Surgery, Gastroenterology and Oncology

|
|
Background/Aim: Major complications of biliary surgery, such as laparoscopic cholecystectomy, include bile duct injury. Surgeons with extensive experience in the hepatobiliary system may find it difficult to address severe cases of bile duct injury. The purpose of this research was to assess various therapeutic approaches for bile duct injuries, and to determine which was superior in terms of injury type and presentation time (early or late), as well as improvement in quality of life.
Methods: Research on 80 patients was undertaken at XXX University's Faculty of Medicine. Strasberg's bile duct injuries classification and key presenting features were used to categorize each patient into one of three groups: surgical, endoscopic, or radiological.
Results: In terms of the type of intervention, 25% underwent surgery, 12.5% underwent radiological intervention, and 37.5% underwent endoscopic intervention. However, 25% used a combination strategy. When the endoscopic group was compared to the surgical and radiological groups, the number of complications was much lower. The quality-of-life score showed a statistically significant difference between the groups under investigation; it was higher in the endoscopic and radiological groups than in the surgical group. This study showed that patients who had their bile duct injuries treated non-surgically were satisfied with their results and could function well with minimal pain.
Conclusion: quality of life in patients diagnosed with bile duct injury who are managed with non-surgical treatment is better than surgical management.
INTRODUCTION
Regarding postoperative complications and the requirement for reintervention, the outcome following bile duct injury (BDI) repair in specialized referral centers is often reported to be outstanding (1-7). It is advised that patients be identified and referred to a hepatobiliary center as soon as possible (8). Quality-of-life (QoL) outcomes following BDI are less commonly documented, and prior research findings have been mixed (9-16). According to prior national cohort research conducted in Sweden, patients with mild BDIs—defined as lesions less than 5 mm—that were found and corrected concurrently with cholecystectomy reported QoL that was similar to that of patients who had an uneventful cholecystectomy (9). Similarly, Sarmiento and Hogan found no difference in QoL between BDI and conventional laparoscopic cholecystectomy in the long run (12,14). However, most studies of QoL are conducted at tertiary referral institutions, where more serious injuries and failures following the first repair are more likely to be seen. Even if the functional outcome is good, QoL in both the mental and physical realms may suffer for years following the repair (10,11,13-14). According to a meta-analysis by Landman et al. in 2013 "there is a long-term detrimental effect of BDI on mental health related QoL" (15). An injury's severity and whether patients have surgery to treat it may have an impact on HR-QoL, per a recent meta-analysis by Halle-Smith et al (16). The purpose of this research was to compare the effect of various therapy approaches for bile duct injuries in terms of social and physical results, and quality of life improvement.
PATIENTS AND METHODS
Study context
This study adopted a quasi-experimental design in the period from February 2018 to February 2022 in the General Surgery department at XXX University Hospital.
Study population
After fulfilling the inclusion requirements, 80 patients with confirmed BDI were included in this study. Any patient, regardless of gender, who had sustained a bile duct injury was included. A bile duct injury did not disqualify any patients. Based on the initial thrashes received, patients at the XXX University Hospital tertiary center were categorized into surgical, endoscopic, and radiological groups. Patients were treated in a stepwise manner, starting with endoscopy either alone or in conjunction with radiological access such as percutaneous abdominal drainage (pigtail drainage), and then moving on to surgery unless, in the case of biliary issues such as biliary peritonitis, surgery had already been started.
Methods
The full history of the eligible patients included in this study was obtained, encompassing personal information such as age and gender, as well as comorbidities such as cirrhosis, diabetes, hypertension, and obesity, as well as the cause of the bile duct lesion. Whole Vital indicators (pulse, temperature, blood pressure), clinical manifestation (bile in the drain's output, sepsis, jaundice, abdominal discomfort, fever), injury type, diagnostic test results, diagnostic duration, and referral time were all included in the clinical assessment. Comprehensive radiographic evaluation including abdominal CT, US, and MRCP in addition to standard laboratory testing.
