Surgery, Gastroenterology and Oncology

|
|
Introduction: MRI is one of the main tools for staging and assessing response to neoadjuvant therapy in locally advanced rectal cancer. However, there is no consensus on its role in restaging. The aim of this retrospective study was to assess the imaging response with MRI and to compare restaging MRI with histopathological findings in patients with locally advanced rectal cancer who underwent neoadjuvant therapy.
Material and Method: A significant difference was found between staging and restaging MRI in clinical stage T (Z=-5.03, p<0.001) and N (Z=-5.15, p<0.001), tumour length (t(56)=10.35, p<0.001), mesorectal fascia status (p=0.004), and number of suspicious mesorectal lymph nodes (Z=-5.24, p<0.001).
Results: The agreement between restaging MRI and pathology was moderate for stage T and the status of the circumferential resection margin (K=0.58 and K=0.46, respectively, p=0.001), and low for stage N (K=0.34, p=0.005). Over-staging with MRI occurred in 34.4% of cases for stage T and 22.2% for stage N.
Conclusion: Restaging MRI is essential for evaluating the response to neo-adjuvant therapy in locally advanced rectal carcinoma. However, it should not be the sole basis for therapeutic decisions as its concordance with anatomopathological study is limited.
Introduction
Colorectal carcinoma is the third most common type of cancer worldwide, with rectal cancer accounting for approximately one-third of these cases (1-3). Although the incidence and mortality of colorectal cancer have been decreasing, there has been an increase in the incidence of rectal cancer, even among patients under the age of 50 (3).
RT and/or CT are often used to treat LARC, followed by total excision of the mesorectum (4-7). This treatment approach has been shown to reduce tumour size and stage, and can result in a pathological complete response in 10% to 25% of patients (6,8,9). Patients who have achieved a complete response after NAT can benefit from less invasive treatment options, such as local resection with anal sphincter sparing and the non-surgical approach after NAT known as Watch and Wait (6,8,10-12). Therefore, accurate restaging of LARC is crucial in clinical practice as subsequent therapeutic decisions may vary depending on the type of tumour response.
MRI is a crucial tool for staging and assessing clinical response to NAT (11,13-15). It has high contrast resolution, which enables the identification of various tumour characteristics, including tumour volume, degree of tumour regression, depth of invasion, lymph node staging, circumferential resection margin status, and extramural vascular invasion (16,17). However, restaging with MRI presents several challenges, including differentiating fibrosis from residual tumour, identifying residual early stage T1 and T2 lesions, and evaluating small lymph nodes (18).
The aim of this study was to assess the MRI response to NAT and to compare restaging MRI with histopathological findings in patients with LARC who underwent preoperative RT.
Material and Method
The Braga Hospital Ethics Committee approved this retrospective review without the need for informed consent. All patient data was pseudonymised before analysis.
We identified 65 consecutive patients diagnosed with rectal adenocarcinoma who received neoadjuvant RT at our institution between January 2016 and December 2020.
Inclusion criteria included: a) age 18 or older; b) histologically proven adenocarcinoma of the rectum; c) locally advanced clinical stage (cT3-4 or cN+); d) staging and restaging MRI; d) surgical resection after NAT. This study excluded patients with a history of pelvic RT, stage IV rectal cancer, synchronous colorectal carcinoma or other non-colorectal carcinoma, missing histopathological or MRI reports, recurrence of rectal cancer, and palliative surgical resections, emergency surgeries, or local resections.
Neoadjuvant therapy
The majority of patients (n=58, 89.2%) received treatment with long course chemoradiotherapy. This involved administering a total dose of 50-50.4Gy, in fractions of 1.8-2Gy, over 5 days a week, using three-dimensional conformal pelvic RT technique. Concomitant CT consisted of 5-FU in continuous infusion (350 mg/m2, administered on days 1-5 and days 29-33) or oral capecitabine (825-850 mg/m2, twice a day, during the days of RT treatment). No patients received CT between the completion of RT ± CT and surgery.
