Surgery, Gastroenterology and Oncology

|
|
Background: Gastric bypass and sleeve gastrectomy are weight-loss surgeries that significantly reduce obesity, impacting reproductive health by altering total sperm count. Aim: to ascertain the impact of gastric bypass and gastric sleeve surgeries on hormonal levels, reproductive health, and alterations in total sperm count in patients with morbid obesity.
Material and Method: A total of 67 obese patients who had undergone both gastric bypass and gastric sleeve operations were recruited to the study, with an age range of 30 – 60 years, and the study period spanned from January 2022 to April 2023. Comprehensive semen and serum hormone analyses were performed on all patients who had undergone bariatric surgery. Sexual function was evaluated using a questionnaire to determine erectile function in patients after surgery.
Results: The study cohort comprised 67 obese men who underwent gastric bypass or sleeve gastrectomy. Most of the participants were aged between 41 and 50 years, and a high prevalence of dyslipidaemia and smoking was observed. The mean surgical time was 114.63 ± 4.68 minutes, with a mean blood loss of 80.42 ± 5.62 millilitres. The postoperative BMI was significantly reduced in all patients, with a preoperative BMI of 40.3 ± 10.23 and a postoperative BMI of 26.14 ± 2.60 in gastric sleeve surgery and 27.94 ± 2.63 in gastric bypass surgery. The hormonal profile, as indicated by SHBG, total testosterone, and free testosterone, exhibited a notable improvement following gastric sleeve surgery. Postoperatively, orgasmic function and sexual activity demonstrated a marked enhancement, while libido, erectile function, sexual satisfaction, and overall satisfaction exhibited a significant increase at the one-year mark.
Conclusion: Both gastric bypass and gastric sleeve surgeries were regarded as efficacious procedures for substantial weight reduction. This contributed to enhanced fertility outcomes in obese patients and had a favorable impact on reproductive health, resulting in discernible improvements in sperm levels and motility.
INTRODUCTION
Obesity is one of the critical health issues affecting almost the whole world. It has doubled in rank over the past 30 years, thereby making it a global predicament (1,2). Obesity in males has been connected to problems with infertility and disparities in hormones. Perhaps the cause of this connection lies in the way that fatness affects male reproductive hormones. It has been established beyond reasonable doubt that total testosterone, free testosterone, and sex hormone-binding globulin are markedly lower among obese males, while their levels of estradiol are higher (3).
Sermon Dade at al. found that overweight/obese males were more likely to have sperm abnormalities, which makes them infertile. Weight loss due to an altered lifestyle can lead to an increase in free testo-sterone (4) and improve obesity-related metabolic disorders like insulin resistance among obese males, thus leading to sperm functionality (5,6). Bariatric surgery is considered to be the most effective treatment for obesity as of now. It was reported that after surgery, 87% of men with secondary hypogonadism had their gonadal functions resolved due to loss of excess body mass (7-9). There isn’t much information about the impact of natural weight decrease on sperm parameters. However, the few studies available indicate that lifestyle modification can increase sperm quantity and total count, hence improving potential fertility while reducing the conception period (10,11). However, the impact of bariatric surgery is unclear in terms of semen parameters or sexual function (12), where this prospective study aimed at assessing the lasting effects of gastric sleeve surgery on hormones, sexual functions, and sperms in very overweight men who have had problems with infertility (13,14).
MATERIAL AND METHODS
The study involved a cohort of 67 morbidly obese patients who were to undergo sleeve gastric surgery as well as gastric bypass surgery, scheduled between January 2022 and April 2023. The study included patients selected from hospitals in Thi-Qar, Iraq, based on specific surgical criteria and who had additional surgery appointments. The exclusion criteria for our study consisted of patients who were either over 60 years old or under 30 years old, individuals who had renal, hepatic, gonadal, and endocrine disease, patients undergoing concomitant therapy that could impact sex hormone levels or as semen parameters, patients with a history for malignant testicular tumors, trauma as well as dysplasia, and patients with a history of vascular surgery.