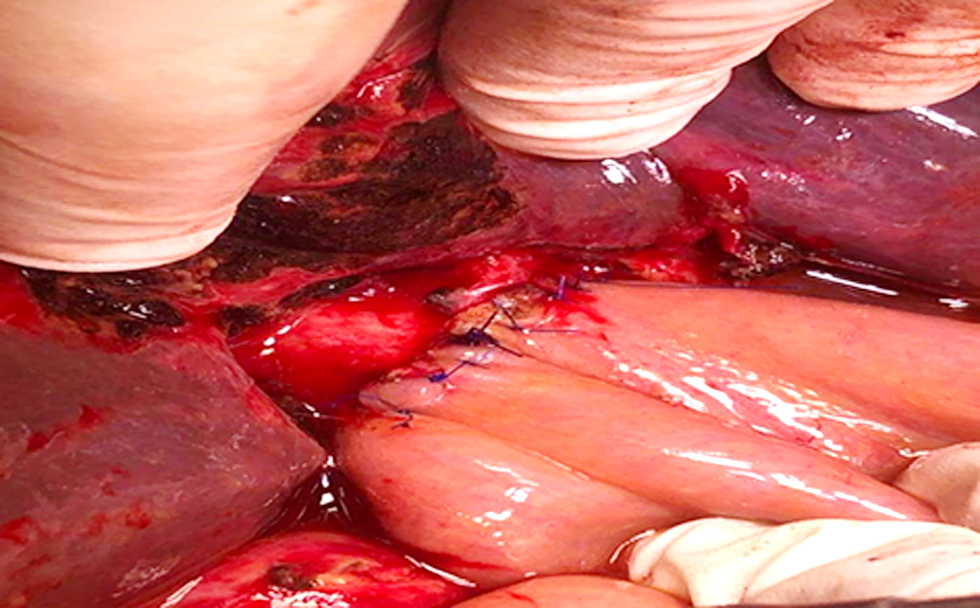
Figure 1 - Operative photograph of one of our cases, creation of end to side – hepaticojejunostomy
Interventions
According to severity of injury in Strasberg classification, interventions were designed as follows; 30 patients were subjected to ERCP (sphincterotomy and stenting)diagnosed with class A and D Strasberg, while 10 patients were subjected to interventional radiological pigtail drainage of biloma and generalized peritoneal biliary collection for class A Strasberg.
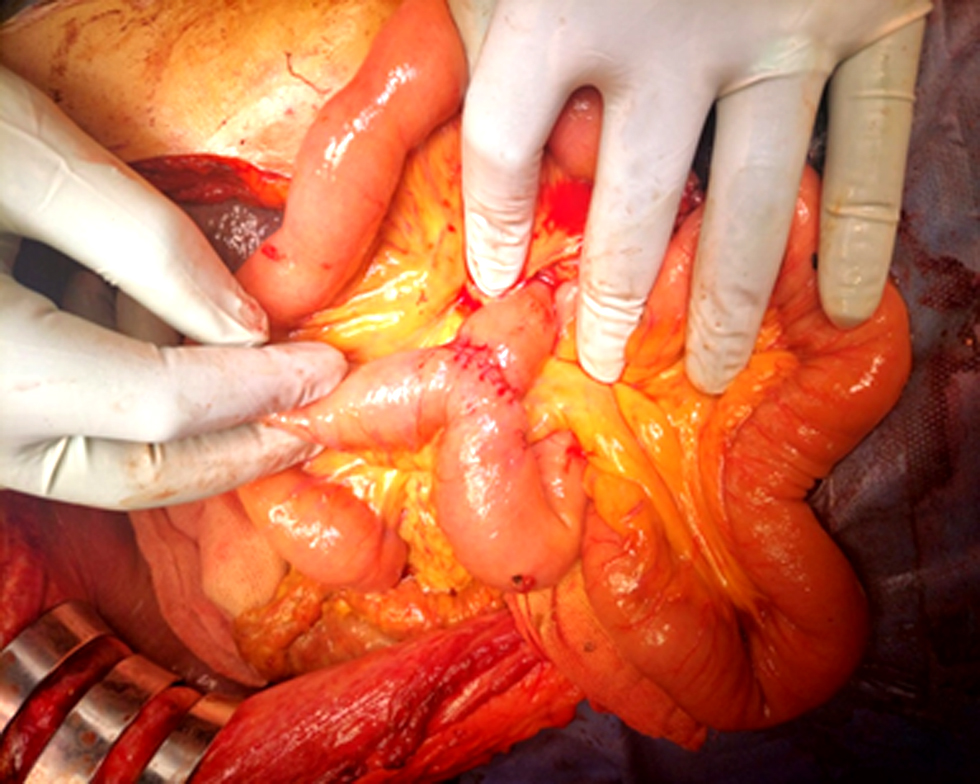
Also 20 patients were treated surgically with bilio-enteric reconstruction for class B, C and E strasberg and with simple repair over t-tube for class D Strasberg (fig. 1 and 2), and 20 patients were treated with a combined approach (more than one modality of management) for class A and E strasberg.