Magnetic Resonance Imaging: protocol and interpretation
All MRI scans were conducted by the Radiology Department of our institution. Rectal MRI scans were typically performed using 1.5T machine (Magnetom Avanto® model by Siemens®), with occasional use of 3T (Magnetom Verio® model by Siemens®) or 1.5T machines (Achieva Pulsar/SE model by Phillips®), equipped with volumetric phase-array antenna, following the established protocol for rectal cancer. This protocol includes high-resolution T2 FSE sequences in three planes, following axes that are orthogonal to the lesion, and an axial diffusion-weighted sequence perpendicular to the long axis of the tumour, with b-values of 0, 50, 500 and 1000. No images are obtained after the administration of intravenous paramagnetic contrast. All MRI scans were interpreted by two radiologists with more than 10 years of experience in pelvic MRI. For this study, the staging and restaging MRI reports were reviewed. These consist of structured reports containing information about the local status of the tumour, invasion of the MRF and peritoneal reflection, lymph nodes, tumour deposits and extramural venous invasion, as recommended by the European Society of Gastrointestinal and Abdominal Radiology (ESGAR) (19).
Histopathological assessment
The histopathological reports were reviewed to obtain information on the pathological tumour stage and circumferential resection margin.
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics v27. Wilcoxon’s test, McNemar’s test and the t-test for paired samples were used to compare the characteristics of the staging MRI with those of the restaging MRI. A p-value of less than 0.05 was considered statistically significant. The correlation between the restaging MRI and the histopathological findings was assessed using the Kappa coefficient of agreement. Kappa values were classified as follows: 0.0-0.2, weak agreement; >0.2-0.4, considerable agreement; >0.4-0.6, moderate agreement; >0.6-0.8, substantial agreement; >0.8-1.0, almost perfect agreement (20).
Results
This study included 65 patients diagnosed with LARC, with an average age of 64 years (range 44-88 years). Of these patients, 71% were male. 74% had an ECOG PS of 0, 23% ECOG PS 1 and 3% ECOG PS 2. Tumours were located in the lower rectum in 35% of cases, in the middle rectum in 54%, and in the upper rectum in 11%.
The administered treatment involved a long course RT for 91% of patients and a short course for 9% (total dose of 25Gy, with 5Gy per fraction). Additionally, 69% of patients received 5-FU and 31% received capecitabine concomitantly. 11% of patients underwent RT as monotherapy.
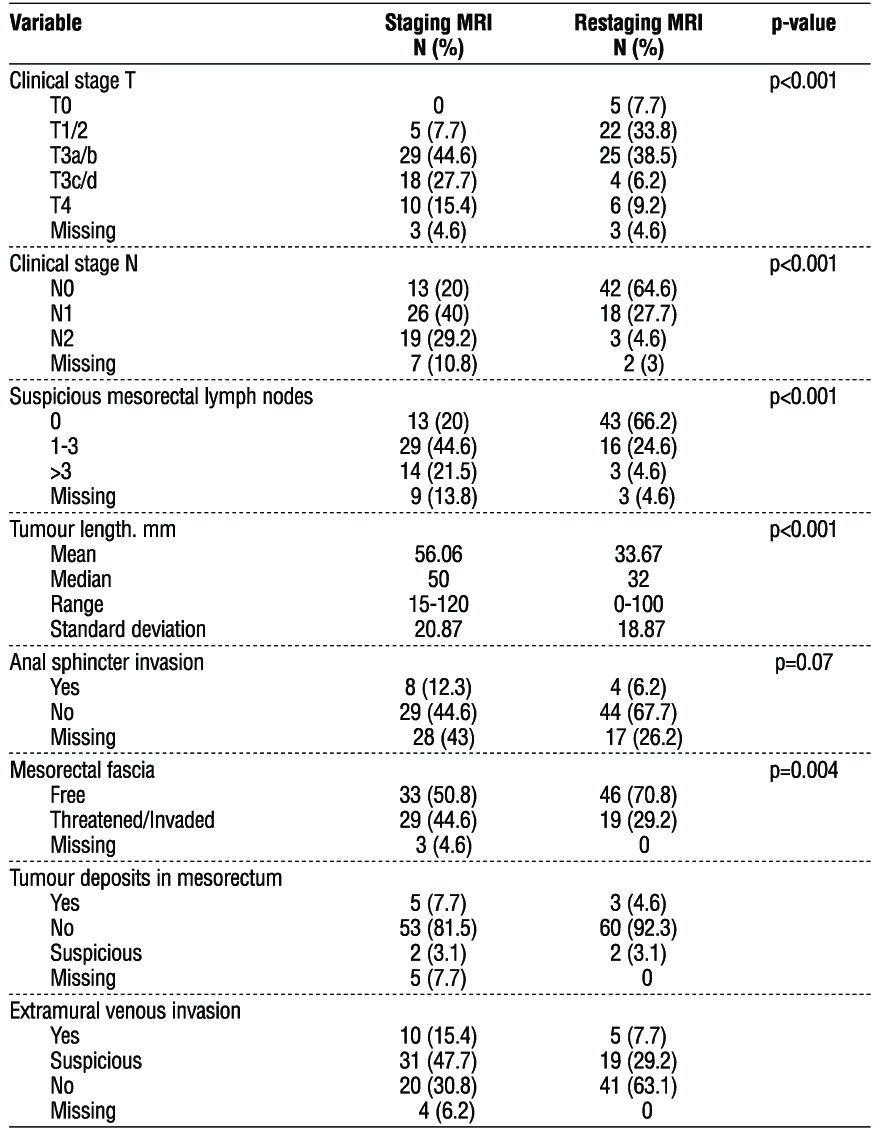
