Surgery, Gastroenterology and Oncology

|
|
Background: Baclofen has been tried in Alcohol Use Disorder (AUD) with liver cirrhosis and is considered safe and efficacious. Acamprosate is another option available to treat AUD, however currently there are no trials comparing baclofen & acamprosate in patients with liver cirrhosis. Hence this study was undertaken to compare the two drugs in maintaining alcohol abstinence in patients with ethanol related liver cirrhosis.
Methods: Patients with cirrhosis of liver secondary to alcohol and actively consuming alcohol were randomized to receive either baclofen or acamprosate for a period of 3 months. A total of 74 patients were included and were followed up prospectively and assessed for abstinence.
Results: Amongst the patients who took baclofen, 20 patients were completely abstinent (54.05%) and 21 patients in the acamprosate group (56.76%) were abstinent at the end of 3 months. There was statistically insignificant difference between patients who were randomized to either baclofen or acamprosate (P=0.440) Both the treatment arms had similar incidence of new onset overt hepatic encephalopathy (P=1.000). Baclofen group had a slightly higher rate of new onset decompensation (29.73%) in the form of ascites or overt hepatic encephalopathy or AKI – Hepatorenal syndrome or Variceal Gastro Intestinal bleed (P<0.05).
Conclusion: Both Baclofen and Acamprosate appear equally effective to maintain remission in Alcohol use disorder patients with cirrhosis of liver.
Introduction
Alcohol is the most common cause of liver cirrhosis (1). Persistent intake of ethanol in people with cirrhosis is associated with high mortality (2). The most effective management strategy for these individuals is to achieve total alcohol abstinence for lifetime. Presently until now baclofen is studied for alcohol abstinence in liver cirrhosis and it was found that baclofen was effective in promoting alcohol abstinence in alcohol dependent patients with liver cirrhosis (3). Acamprosate has been studied in alcoholic patients without cirrhosis and is effective and safe in maintaining abstinence (4). However, currently there are no trials comparing the two drugs – baclofen Vs acamprosate in patients with liver cirrhosis. Hence this study is being undertaken to compare the two drugs in maintaining alcohol abstinence in patients with ethanol related liver cirrhosis. Baclofen, a g aminobutyric acid (GABA) B-receptor agonist, is an effective drug for treatment of craving in alcohol dependent patients. Studies have shown that baclofen reduced alcohol craving. It also enhanced abstinence in alcohol dependent patients (3). Baclofen has low liver metabolism (about 15%) and is mainly excreted by the kidneys (5). Most common side effects of baclofen are nausea, drowsiness, confusion, dizziness and fatigue. No hepatic side-effects have been reported in patients dependent on alcohol (6). Thus baclofen could be an useful drug in maintaining abstinence from ethanol in patients suffering from cirrhosis due to ethanol.
Acamprosate has been a proven safe and well tolerated treatment modality for alcohol dependence since its introduction in 1989 (7). It mainly acts as a glutamatergic antagonist & GABA agonist by normalizing glutamatergic excitation that occurs during alcohol withdrawal (8). A Cochrane review of 24 randomized control trials (n=6915) showed that acamprosate, compared to placebo significantly reduced risk of any drinking and increased the cumulative abstinence duration (CAD). The Cochrane review concluded that acamprosate is safe & effective in promoting continuous abstinence after detoxification in AD patients (8).
Material and Methods
After setting the study protocol, approval was obtained from institutional ethics committee, JSS Medical College, Mysore. The study was conducted in the Department of Medical Gastroenterology, JSS Medical College & Hospital, Mysore, Karnataka between January 2022 – April 2023. Patients with liver cirrhosis secondary to ethanol consumption diagnosed clinically, radiologically (Ultrasound abdomen) and based on laboratory parameters were screened for eligibility to participate in the study. A total of 74 subjects were included in the study.
Sample size
Sample size was calculated assuming the proportion of alcohol abstinence in baclofen received group as 71% and in placebo group as 29% ( As per study Giovanni Addolorato et al (3). The other parameters considered for sample size calculation were 90% power of study and 5% alpha error. The below formula was used for sample size calculation.