Figure 2 - Operative photograph of one of our cases, entero-enterostomy (jejuno-jejunal)
Complications assessment
Possible surgical complications during or after the occurrence that affected the medical pathway, such as biliary leakage, bleeding, wound bleeding, abdominal collections, biliary peritonitis, and pancreatitis wound infection, were considered a Complication. Post-operative mortality was defined as the number of fatalities that occurred within a period of 30 days of treatment. The term "post-operative morbidity" refers to the occurrence of any procedure-related problems in the first 30 days after surgery. Surgical complications were classified using the Clavien-Dindo system. A full or partial incision was necessary for drainage of infected wounds, such as those in the T-tube tract (17).
Assessment of quality of life
To gauge the general health of our patients, we administered the Short Form-36. It's beneficial since it's a standardized, unified, and straightforward method for gauging quality of life. Self-reporting by patients has made these instruments popular. There are a total of 36 questions on it, and each of the eight scaled scores represents a weighted average of those 36 questions. The eight categories are vitality, physical ability, physical pain, perceptions of overall health, physical role functioning, emotional role functioning, social role functioning, and psychological or emotional well-being. An identical 0-100 scale is generated from each scale. The more disabled one is the lower their score. A score of zero indicates complete disability, whereas a score of 100 indicates complete absence of disability (18).
Follow up
Comprehensive evaluations were conducted at three, six, 12-, and 24-months following surgery, encompassing clinical characteristics, results from biochemistry and radiological laboratory tests, and sub-sequent activities both social and physical.
Data Administration and Statistical Evaluation
Statistical Package for the Social Sciences (IBM-SPSS 20.0) was used to analyze the data after it was imported from the data collection spreadsheets. Quantitative data is typically represented as mean ± SD for groups, while qualitative data is typically represented as numbers and percentages. When comparing two categorical variables, the chi-square test is typically utilized. Normality analysis was conducted using Shapiro-Wilk test. Variables with more than two groups were compared on independent continuous variables, One-Way ANOVA was employed (if the data was normally distributed) and the Kruskal-Wallis test was used (if the data was not normally distributed). P-value < 0.05 denoted statistical significance.
Ethical consideration
IRB approval was obtained from the Medical Ethic Committee, Faculty of Medicine, XXX University (XXX.U./830/9/23). The study was carried out in accordance with the Helsinki Declaration guidelines (19) and in line with STROBE checklist for research ethics. The title and objectives of the study were explained to them to ensure their cooperation. A written informed consent was obtained from the patient before the participation in the study. All collected data was confiential and was used for the purpose of scientific research only. Every research participant had the complete right and freedom to withdraw at any time from the study without any consequences on themedical service provided.

