phull MK, Fowler AJ, Hewson R, Biccard BM, et al. The surgical safety checklist and patient outcomes after surgery: a prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018;120(1):146-155.
8. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126(1):66-75.
9. Panesar SS, Cleary K, Sheikh A, Donaldson L. The WHO checklist: a global tool to prevent errors in surgery. Patient Saf Surg. 2009;3(1):9.
10. NCEPOD. Knowing the Risk: A review of Knowing the Risk: A review of the peri-operative care of surgical patients. UK: National Confidential Enquiry into Patient Outcome and Death, 201111] Hornpout LH, de Bruijne MC, Wagner C, et al. Direct medical costs o.
11. Putnam LR, Levy SM, Sajid M, Dubuisson DA, Rogers NB, Kao LS, et al. Multifaceted interventions improve adherence to the surgical checklist. Surgery. 2014;156(2):336-344.
12. WHO surgical safety checklist. 2008 (Available from:) http://www. who.int/patientsafety/safesurgery/checklist/en/ Date accessed: May 9, 2017.
13. Close KL, Baxter LS, Ravelojaona VA, Rakotoarison HN, Bruno E, Herbert A, et al. Overcoming challenges in implementing the WHO Surgical Safety Checklist: lessons learnt from using a checklist training course to facilitate rapid scale up in Madagascar. BMJ Glob Health. 2017;2(Suppl 4):e000430.
14. Aveling EL, McCulloch P, Dixon-Woods M. A qualitative study comparing experiences of the surgical safety checklist in hospitals in high-income and low-income countries. BMJ Open. 2013;3(8): e003039.
15. Kasatpibal N, Senaratana W, Chitreecheur J, Chotirosniramit N, Pakvipas P, Junthasopeepun P. Implementation of the World Health Organization surgical safety checklist at a University Hospital in Thailand. Surg Infect (Larchmt). 2012;13(1):50-6.
16. Lilaonitkul M, Kwikiriza A, Ttendo S, Kiwanuka J, Munyarungero E, Walker IA, et al. Implementation of the WHO Surgical Safety Checklist and surgical swab and instrument counts at a regional referral hospital in Uganda – a quality improvement project. Anaesthesia. 2015;70(12):1345-55.
17. Hales BM, Pronovost PJ. The checklist is a tool for error management and performance improvement. J Crit Care. 2006;21(3):231-5.
18. Jammer I, Ahmad T, Aldecoa C, Koulenti D, Goranovi? T, Grigoras I, et al. Point prevalence of surgical checklist use in Europe: relationship with hospital mortality. Br J Anaesth. 2015;114(5):801-7.
19. Lacassie HJ, Ferdinand C, Guzman S, Camus L, Echevarria GC. World Health Organization (WHO) surgical safety checklist implementation and its impact on perioperative morbidity and mortality in an academic medical center in Chile. Medicine (Baltimore). 2016; 95(23):e3844.
20. Chaudhary N, Varma V, Kapoor S, Mehta N, Kumaran V, Nundy S. Implementation of a surgical safety checklist and postoperative outcomes: a prospective randomized controlled study. J Gastrointest Surg. 2015;19(5):935-42.
21. Urbach DR, Govindarajan A, Saskin R, Wilton AS, Baxter NN. Introduction of surgical safety checklists in Ontario, Canada. N Engl J Med. 2014;370(11):1029-38.
22. GlobalSurg Collaborative. Pooled analysis of WHO Surgical Safety Checklist use and mortality after emergency laparotomy. Br J Surg. 2019;106(2):e103-e112.
23. Borgi J, Rubinfeld I, Ritz J, Jordan J, Velanovich V. The differential effects of intermediate complications with postoperative mortality. Am Surg. 2013;79(3):261-6.
24. Khan NA, Quan H, Bugar JM, Lemaire JB, Brant R, Ghali WA. Association of postoperative complications with hospital costs and length of stay in a tertiary care center. J Gen Intern Med. 2006; 21(2):177-180.
Full Text Sources:
Abstract:
Views: 1903
Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Dec 2025
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.