All patients who participated in the study underwent before and after examinations in a follow- up period of 12 months. Measurements, including body mass index (BMI), cigarette usage, and any other health conditions, were recorded before to the operation and during the post-operative monitoring period. Dyslipidaemia is defined through the presence of any one of the following: triglycerides equal to or higher than 1.7 mmol/L, a level of high-density lipoprotein cholesterol (HDLc) equal to or lower than 4.14 mmol/L, or past use of lipid-lowering treatment. Percent total weight loss (%TWL) is calculated by subtracting the follow-up weight of the preoperative weight, dividing it by the preoperative weight, and then multiplying the result by 100.
After the operation, all people were examined for semen and hormone analysis for serum. The research was conducted again after 12 months from the date of the surgery. This is the time when this test was designed to allow for recovery from the immediate effects of rapid weight loss, including massive gain in mass and its attendant effect on sperm count. To complete a man's analysis, the patient has to wait for a period of between three days and five days. During each of his visits to the hospital premises, he would ejaculate into a clean container after exciting himself. They were then put in an incubator maintained at 37°C, which is the normal body temperature for humans, followed by a thirty-minute period of liquefaction so that further tests could be done on them. We measured sex hormone-binding globulin (SHBG), follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, testosterone, and estradiol as hormonal parameters. We estimated serum testosterone and prolactin using electrochemi-luminescence immuno-assay; estradiol, FSH, and LH were measured on chemiluminescent microparticle immunoassay (CMIA). We used a chemiluminescent enzyme immunoassay to measure SHBG. Hypogo-nadism was determined by total testosterone measurement and categorical variables. Spearman correlation analysis was applied to establish relationships among observed changes. A significance level of P < 0.05 was considered.
Table 1 - Baseline and preoperative data of patients with obesity.
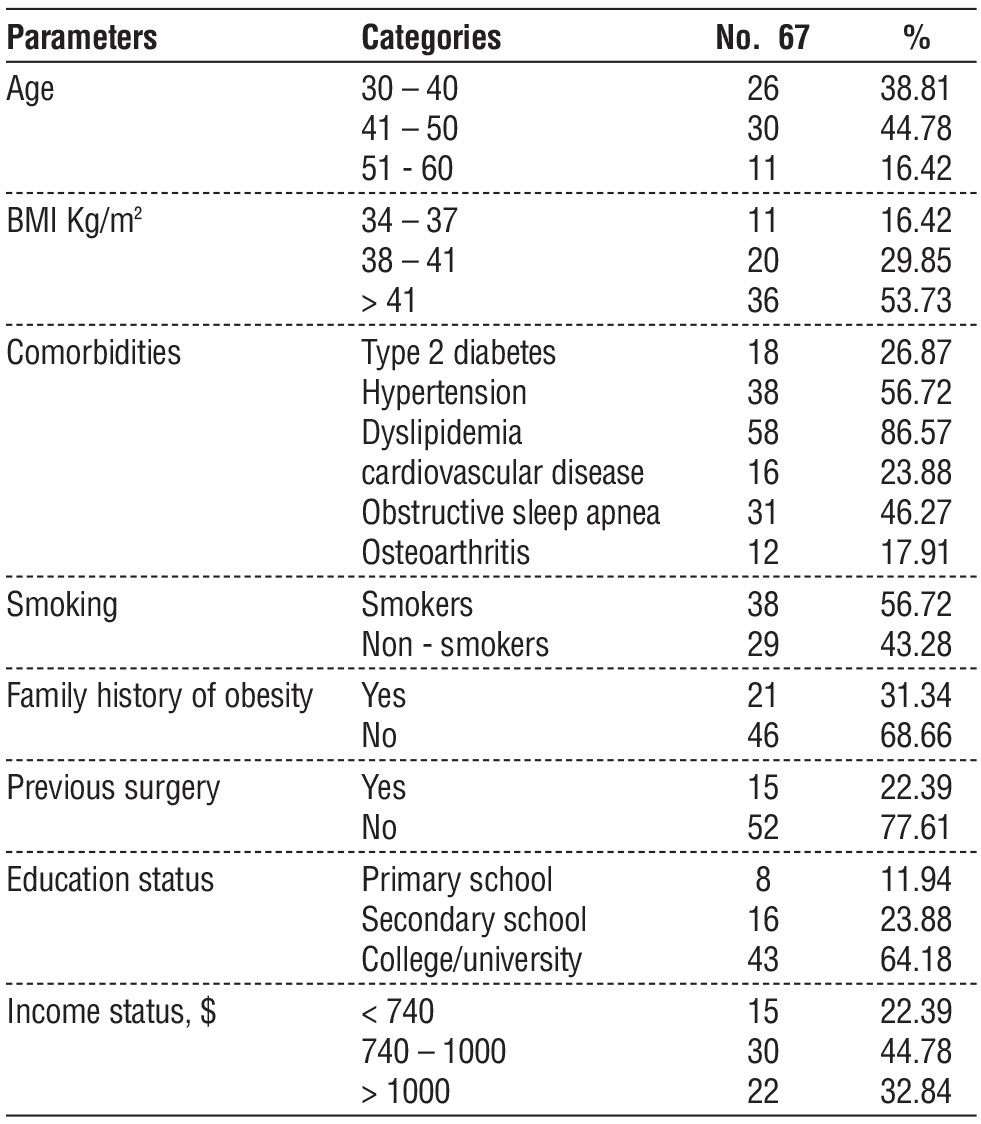
RESULTS
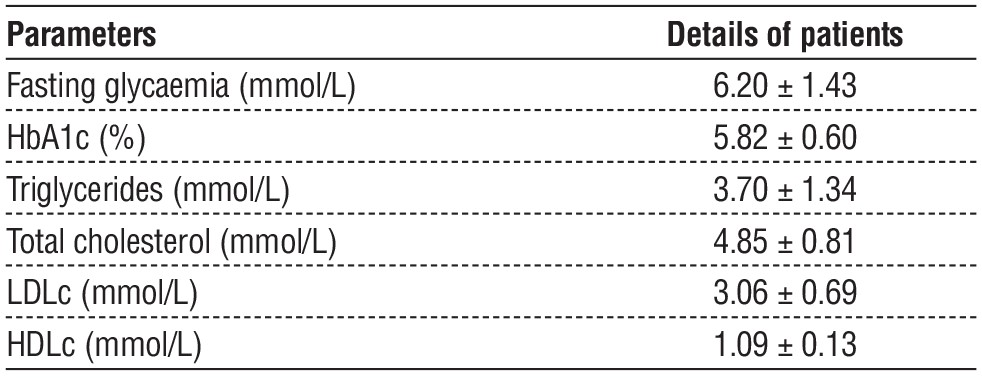
According to table 1, demographic findings enrolled obesity patients’ data, which included 67 men who underwent in both of gastric bypass and sleeve gastrectomy. Patients with ages (41 - 50) years were the highest class of patients, which include 30 cases, BMI classified into (34 – 37) had 11 cases, (38 – 41) had 20 cases, and > 41 with 36 cases, where 86.57% of patients had dyslipidemia, and 56.72% of patients were smokers. Table 2 listed laboratory parameters of obese patients.