Figure 3 - Pigtail (blue arrow) drainage of post-cholecystectomy bile collection in one of our cases

RESULTS
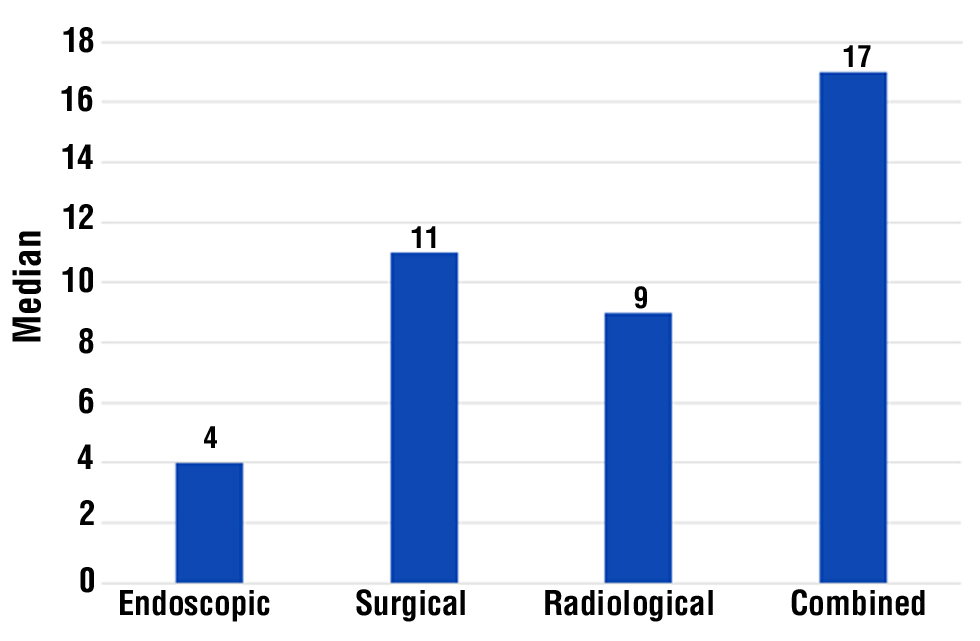
The present investigation consisted of a non-randomized clinical trial (N-RCT) involving a cohort of 80 patients who had been diagnosed with bile duct injury. These patients were selected based on meeting specific inclusion and exclusion criteria. Among the participants, 60 patients (75%) were referred from private clinics and central hospitals, while the remaining 20 patients (25%) were diagnosed with bile duct injury at our tertiary centre, specifically the surgical department of the faculty of medicine at XXX University (tables 1,2 and fig. 3). Table 3 evidenced the presence of a highly significant difference between the groups investigated with respect to hospital stay per day, with the combined group having the longest average