Surgery, Gastroenterology and Oncology

|
|
CASE DESCRIPTION
A 59-year old Caucasian female patient presented to our surgical admissions unit with vague abdominal pain, abdominal distension and progressive constipation, with dependence on laxatives. Her past medical history was unremarkable and she had no previous abdominal or pelvic surgery. Clinical examination revealed a moderately distended abdomen, with palpable fullness in the left upper quadrant of the abdomen, as well as the left hypogastrium. Her admission blood tests were within normal range. Of note, the patient had been investigated with a flexible sigmoidoscopy, as well as completion colonoscopy, due to her altered bowel habits, which reported a non-critical segmental narrowing proximally to the sigmoid colon. The patient was scheduled for a computed tomography (CT) and subsequently magnetic resonance (MR) scans of her abdomen and pelvis, which revealed the presence of a large 14.5x14.0x5.5 cm, probably cystic, lesion of the left-sided colonic mesentery, splaying the inferior mesenteric vessels, as well as the pancreatic tail (figs. 1, 2).
Figure 1 - Compilation of the preoperative CT & MR images, demonstrating the presence of fluid-filled cystic lesion, arising from the mesentery of the descending colon and displacing the pancreatic tail in cephalad position
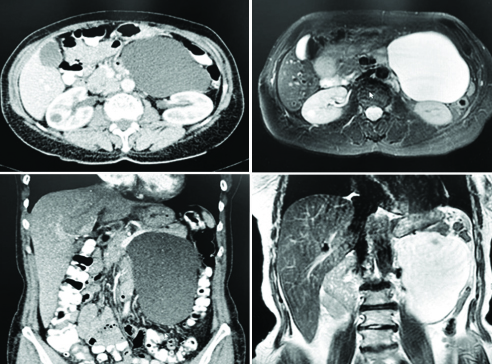

Figure 2 - Intraoperative images of the resected specimen, as well as the residual cavity in the colonic mesentery, adjacent to the pancreatic tail
After obtaining informed consent, the patient was scheduled for exploratory laparotomy. During the procedure, a benign-looking cystic mass was identified within the mesentery of the descending colon, splaying the mesenteric vessels and abutting the pancreatic tail. Using a combination of sharp and blunt dissection, with minimal use of diathermy, the cystic mass was encapsulated en block. The patient had an uneventful recovery and was discharged on the fourth postoperative day. Histopathological examination of the specimen confirmed the benign nature of the cystic lesion, revealing the presence of normal mesothelial cells only on representative sections of the cyst’s wall.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
No financial support was required for this study.
Data availability statement
All data referred to in the study reside within the manuscript and supplementary material.
Key Clinical Message
Benign mesenteric cysts are very uncommon clinical entities, which can manifestate with extrinsic
compression of the adjacent viscera; surgery remains the mainstay of treatment in cases of iagnostic
dilemmas or progressive relevant symptomatology.
Author contributions
CS & GZ: contributed to the clinical data collection and preparation of the manuscript; OP, VK & AP contributed to the review of the literature and preparation of the manuscript; OP & GZ: contributed to the design of the case report presentation and performed the final revision of the manuscript.
Ethics of approval
For performing this case ethical approval was obtained.
REFERENCES
1. Tan JJ, Tan KK, Chew SP. Mesenteric cysts: an institution experience over 14 years and review of literature. World J Surg. 2009;33(9): 1961-5.
2. Ousadden A, Elbouhaddouti H, Ibnmajdoub KH, Harmouch T, Mazaz K, Aittaleb K. A giant peritoneal simple mesothelial cyst: a case report. J Med Case Rep. 2011;5:361.
Full Text Sources:
Abstract:
Views: 2403

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.