Table 2 - Identify diagnoses data of patients with obesity
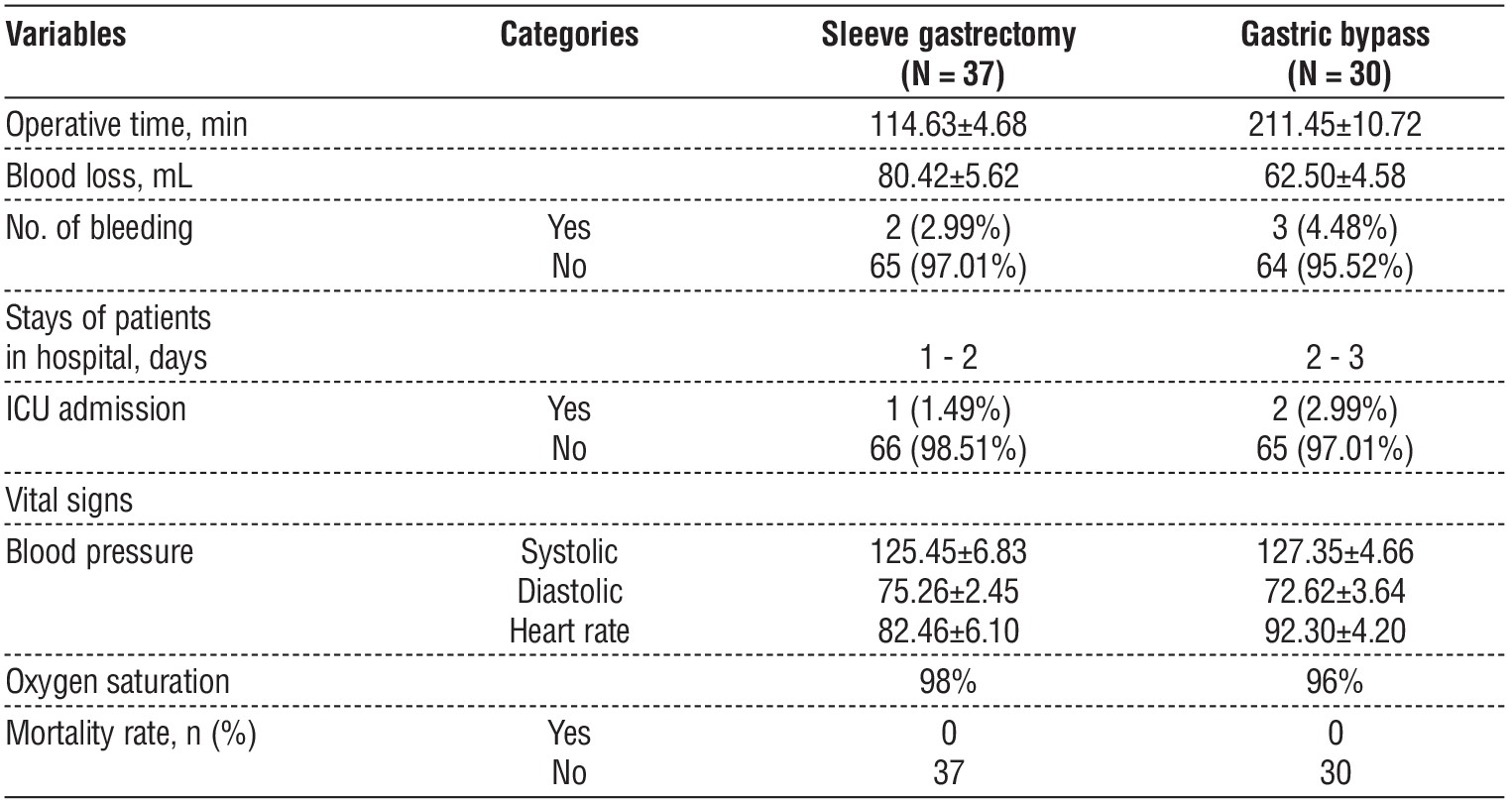
According to the outcomes in table 3, the current findings shown sleeve gastrectomy time was 114.63 ± 4.68 min and, gastric bypass was 211.45 ± 10.72 min, Blood loss had 80.42 ± 5.62 mL, amount of bleeding cases enrolled 2 cases in sleeve gastrectomy surgery and 3 cases in gastric bypass, stays of patients in hospital 1 – 3 days, there is no death cases.