hospital stay "median (IQ range) =17 (14-20)" in days while least amount of time in endoscopic group "median (IQ range) =4(3-4)" in days. Also, the success rate in the endoscopic and surgical groups was 100%, while in the radiological and combined group was 80% as described in fig. 4.
Figure 4 - Descriptive analysis of duration of hospital-stay in the studied population
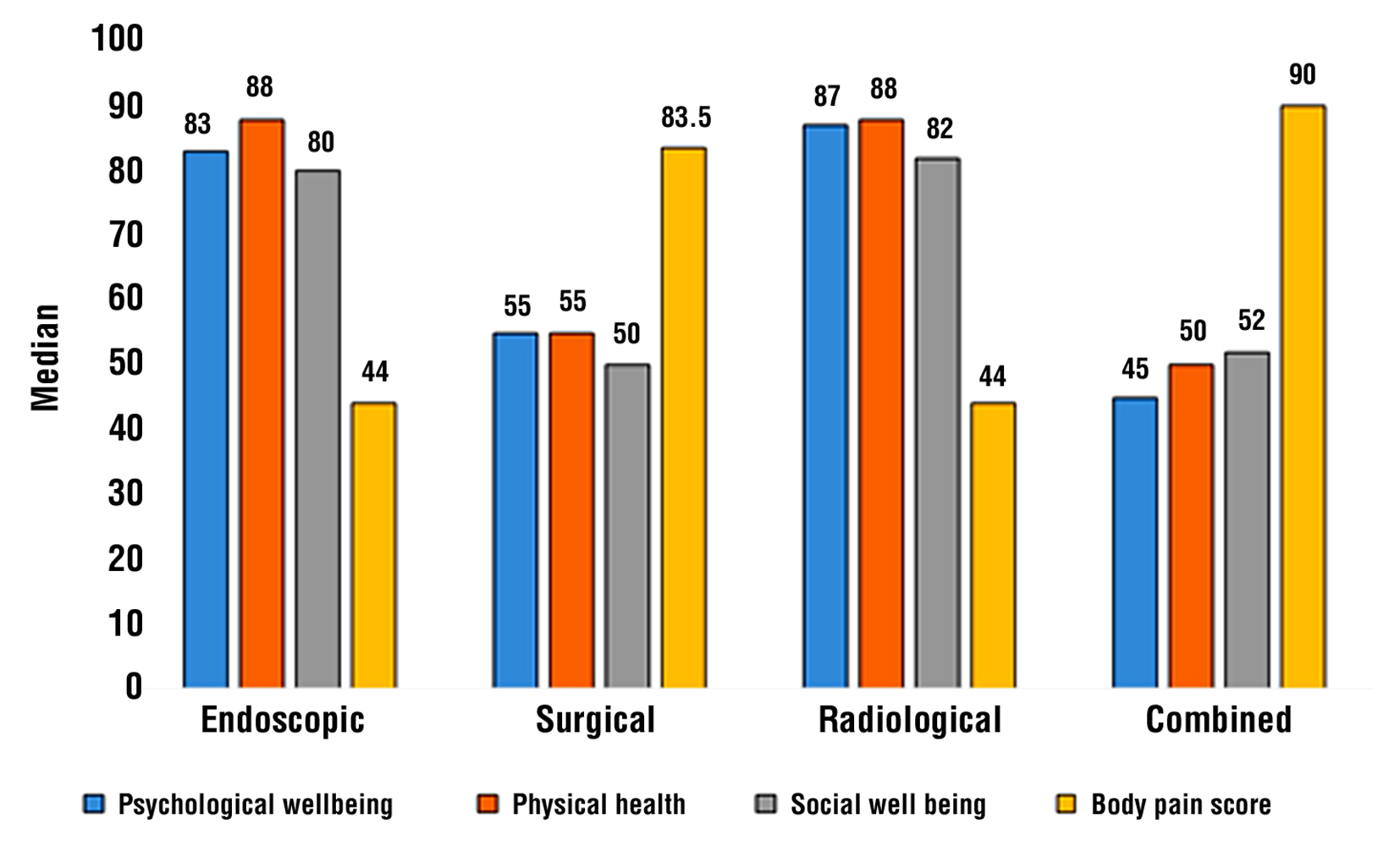
The radiological and endoscopic groups had higher quality-of-life scores than the surgical and combination groups, with very significant differences between the patient groups in terms of (psychological health, physical health, social status, and body pain score). According to our research, patients with bile duct injury who are treated non-surgically report higher levels of happiness and better social interactions, as well as reduced physical pain (table 4 and fig. 5).