Upon initial MRI assessment, 8.1% (n=5) of the tumours were solid-polypoid, 79% (n=49) were solid-semianular and 12.9% (n=8) had another type of unspecified morphology. No mucinous tumours were detected. The average time between completion of NAT and the restaging MRI was 8 weeks (range 6-11 weeks). The characteristics of staging and restaging MRI are illustrated in table 1.
Table 1 - Characteristics of staging and restaging MRI
Imaging response to neoadjuvant treatment
The comparison between the staging and the restaging MRI revealed significant differences in clinical stage T (Z=5.03, p<0.001), N (Z=-5.15, p<0.001), the number of suspicious mesorectal lymph nodes (Z=-5.24, p<0.001), and MRF status (p=0.004). Out of the 59 patients, 30 (51%) had a reduction in T stage after NAT, while 29 (49%) maintained the same stage. In terms of N stage, 35 (60%) experienced a decrease, only 2 (3%) experienced an increase, and 21 (36%) showed no change. 33 patients (59%) had a reduction in the number of suspicious mesorectal lymph nodes, while 22 (39%) remained unchanged.
Out of the 29 patients with threatened/invaded MRF, 14 (48%) subsequently had free MRF. Out of the 33 patients with free MRF, 2 (6%) had threatened/ invaded MRF. The MRF status remained unchanged for 46 individuals.
Differences in tumour length were also observed after NAT [t(56)=10.35, p<0.001)]. On restaging MRI, tumour length was shorter (M=33.67 mm, SD=18.87) than on staging MRI (M=56.68 mm, SD=21.05).
The difference in anal sphincter status was marginally significant (p=0.07). Of the 8 patients with anal sphincter invasion on the initial MRI, only 1 still showed invasion on the restaging MRI. Twenty-eight patients showed no change in anal sphincter status after NAT.
Patients with tumour deposits in the mesorectum tended to retain these deposits or suspicion of deposits after NAT (adjusted residual = 4.8 and 2.2, respectively). Patients suspected of having extramural venous invasion tended to maintain this suspicion after NAT (adjusted residual = 2.5).
Based on the restaging MRI, we achieved a complete response rate of 3.8% (2/52) and an almost complete response rate of 23.1% (12/52). In the remaining cases (38/52, 73.1%) there was a residual mass and/or focal hypersignal on diffusion-weighted images or tumour remnant.
Restaging MRI versus histopathological study
All patients underwent total excision of the mesorectum. The average time between the completion of RT and surgical resection was 12 weeks (range, 5-15 weeks).
Tables 2, 3 and 4 show the comparison between the restaging MRI and the histopathological findings for tumour and lymph node staging, as well as circumferential resection margin status.

MRI correctly staged the primary tumour in 38 out of 64 patients after NAT, with an accuracy of 59.4% based on histopathological findings. Overstaging occurred in 34.4% (22/64) of cases, while understaging occurred in only 6.3% (4/64). Among the 22 patients who were overstaged with MRI, 91% (n=20) had pathological tumour stages of T0, T1 or T2.