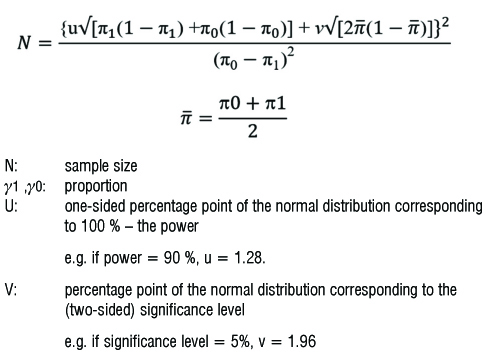
The required number of subjects as per the above-mentioned calculation was 28 in each group. To account for a non-participation rate of about 30% (9 subjects), it was decided to sample 37 subjects in the study (in each group). Alcohol Use Disorder (AUD) was diagnosed based on the criteria set by the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (9). Compared with the previous editions, the terms alcohol abuse and alcohol dependence have been substituted with AUD. Patients admitted to the Department of Medical Gastroenterology, JSS Hospital Mysore, who were diagnosed to have cirrhosis of liver secondary to ethanol satisfying the criteria for Alcohol Use Disorder were screened for eligibility and were included in the study after obtaining informed consent.
Inclusion criteria
Age range 18-75 years; diagnosis of alcohol use disorder according to DSM V criteria; diagnosis of liver cirrhosis on clinical and radiological basis; an alcohol intake of atleast two heavy drinking days per week on average (men > 5 drinks/day, women > 4 drinks per day) and an average overall consumption of 21 drinks per week or more for men and 14 drinks per week or more for women during 4 weeks before enrollment (10); presence of family member able to assist with drug administration and monitoring.
Exclusion criteria
Patients with severe heart or lung disease; abnormal renal functions; malignant disease including HCC; hepatic encephalopathy; treatment with interferon/ corticosteroid within past 60 days; psychopathological illness treated with psychoactive drugs; epilepsy and addiction to drugs other than nicotine were excluded.
Seventy four patients were divided into two study arms (37 subjects in each arm). Randomization was carried out by using computer generated random number and patients were allocated to either arms. Thus, 74 patients were randomized to receive either baclofen or acamprosate. One study arm received tablet baclofen 10 mg thrice daily and the other arm received tab acamprosate 333 mg thrice daily for a period of 3 months. All the patients who were enrolled for the study were admitted in the hospital and received standard medical therapy and work up including compete haemogram, liver function tests (LFT), renal function tests (RFT), HBsAG, Anti HCV, Serum Alpha FetoProtein, Ultrasound abdomen, Upper GI endoscopy for variceal assessment. Psychiatry consultation was taken for deaddiction counselling and to rule out other psychiatric comorbidities. Patients were started on either baclofen or acamprosate prior to discharge after they received atleast two doses of the drug. Patients enrolled were followed up after a week and thereafter monthly for a period of 3 months with blood investigations which included complete blood count, Liver function tests and renal function tests. Patients closest relative was counselled regarding possible side effects like hepatic encephalopathy, reduction in urine output and were asked to report to the hospital incase the patient develops any of the side effects.Patients were also followed up telephonically. At every visit review of drinking, difficulties with treatment adherence, overall functioning and adverse effects were addressed. Patients were instructed to review with empty tablet boxes which served as a marker for treatment adherence. We also provided routine psychological support counseling at every visit.
At the end of 3 months, patient was reevaluated with respect to abstinence from alcohol and side effects that included new decompensation, overt hepatic encephalopathy, acute kidney injury.
Results
Statistical Analysis
Descriptive analysis was carried out by frequency and proportion for categorical variables. Continuous variables were presented as mean ± SD. The chi-square test was used to test the statistically significant difference between two categorical variables. An Independent t-test was used to compare the mean ± SD of continuous variables between the two groups.
P value < 0.05 was considered statistically significant. RStudio Desktop Version 2023.03.0+ 386 was used for statistical analysis. (Reference: RStudio Team (2023). RStudio: Integrated Development for R. RStudio, PBC, Boston, MA URL http://www.rstudio.com/.).