Table 3 - Descriptive analysis of outcome in the studied population (n=40)
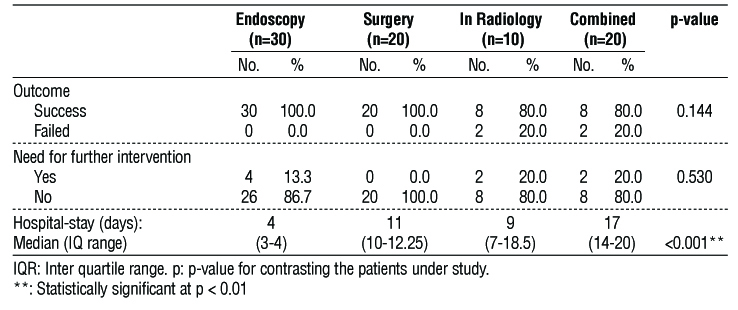
Table 4 - Descriptive analysis of quality of life in the studied patients (n=40)
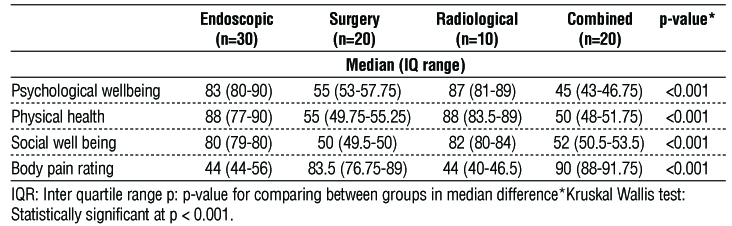
Figure 5 - Descriptive analysis of QOL variables in the studied patients
DISCUSSION
As bile leaks into the peritoneal cavity, bile ascites forms, and if left untreated, can cause peritonitis, sepsis, cholangitis, or an external biliary fistula, BDIs are typically discovered in the postoperative period. Most patients report generic symptoms like vague abdominal pain, nausea, vomiting, and a low-grade fever. The patient may show jaundice and/or cholangitis sometime after the onset of stricture (20). Long-term QoL (as measured by the SF-36) was found to be lower in individuals who underwent BDI reconstruction with a HJ compared to those who underwent cholecystectomy without BDI reconstruction. QoL was also negatively affected by HJ compared to BDI patients who underwent drainage, sutures, or endoscopy for their condition.
Booij et al. observed that patients with HJ and the vast majority of injuries referred to a tertiary hepato-biliary center were less satisfied with their QoL after receiving endoscopic and/or percutaneous treatment, with both studies finding a drop in PCS but no difference in MCS (21). According to a recent meta-analysis, the results of published research on QoL following BDI are still contradictory, with half indicating worse QoL and half showing equal QoL (16). Major BDI and nonsurgical therapy were found to be two potential contributors to diminished QoL. The former is consistent with the results of the current investigation, which links the need for HJ to lower QoL over the long term. After final biliary reconstruction, Otto et al found that 199 patients' QoL improved, while those with post-cholecystectomy inflammatory problems fared worse (22).
Among the cases analyzed, we observed that the mean age was 46 (±15 SD) with a range of 57-69, that 13 (43.3% of the total) were male and 17 (56.7% of the total) were female, that 40% had hypertension, 40% were obese, and that 6.7% had cirrhosis. There were 36 males and 64 females, with an average age is 45.41±11.5 (from 19 to 67) years, as shown by Aziz et al. (23). Sixty-nine patients had coexisting conditions; among them were 27 patients with liver cirrhosis, 24 with obesity, and 18 with abdominal surgery. According to the results of this study, endoscopic procedures accounted for 50% of interventions, surgical procedures for 33.3%, and radiographic procedures accounted for 16.7%. Aziz et al (23) showed that 29 (29.6%) patients who were not surgically treated were managed on an elective basis. The percutaneous draining of the abdomen has been observed to be effective in managing Type A injuries, with a success rate of 7.7% and ERCP and stenting (45.6%) were the most common procedures followed by ERCP and stenting (8.3%) and ERCP in patients with Type C and D injuries. In addition to the 72 patients who underwent Roux-en-Y H.J. surgery (73.4%), Booij et al, (21) discovered that the definitive therapeutic approach has been identified for 398 patients (49.8%) was an endoscopic intervention, 272 patients (34.0%) underwent surgery, and 96 patients (12.0%) underwent radiological intervention.
The main method for treating BDI is using biliary stent therapy yielded a success rate of 15 out of 17 patients, demonstrating no instances of stenosis or leakage, as reported by Khalaf et al (24). The Roux-en-Y procedure was used successfully in all but two patients, who needed additional surgery to fix the problem (stent migration). The duration of the operation and the patient's stay in the hospital were both noticeably lengthened. Through this research, we found that the endoscopic group experienced considerably fewer problems than the radiological and surgical groups (p = 0.002).