The accuracy rate for restaging lymph nodes using MRI was 65.1% (41/63). Overstaging occurred more frequently (22.2%, 14/63) than understaging (12.7%, 8/63), which was consistent with primary tumour restaging.
Finally, MRI had an accuracy of 77.1% (37/48) in restaging the circumferential resection margin status, with a positive predictive value of 56.3% and a negative predictive value of 87.5%. The sensitivity and specificity of MRI in this context were 69.2% and 80%, respectively.
The agreement between the restaging MRI and the anatomopathological study was moderate for tumour staging and circumferential resection margin status (K=0.58 and K=0.46, respectively, p=0.001), and low for lymph node staging (K=0.34, p=0.005).
The anatomopathological complete response rate was 22.6% (14/62). Restaging MRI overstaged 10 patients with stage ypT0, 7 as ycT1/2 and 3 as ycT3. Additionally, 13 patients with stage ypN0 were overstaged on restaging MRI, 12 as ycN1 and 1 as ycN2. Conversely, one patient was staged as ycT0 on MRI when histologically it corresponded to a ypT1/2. Furthermore, 7 patients with ypN1 staging were understaged as ycN0 on the restaging MRI.
Discussion
NAT has been proven to reduce the size of the primary tumour and malignant lymph nodes in LARC. (16,21) Our analysis revealed that 51% of patients experienced a reduction in T stage and 60% in N stage (p<0.001) when evaluated with MRI. Restaging rectal cancer after NAT enables identification of distant metastases that may impact treatment strategy. It assists in surgical planning and determining the need for additional therapy or the possibility of avoiding surgery in certain patients. However, commonly used imaging techniques in clinical practice, such as MRI, CT scans, and endoscopic ultrasound, have shown limited accuracy in this evaluation (22).
Local tumour status
Multiple studies have investigated the accuracy of MRI in identifying T and N stages in rectal cancer after chemoradiotherapy treatment. However, the accuracy of T stage was found to be moderate, ranging from 43% to 60% (23). This low accuracy can be attributed to several factors, including necrosis and regression of the rectal tumour due to NAT, as well as fibrosis, necrosis, and other pathological reactions of the connective tissue. This makes it difficult to differentiate between tumour tissue, fibrotic scar tissue and normal intestinal wall tissue (17,22).
Additionally, on diffusion-weighted images, inflammatory cell infiltration may appear with high signal intensity in fibrotic areas, which can be similar in appearance to residual tumour. Oedema of the mucosa and submucosa adjacent to the tumour may also be mistaken for residual tumour due to slightly hyper-intense signal on T2-weighted images. This can lead to a tendency to overstage ypT0-2 lesions on MRI assessment (16,17). Our study yielded results consistent with previous investigations. We found that MRI after NAT correctly staged the primary tumour in 38 out of 64 patients, with a moderate accuracy of 59.4% based on the correlation between histopathological findings and MRI. Most of the remaining cases were overstaged (34.4%), with 91% of these having stage ypT0-2.
Lymph node involvement
Previous studies have reported MRI accuracy values for lymph node restaging ranging from 51% to 81%. Additionally, they indicate that MRI assessment after NAT generally results in lymph node overstaging in around 11-36% of cases, while understaging occurs in 2-19% of cases (24). These findings are comparable to our results, where the accuracy of MRI in our population was 65.1%. Lymph node overstaging occurred in 22.2% and understaging in 12.7% of cases.
Traditionally, lymph nodes were assessed primarily based on size (16). Studies have suggested cut-offs for distinguishing between benign and malignant nodes after NAT (24). However, it is important to note that in rectal cancer, there is a high incidence of microscopic metastases in nodes that appear normal. Additionally, patients may present with reactive mesorectal lymph nodes that have increased dimensions (25). Brown et al. found that MRI accuracy in rectal cancer after chemoradiotherapy was low [69% (56/81)] when using a 5 mm cut-off for lymph node size. This was due to significant overlap in the size of benign and malignant lymph nodes (26). In a prospective study of 53 patients, Barbado et al. reported a sensitivity of 57% and specificity of 73% when using the same 5 mm cut-off for lymph node size (24).