The mean age in baclofen group was 47.73 ± 6.24 and in acamprosate group 48.41 ± 7.33 which were comparable. Majority of the subjects in both the groups belonged to male gender (P=1.000).
The CTP scores between the two arms were comparable. Majority of the patients were in CTP B / C category. Study arms included both compensated and decompensated patients.
The mean MELD – Na score was 22.59 in the baclofen group and 22.38 in the acamprosate group which were comparable.
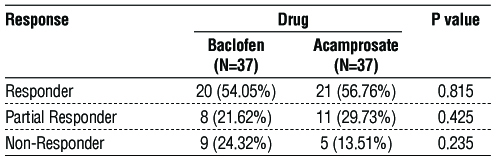
There was statistically insignificant difference in proportion of response between baclofen and acamprosate (p>0.05).
Alcohol relapse (Non-responders) was defined as ethanol intake of atleast two heavy drinking days per week on average (men >5 drinks/day, women > 4 drinks per day) and an average overall consumption of 21 drinks per week or more for men and 14 drinks per week or more for women (11). Response was defined by complete abstinence of ethanol at the end of 3 months. Partial response was defined as any episode of ethanol consumption not classified as relapse i.e unable to achieve complete abstinence.
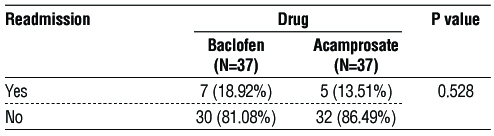
Number of readmissions due to any reason in the two groups were analysed and it was found that patients with baclofen had a slightly higher readmission rate compared to acamprosate although it was not statistically significant (P = 0.528)
Total of five patients had hepatic encephalopathy. Both the groups had similar incidence of new onset overt hepatic encephalopathy during their therapy. Drugs were stopped briefly until the patients completely recovered from encephalopathy. Patients were worked up for precipitating factors, 2/5 had hyponatremia, 1/5 had spontaneous bacterial peritonitis, 2/5 had preceding history of constipation.
Baclofen group had a slightly higher rate of new onset decompensation (n=11, 29.73%) in the form of ascites or overt hepatic encephalopathy or AKI – Hepatorenal syndrome or Variceal Gastro Intestinal bleed as compared to Acamprosate. (P<0.05) The drugs were withheld in patients who developed new onset decompensation (HE / AKI – HRS ) and restarted once the patient was recovered. Patients received standard medical therapy during this course. Whether development of decompensation was due to the natural course of the disease or secondary to drugs could not be ascertained.
Discussion
The final stage of alcohol-related liver disease is cirrhosis where the liver is shrunken & irreversibly scarred. For these subset of patients, abstinence from ethanol is the only intervention which can halt or delay liver disease progression. Patients who maintain abstinence from alcohol for 18 months are 50% more likely to be alive than those who continue to drink (12). All patients with cirrhosis who continue to drink alcohol meet criteria for a diagnosis of AUD, since they continue drinking in the face of adverse health consequences. The mainstay of management for patients with AUD consists of psychosocial interventions and medications. Evidence for use and safety of medications is increasing but advanced liver disease often curtails their use in end-stage ALD. This however, is not the only cause of, underusing AUD treatment in many actively drinking patients with ALD. Many barriers to treatment exist, often related to patient or physician misconceptions such as imprecise perception of drug side effects and belief that an advanced liver disease would complicate the treatment of alcohol use. The most common barriers to treatment include unwillingness to undergo therapy, financial or insurance constraints, and logistic difficulties (13). Psychosocial interventions (PIs) aim at achieving and maintaining alcohol abstinence by encouraging motivation to stop drinking and attaining sustained improvements in drinking outcomes—regardless of the type of patient treated (14).