In their study, El-Shafei et al, (25) found a higher incidence of complications in the surgical group (53.8% compared to 20% in the endoscopic group; P = 0.05) relative to the endoscopic group. The results of this study showed that the endoscopic group had a marginally higher quality of life than the radiological and surgical groups, but this difference was only significant in the domain of mental health (p = 0.04).
Moreover, Booij et al, (21) conducted a study comparing the SF-36 scores of patients who underwent surgery to those who underwent endoscopy. The results showed that patients who underwent surgery had considerably lower SF-36 scores (median 46.3, IQR 36.3-54.7) compared to those who received endoscopy (median 53.9, IQR 44.3-57.6); the difference was statistically significant with a p-value of less than 0.05.
Also, Mental, and physical QoL were found to be equally unsatisfactory whether patients treated with endoscopy or (major) surgery (26).
Limitations
This study has some limitations, such as a limited sample size, which may have an impact on our results; therefore, larger sample size studies are required to confirm our findings.
CONCLUSION
Non-surgical management yields better physical, social, and emotional outcomes than surgical intervention, with a lower pain scale as a result. For these reasons, we advocate for a conservative approach to bile duct injuries and call for the decision to operate to be made by a multidisciplinary team rather than a single physician because of the negative impact it can have on a patient's quality of life.
Acknowledgement
The authors expressed their thanks for the help and support of the staff members (physicians, nurses, and office workers) of the cardiovascular departments at XXX University Hospital. Also, we acknowledge the eminent role of the participants; their keen participation was the cornerstone of this work.
Author’s contributions
Mohamed A Mohamed (MAM) (ORCID=Not applicable); concept, design, literature search, Operative work, statistical analysis, manuscript preparation, editing and review. Hassan A Abdalla (HAA) (ORCID=Not applicable); design, literature search, manuscript preparation and review. Sara Abdelmohsen (SA) (ORCID=https://orcid.org/0000-0001-5208-5307); literature search, manuscript editing and final draft reviewing. Mahmoud Hasab-Elnabi (MHA) (ORCID= Not applicable): clinical, design, operative work, manuscript preparation and final draft review.
Conflict of interest
The researchers assert that they have no conflicts ofinterest.
Funding sources
No specific grants were awarded to support the current. No relevant financial/non-financial interests to disclose.
Consent to participate
A written informed consent was obtained from the patient before the participation in the study.
Data availability
Data is available upon request from the corresponding author.
References
1.Sicklick J, Camp M, Lillemoe K, Melton G, Yeo C, Campbell K, et al. Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients. Ann Surg. 2005;241(5):786-92; discussion 793-5.
2.de Reuver P, Grossmann I, Busch O, Obertop H, van Gulik T, Gouma DJ. Referral pattern and timing of repair are risk factors for complications after reconstructive surgery for bile duct injury. Ann Surg. 2007;245(5):763-70.
3.Dominguez-Rosado I, Sanford D, Liu J, Hawkins W, Mercado M. Timing of Surgical Repair After Bile Duct Injury Impacts Postoperative Complications but Not Anastomotic Patency. Ann Surg. 2016;264(3):544-53.
4.Perera M, Silva M, Hegab B, Muralidharan V, Bramhall S, Mayer A, et al. Specialist early and immediate repair of post-laparoscopic cholecystectomy bile duct injuries is associated with an improved long-term outcome. Ann Surg. 2011;253(3):553-60.
5.Thomson B, Parks R, Madhavan K, Wigmore S, Garden O. Early specialist repair of biliary injury. Br J Surg. 2006;93(2):216-20.
6.Connor S, Garden O. Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg. 2006;93(2):158-68.
7.Bektas H, Schrem H, Winny M, Klempnauer J. Surgical treatment and outcome of iatrogenic bile duct lesions after cholecystectomy and the impact of different clinical classification systems. Br J Surg. 2007;94(9):1119-27.
8.Khadra H, Johnson H, Crowther J, McClaren P, Darden M, Parker G, et al. Bile duct injury repairs: progressive outcomes in a tertiary referral center. Surgery. 2019;166(4):698-702.