Other morphological characteristics have demonstrated greater specificity in detecting lymph node involvement, such as irregular shape and contour and abnormal signal intensity, particularly signal intensity similar to that of a rectal tumour (16). However, assessing contour and tumour heterogeneity in small lymph nodes is challenging (23,24).
Although the ideal size cut-off is still debated, ESGAR recommends a short-axis diameter ≥ 5 mm in the identification of positive nodes after chemoradiotherapy (19). In our study, we assessed pre-NAT lymph nodes based on size criteria and morphological characteristics, such as round shape, irregular contour and heterogeneous signal. Post-NAT lymph nodes were assessed based solely on size criteria, following ESGAR’s recommendation.
Circumferential resection margin involvement
The status of the circumferential resection margin is a strong predictor of prognosis in rectal cancer. The presence of positive radial surgical margins significantly increases the risk of local recurrence and distant metastasis, resulting in worse overall survival (27).
Chemoradiotherapy has been demonstrated to decrease tumour size and increase the probability of negative circumferential resection margins (27). Our study found a significant difference in tumour length (t(56)=10.35, p<0.001) and MRF status (p=0.004) after NAT, as revealed by MRI. At our institution, we consider a circumferential resection margin to be involved or threatened when the distance between the MRF and the tumour is ≤ 2 mm.
The assessment of the circumferential resection margin with MRI after NAT has shown low positive predictive values (44-57%) and high negative predictive values (91-100%). This difficulty in interpreting MFR involvement is essentially based on fibrotic changes in the tumour bed (28). Our evaluation yielded a positive predictive value of 56.3%, which is consistent with the aforementioned range, while the negative predictive value was slightly lower at 87.5%. Our study had a sensitivity of 69.2%, which is lower than a previous meta-analysis that had a sensitivity of 85.4%. However, our study's specificity was consistent with the value obtained in that meta-analysis, which was 80% (17). Similarly, the accuracy of MRI in terms of circumferential resection margin involvement was identical to the Mercury group's analysis of a subgroup of 97 patients treated with preoperative chemoradiotherapy or long course RT (77% in both)(29).
Detection of complete responses
Following NAT, approximately 10-25% of patients with LARC achieve a pathological complete response (9). Currently, the decision to include these patients in non-invasive therapeutic approaches is based on clinical variables that are known to underestimate the complete response rate (10). On the other hand,inaccurate assessment of tumour response may lead to inappropriate use of organ-preserving treatments with potentially devastating consequences (28).
While rectal examination and endoscopy allow complete response to be assessed at the level of the lumen, restaging MRI provides additional information about the presence of residual tumour in the rectal wall layers, lymph node response and tumour growth (8). Currently, pelvic MRI with T2-weighted and diffusion-weighted images is the most widely accepted technique for identifying complete response, and should be combined with rectal examination and endoscopy (19,30).
Our results were consistent with the literature. The pathological response rate was 22.6%. In both ypT0 and ypN0 stages, there was a predominance of overstaging on MRI. Clinical understaging was less common than overstaging and was more pronounced for lymph nodes.
Our study has some limitations
First, it is a single-centre retrospective analysis with a relatively small sample size. The number of patients with ypT0 and ypT4 was very small, which makes it difficult to assess the accuracy of MRI at these stages. Not all patients underwent the same type of NAT. The majority (89.2%) received chemoradiotherapy, but we also included patients who received only long or short course RT. There were also some inconsistencies in the way the MRI was performed, including 3 MRI machines with different characteristics were used; we didn't routinely use pre-MRI enemas, which are not formally indicated, although they are often used in restaging studies; the reports were based on the assessment of only 1 radiologist.
Conclusions
MRI is essential for evaluating the response to NAT in LARC. However, its accuracy and agreement with anatomopathological studies are limited. In restaging, MRI accuracy was 59.4% for stage T, 65.1% for stage N, and 77% for circumferential resection margin involvement. Agreement with anatomo-pathological studies was moderate for tumour staging and circumferential resection margin status, and low for lymph node staging. Overstaging was the main cause of inaccuracies in the T and N stages, especially in ypT0-2 tumours. Therefore, therapeutic decisions after NAT should not rely solely on this examination. Although MRI faces difficulty in distinguishing fibrosis from residual tumour, emerging techniques such as PET/MRI could be useful in restaging rectal cancer.