Table 1 - Demographic parameters between drugs (N=74)
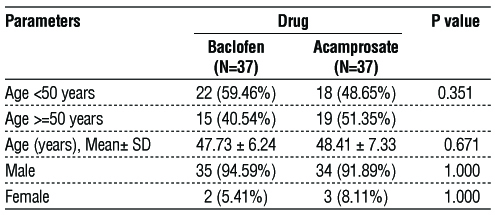
In this study, the mean age in the baclofen group was 47.73±6.24 and in Acamprosate group, it was 48.41±7.33, comparable to a randomized controlled trial by Giovanni Addolorato et al., in which mean age was 49 in baclofen group and 49.5 in placebo group (15). ALD was seen more in males as compared to females in our study cohort (table 1), similar to a metanalysis by Xuanxuan Niu 16 which found global prevalence of ALD in males was six times that in females. The study group (n=74) included alcohol related compensated and decompensated liver cirrhosis. CTP and MELD – Na scores were calculated in both the groups as shown in table 2 and table 3 respectively.
Table 2 - Comparison of CTP score between the two arms (N=74)
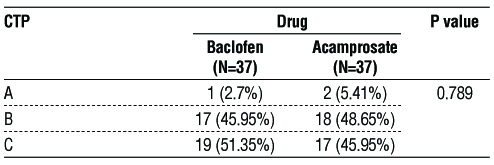
Table 3 - Comparison of mean of MELD-Na score between drugs (N=74)

The primary objective of the study being, number/percentage of patients maintaining alcohol abstinence at 3 months period. It was found that 20/37 (54.05%) patients in the baclofen group & 21/37 (56.76%), P = 0.815 were completely abstinent from alcohol. Both the groups received psychosocial counseling at the time of admission and follow-up. Hence, both drugs were equally efficacious in maintaining abstinence along with psychosocial support in this study. Non-responders i.e relapse, subjects who consumed significant amount of ethanol during the study period were more in the baclofen group as compared to acamprosate (9 and 5 respectively), however