9.Rystedt J, Montgomery A. Quality-of-life after bile duct injury: intraoperative detection is crucial. A national case-control study. HPB (Oxford). 2016;18(12):1010-1016.
10.Boerma D, Rauws E, Keulemans Y, Bergman J, Obertop H, Huibregtse K, et al. Impaired quality of life 5 years after bile duct injury during laparoscopic cholecystectomy: a prospective analysis. Ann Surg. 2001;234(6):750-7.
11.Melton G, Lillemoe K, Cameron J, Sauter P, Coleman J, Yeo C. Major bile duct injuries associated with laparoscopic cholecystectomy: effect of surgical repair on quality of life. Ann Surg. 2002; 235(6): 888-95.
12.Sarmiento J, Farnell M, Nagorney D, Hodge D, Harrington J. Quality-of-life assessment of surgical reconstruction after laparoscopic cholecystectomy-induced bile duct injuries: what happens at 5 years and beyond? Arch Surg. 2004;139(5):483-8; discussion 488-9.
13.Moore D, Feurer I, Holzman M, Wudel L, Strickland C, Gorden D, et al. Long-term detrimental effect of bile duct injury on health-related quality of life. Arch Surg. 2004;139(5):476-81; discussion 481-2.
14.de Reuver P, Sprangers M, Rauws E, Lameris J, Busch O, van Gulik T, et al. Impact of bile duct injury after laparoscopic cholecystectomy on quality of life: a longitudinal study after multi-disciplinary treatment. Endoscopy. 2008;40(8):637-43.
15.Hogan A, Hoti E, Winter D, Ridgway P, Maguire D, Geoghegan J, et al. Quality of life after iatrogenic bile duct injury: a case control study. Ann Surg. 2009;249(2):292-5.
16.Halle-Smith J, Hodson J, Stevens L, Mirza D, Roberts K. Does non-operative management of iatrogenic bile duct injury result in impaired quality of life? A systematic review. Surgeon. 2020;18(2):113-121.
17.Dindo D, Demartines N, Clavien P. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-13.
18.Burholt V, Nash P. Short Form 36 (SF-36) Health Survey Questionnaire: normative data for Wales. J Public Health (Oxf). 2011;33(4):587-603.
19.World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-4.
20.Julian D, Martín S, Martín P, Rodrigo S, Guillermo A, Oscar M, et al. Role of laparoscopy in the immediate, intermediate, and long-term management of iatrogenic bile duct injuries during laparoscopic cholecystectomy. Langenbecks Arch Surg. 2022;407(2):663-673.
21.Booij KAC, de Reuver PR, van Dieren S, van Delden OM, Rauws EA, Busch OR, et al. Long-term Impact of Bile Duct Injury on Morbidity, Mortality, Quality of Life, and Work-Related Limitations. Ann Surg. 2018;268(1):143-150.
22.Otto W, Sierdzinski J, Smaga J, Dudek K, Zieniewicz K. Long-term effects and quality of life following definitive bile duct reconstruction. Medicine (Baltimore). 2018;97(41):e12684.
23.Aziz A, Shoreem H, Sallam A, Al-warraky M, Sadek A, Osman M. Iatrogenic bile duct injury: A retrospective analysis of short-and long-term outcomes after surgical repair. Saudi Surgical Journal. 2016;4(2):61-69.
24.Khalaf A. Management of bile duct injuries: comparative study between Roux-en-Y hepaticojejunostomy and primary repair with stent placement. Journal of The Arab Society for Medical Research. 2013;8(2):89-95.
25.El-Shafei M, Helmy A, Ahmed M. Management of postcholecystectomy biliary injury in Assiut University Hospital clinical audit. Journal of Current Medical Research and Practice. 2020;5(3):322.
26.Boerma D, Rauws E, Keulemans Y, Bergman J, Obertop H, Huibregtse K, et al. Impaired quality of life 5 years after bile duct injury during laparoscopic cholecystectomy: a prospective analysis. Ann Surg. 2001;234(6):750-7.
Full Text Sources:
Abstract:
Views: 2814

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.