Table 3 - Enrol surgery data related to Gastric bypass and sleeve gastrectomy surgeries
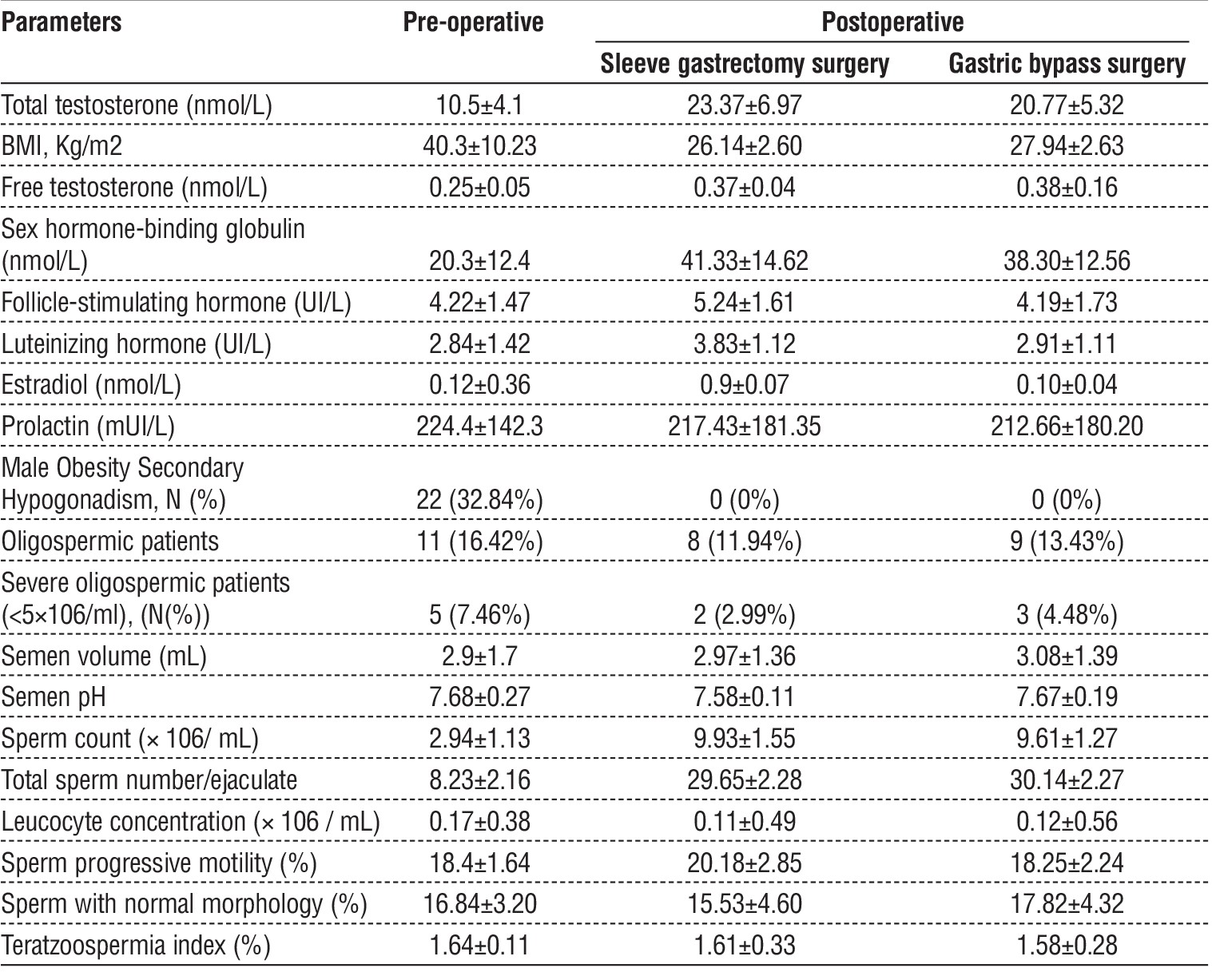
In terms of table 4, our outcomes shown a high reduced of BMI in all patients, in which preoperative BMI was 40.3 ± 10.23, while postoperative BMI in gastric sleeve surgery was 26.14 ± 2.60, and gastric bypass surgery was 27.94 ± 2.63. However, this study realized no significant change among effects with patients having diabetes, hypertension, or obstructive sleep apnea despite losing weight post gastrectomy (OSA) on them. Twenty-two (32.84%) out of 22 patients who had male obesity secondary hypo-gonadism before operation underwent complete regression as a result of postoperative treatment. Hormonal profile on SHBG, total testosterone plus free testosterone significantly improved due to undergoing gastric sleeve surgery 12 months ago. At 12 months after surgery, in the same way, the average total serum testosterone went up from 10.5 ± 4.1 to 23.37 ± 6.97 nmol/l preoperatively, while the average free testosterone increased from 0.25 ± 0.05 to 0.38 ± 0.16/L before operation. This increase was seen in the levels of these hormones, and SHGB was noted following surgery on patients.