the value was not statistically significant (P = 0.235) (table 4 and fig. 1). Abstinence was ascertained only by means of taking history with the patient and closest relative accompanying the patient. No biochemical tests were done to confirm recent alcohol use. In a RCT, comparing baclofen with placebo 15 it was seen that patients allocated baclofen achieved alcohol abstinence (30/42 i.e 71%) were significantly more as compared to placebo (12/42 i.e 29%) P = 0.0001.
Figure 1 - Comparison of response between drugs (N=74)
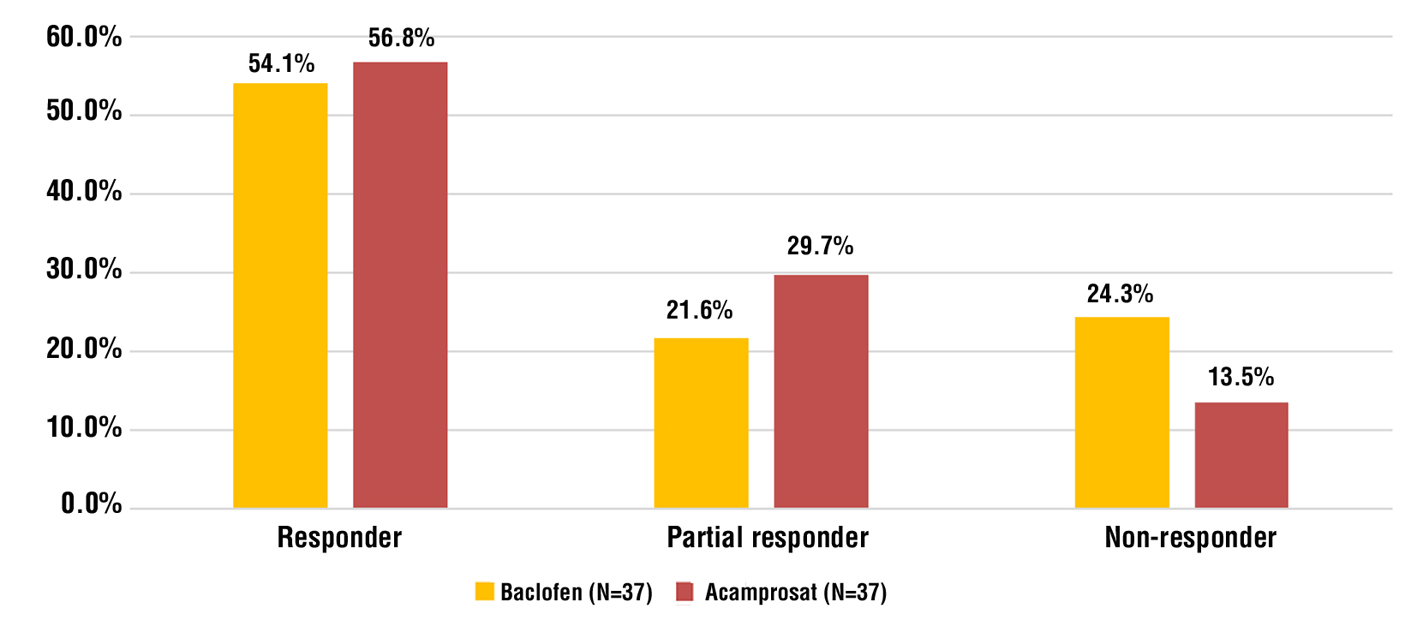
Table 4 - Comparison of response between drugs (N=74)
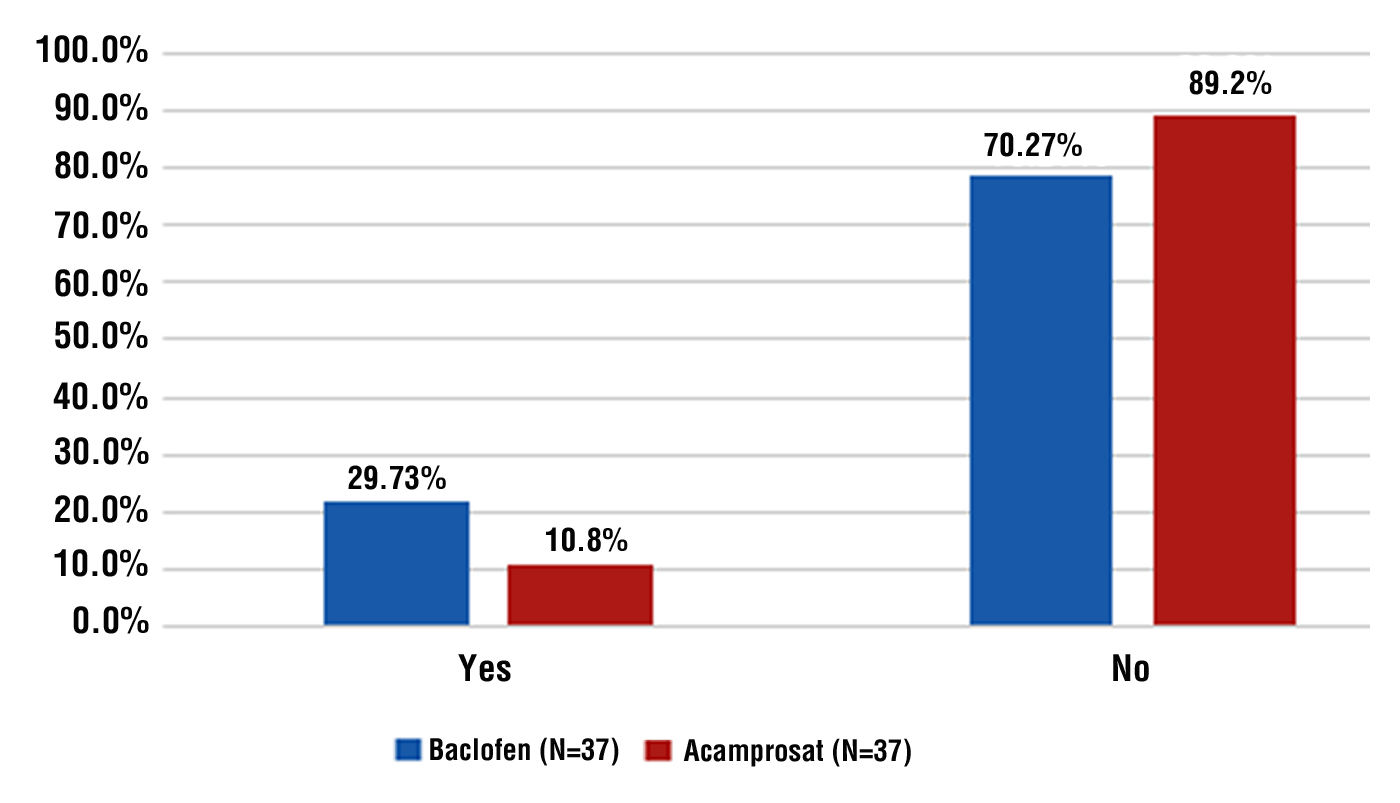
The secondary objectives of the study, was to assess the readmission rates, development of new decompensation in both the groups as shown in table 5 and fig. 2. Readmissions were done due to hepatic encephalo-pathy, gastrointestinal bleed, acute kidney injury – hepatorenal syndrome, ascites requiring paracentesis, spontaneous bacterial peritonitis. Both the groups had similar readmission rates, however in view of advanced liver disease in both the groups, it could not be attributed to either drug alone and may represent the natural course of liver disease. Similarly new onset decompensation was slightly more in the baclofen group as compared to acamprosate group (P<0.05) In a study by Tyson LD et al., acamprosate was associated with fewer unplanned hospital admissions as compared to baclofen, hence could be considered safer despite historical concerns of its use in advanced liver disease (17).