Conflicts of interest and source of funding
The authors declare no conflicts of interest or sources of funding in this paper.
Ethics approval
The authors declare that the procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and to the 2013 Helsinki Declaration of the World Medical Association.
References
1.Li X, Fu R, Ni H, Du N, Wei M, Zhang M, et al. Effect of Neoadjuvant Therapy on the Functional Outcome of Patients With Rectal Cancer: A Systematic Review and Meta-Analysis. Clin Oncol R Coll Radiol G B. 2023;35(2):e121–34.
2.Bayani R, Darzikolaee NM, Pashaki AAS, Fadavi P, Hassanlouei B, Garousi M. High Dose Rate Brachytherapy Boost After Chemoradiation in Rectal Cancer Patients: A Retrospective Study. Int J Cancer Manag (Internet). 2022 (cited 2023 May 12);15(5).
3.Garant A, Vasilevsky CA, Boutros M, Khosrow-Khavar F, Kavan P, Diec H, et al. MORPHEUS Phase II-III Study: A Pre-Planned Interim Safety Analysis and Preliminary Results. Cancers. 2022; 14(15):3665.
4.Bahadoer RR, Dijkstra EA, van Etten B, Marijnen CAM, Putter H, Kranenbarg EMK, et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(1):29–42.
5.Cercek A, Roxburgh CSD, Strombom P, Smith JJ, Temple LKF, Nash GM, et al. Adoption of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer. JAMA Oncol. 2018;4(6):e180071.
6.Sun Y, Wu X, Zhang Y, Lin H, Lu X, Huang Y, et al. Pathological complete response may underestimate distant metastasis in locally advanced rectal cancer following neoadjuvant chemoradiotherapy and radical surgery: Incidence, metastatic pattern, and risk factors. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2019;45(7):1225–31.
7.Kwon MJ, Soh JS, Lim SW, Kang HS, Lim H. HER2 as a limited predictor of the therapeutic response to neoadjuvant therapy in locally advanced rectal cancer. Pathol Res Pract. 2019;215(5):910-917.
8.Popita AR, Lisencu C, Rusu A, Popita C, Cainap C, Irimie A, et al. MRI Evaluation of Complete and Near-Complete Response after Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer. Diagn Basel Switz. 2022;12(4):921.
9.Santiago I, Rodrigues B, Barata M, Figueiredo N, Fernandez L, Galzerano A, et al. Re-staging and follow-up of rectal cancer patients with MR imaging when “Watch-and-Wait” is an option: a practical guide. Insights Imaging. 2021;12(1):114.
10.Antunes JT, Ofshteyn A, Bera K, Wang EY, Brady JT, Willis JE, et al. Radiomic Features of Primary Rectal Cancers on Baseline T2 -Weighted MRI Are Associated With Pathologic Complete Response to Neoadjuvant Chemoradiation: A Multisite Study. J Magn Reson Imaging JMRI. 2020;52(5):1531–41.
11.Shi L, Zhang Y, Nie K, Sun X, Niu T, Yue N, et al. Machine learning for prediction of chemoradiation therapy response in rectal cancer using pre-treatment and mid-radiation multi-parametric MRI. Magn Reson Imaging. 2019;61:33-40.
12.Cuicchi D, Castagna G, Cardelli S, Larotonda C, Petrello B, Poggioli G. Restaging rectal cancer following neoadjuvant chemoradiotherapy. World J Gastrointest Oncol. 2023;15(5):700–12.
13.Caturegli I, Molin MD, Laird C, Molitoris JK, Bafford AC. Limited Role for Routine Restaging After Neoadjuvant Therapy in Locally Advanced Rectal Cancer. J Surg Res. 2020;256:317–27.
14.Park H, Kim KA, Jung JH, Rhie J, Choi SY. MRI features and texture analysis for the early prediction of therapeutic response to neoadjuvant chemoradiotherapy and tumor recurrence of locally advanced rectal cancer. Eur Radiol. 2020;30(8):4201–11.