Table 5 - Comparison of Readmission between the arms (N=74)
In a metanalysis by DE Jonas et al., comparing acamprosate and naltrexone, both were associated with reduction of return to drinking alcohol and there was no statistical difference between the two drugs for controlling alcohol consumption (18). However, since naltrexone is metabolized in the liver, concerns remain regarding hepatotoxicity and its use in CTP B and C patients unlike acamprosate which is exclusively metabolized in the kidneys.
Figure 2 - Comparison of New Decompensation between drugs (N=74)
The BacALD trial, examined the effects of baclofen at either 10 mg 3 times daily or 25 mg 3 times daily for 12 weeks in a cohort of patients with and without ALD. Abstinence rates were similar between the baclofen 30- and 75-mg groups (21% and 23% respectively, p = 0.15) with improvement over placebo (10%). More patients had adverse events in the baclofen 75-mg group, with 51% reporting significant sedation or drowsiness (19). Since hepatic encephalopathy is a major complication of advanced liver disease, regular monitoring of patients is needed if the patient is on either baclofen or acamprosate. In addition, these drugs should be used in caution with deranged renal functions since both are metabolized in the kidneys. eGFR should be calculated in every patient, as creatinine alone may not reflect the actual renal function in patients with advanced liver disease as these patients have concomitant sarcopenia.
Currently, AASLD recommends acamprosate at a dose of 333 mg thrice a day as starting dose with effective dose being 666mg thrice a day and baclofen 5 mg thrice a day as a starting dose with effective dose ranging from 5-20 mg thrice a day for management of AUD in liver disease (20). A multidisciplinary approach with pharmacological and psychosocial support is the most effective strategy for the management of AUD; with focus on reducing alcohol intake, promoting long-term abstinence, and preventing relapse (21) which would add to the period of transplant free survival among patients with advanced liver disease. The limitations of the study are small sample size, second absence of a control or a placebo arm, third we relied exclusively on history for abstinence assessment and not biomarkers for alcohol use as some patients may not reveal alcohol consumption owing to the stigma associated with it. Larger multi-center controlled studies are needed to prove the utility of pharmaco-therapy in AUD in AALD. Further studies are needed to determine the duration and optimal dose of treatment needed.
Conclusion
Our results suggest that both Baclofen and Acamprosate may be equally efficacious in the management of AUD in patients with liver disease along with psychosocial support.
Conflict of interests
All author declare that they have no conflict ofinterest.
Funding
No funding sources.
References
1.Tilg H , Day CP. Management strategies in alcoholic liver disease. Nat Clin Pract Gastroenterol Hepatol. 2007;4(1):24-34.
2.Pessione F, Ramond MJ, Peters L, Pham BN, Batel P, Rueff B, et al. Five year survival predictive factors in patients with excessive alcohol intake and cirrhosis. Effect of alcoholic hepatitis, smoking and abstinence. Liver Int. 2003;23(1):45-53.
3.Addolorato G, Leggio L, Agabio R, Colombo G, Gasbarrini G. Baclofen, a new drug for treatment of alcohol dependence. Int J Clin Pract. 2006;60(8):1003-8.
4.Rösner S, Hackl-Herrwerth A, Leucht S, Lehert P, Vecchi S, Soyka M. Acamprosate for alcohol dependence. Cochrane Database Syst Rev. 2010;(9):CD004332.
5.Davidoff RA. Anti spasticity drugs: mechanisms of action. Ann Neurol. 1985;17(2):107-16.
6.Addolorato G, Caputo F, Capristo E, Domenicali M, Bernardi M, Janiri L, Agabio R, et al. Baclofen efficacy in reducing alcohol craving and intake : a preliminary double blind randomized control study. Alcohol Alcohol. 2002;37(5):504-8.
7.Kumar A, Sharma A, Bansal PD, Bahetra M, Gill HK, Kumar R, et al. A comparative study on the safety and efficacy of naltrexone versus baclofen versus acamprosate in the management of alcohol dependence. Indian J Psychiatry. 2020;62(6):650-658.
8.De Witte P, Littleton J, Parot P, Koob G. Neuroprotective and abstinence promoting effects of acamprosate: elucidating mechanism of action. CNS Drugs. 2005;19(6):517-37.
9.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Washington DC; 2013.
10. Litten RZ, Falk DE, Ryan ML, Fertig J, Leggio L. Advances in pharmacotherapy development: human clinical studies. Handb Exp Pharmacol. 2018:248:579-613.
11. Dumortier J, Guillaud O, Adham M, Boucaud C, Delafosse B, Bouffard Y, et al. Negative impact of denovo malignancies rather than alcohol relapse on survival after liver transplantation for alcoholic cirrhosis: a retrospective analysis of 305 patients in a single center. Am J Gastroenterol. 2007;102(5):1032-41.
12. Xie Y-D, Feng B, Gao Y, Wei L. Effect of abstinence from alcohol on survival of patients with alcoholic cirrhosis: a systematic review and meta-analysis. Hepatol Res. 2014;44(4):436-49.
13. Mellinger JL, Scott Winder G, DeJonckheere M, Fontana RJ, Volk ML, Lok ASF, et al. Misconceptions, preferences and barriers to alcohol use disorder treatment in alcohol-related cirrhosis. J Subst Abuse Treat. 2018;91:20-27.
14. O’Donnell A, Anderson P, Newbury-Birch D, Schulte B, Schmidt C, Reimer J, et al. The impact of brief interventions in primary healthcare: a systematic review of reviews. Alcohol Alcohol. 2014;49(1): 66-78.
15. Addolorato G, Leggio L, Ferrulli A, Cardone S, Vonghia L, Mirijello A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: randomised, double-blind controlled study. Lancet. 2007; 370(9603):1915-22.
16. Niu X, Zhu L, Xu Y, Zhang M, Hao Y, Ma L, et al. Global prevalence, incidence, and outcomes of alcohol related liver diseases: a systematic review and meta-analysis. BMC Public Health. 2023; 23(1):859.
17. Tyson LD, Cheng A, Kelleher C, Strathie K, Lovendoski J, Habtemariam Z, et al. Acamprosate may be safer than baclofen for the treatment of alcohol use disorder in patients with cirrhosis: a first description of use in real-world clinical practice. Eur J Gastroenterol Hepatol. 2022;34(5):567-575.
18. Jonas DE, Amick HR, Feltner C, Bobashev G, Thomas K, Wines R, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311(18):1889-900.
19. Rombouts SA, Baillie A, Haber PS, Morley KC. Clinical predictors of response to baclofen in the treatment of alcohol use disorder: results from the BacALD trial. Alcohol Alcohol. 2019;54(3):272-278.
20. Mellinger JL, Fernandez AC, Winder GS. Management of alcohol use disorder in patients with chronic liver disease. Hepatol Commun. 2023;7(7):e00145.
21. Addolorato G, Mirijello A, Barrio P, Gual A. Treatment of alcohol use disorders in patients with alcoholic liver disease. J Hepatol. 2016;65(3):618-30.
Full Text Sources:
Abstract:
Views: 8249

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.