15.Kalisz KR, Enzerra MD, Paspulati RM. MRI Evaluation of the Response of Rectal Cancer to Neoadjuvant Chemoradiation Therapy. Radiogr Rev Publ Radiol Soc N Am Inc. 2019;39(2):538–56.
16.Shaish H, Aukerman A, Vanguri R, Spinelli A, Armenta P, Jambawalikar S, et al. Radiomics of MRI for pretreatment prediction of pathologic complete response, tumor regression grade, and neoadjuvant rectal score in patients with locally advanced rectal cancer undergoing neoadjuvant chemoradiation: an international multicenter study. Eur Radiol. 2020;30(11):6263–73.
17.Jia X, Zhang Y, Wang Y, Feng C, Shen D, Ye Y, et al. MRI for Restaging Locally Advanced Rectal Cancer: Detailed Analysis of Discrepancies With the Pathologic Reference Standard. AJR Am J Roentgenol. 2019;213(5):1081–90.
18.Aryan M, Read T, Goldstein L, Burriss N, Grajo JR, Moser P, et al. Utility of Restaging MRI Following Neoadjuvant Chemoradiotherapy for Stage II-III Rectal Adenocarcinoma. Cureus. 2021;13(10): e19037.
19.Beets-Tan RGH, Lambregts DMJ, Maas M, Bipat S, Barbaro B, Curvo-Semedo L, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018;28(4):1465–75.
20.McHugh ML. Interrater reliability: the kappa statistic. Biochem Medica. 2012;22(3):276–82.
21.Feeney G, Sehgal R, Sheehan M, Hogan A, Regan M, Joyce M, et al. Neoadjuvant radiotherapy for rectal cancer management. World J Gastroenterol. 2019;25(33):4850–69.
22.Liu W, Li Y, Zhang X, Li J, Sun J, Lv H, et al. Preoperative T and N Restaging of Rectal Cancer After Neoadjuvant Chemoradiotherapy: An Accuracy Comparison Between MSCT and MRI. Front Oncol. 2022;11:806749.
23.Engelen SME, Beets-Tan RGH, Lahaye MJ, Lammering G, Jansen RLH, Van Dam RM, et al. MRI After Chemoradiotherapy of Rectal Cancer: A Useful Tool to Select Patients for Local Excision. Dis Colon Rectum. 2010;53(7):979–86.
24.Pangarkar S, Mistry K, Choudhari A, Smriti V, Ahuja A, Katdare A, et al. Accuracy of MRI for nodal restaging in rectal cancer: a retrospective study of 166 cases. Abdom Radiol N Y. 2021;46(2):498–505.
25.Allen SD, Padhani AR, Dzik-Jurasz AS, Glynne-Jones R. Rectal Carcinoma: MRI with Histologic Correlation Before and After Chemoradiation Therapy. Am J Roentgenol. 2007;188(2):442–51.
26.Barbaro B, Fiorucci C, Tebala C, Valentini V, Gambacorta MA, Vecchio FM, et al. Locally Advanced Rectal Cancer: MR Imaging in Prediction of Response after Preoperative Chemotherapy and Radiation Therapy. Radiology. 2009;250(3):730–9.
27.Kulkarni T, Gollins S, Maw A, Hobson P, Byrne R, Widdowson D. Magnetic resonance imaging in rectal cancer downstaged using neoadjuvant chemoradiation: accuracy of prediction of tumour stage and circumferential resection margin status. Colorectal Dis. 2008; 10(5):479–89.
28.Seo N, Kim H, Cho MS, Lim JS. Response Assessment with MRI after Chemoradiotherapy in Rectal Cancer: Current Evidences. Korean J Radiol. 2019;20(7):1003–18.
29.Johnston DF, Lawrence KM, Sizer BF, Arulampalam THA, Motson RW, Dove E, et al. Locally advanced rectal cancer: histopathological correlation and predictive accuracy of serial MRI after neoadjuvant chemotherapy. Br J Radiol. 2009;82(976):332–6.
30.Hawkins AT, Hunt SR. Watch and Wait: Is Surgery Always Necessary for Rectal Cancer? Curr Treat Options Oncol. 2016;17(5):22.
Full Text Sources:
Abstract:
Views: 3975

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.