Table 4 - Comparison between preoperative hormonal assessment and seminogram and follow- up values at 12- and 18-month post-sleeve gastrectomy surgery.
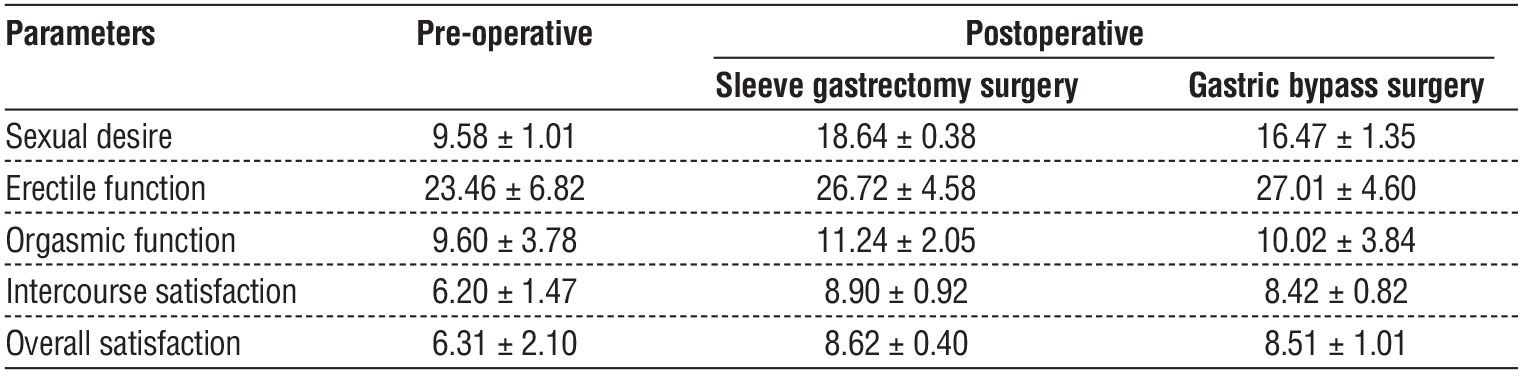
In table 5, our study found that after gastric sleeve surgery and sleeve gastrectomy surgery, orgasmic function improved sexual activity, whereas libido, erectile function, sexual satisfaction, and overall satisfaction increased notably after a year.
Table 5 - Comparison of patients' data between preoperative and postoperative during follow-up in terms of sexual function.
DISCUSSION
Obesity has negative effects on male fertility, and this condition can be blamed on several factors, among them alteration of sexual activity, interruption of hormonal systems (15), deposition of toxic substances within fatty tissues, increased scrotum temperatures, or as a consequence of genetic flaws resulting into defective sperms (16). Weight loss can change the levels of systemic low-grade inflammation, which depends on the mass of the human body (17). This is well supported by the significant changes in 51 inflammation-associated proteins, among them c-reactive protein (CRP) (18).
Many recent studies have highlighted the role of fertility problems caused by obesity and bariatric surgeries. Existing studies show that bariatric surgery may improve some obesity- related co-morbidities like heart diseases, diabetes, or high blood pressure while at the same time greatly reducing the need for drugs and related costs as drugs (19-21). Weight loss plastic surgery might decrease fat accumulation on the thigh and suprapubic regions, decrease testicular temperature, and hence enhance spermatogenesis by cutting down on fat mass after losing weight (22,23). The study’s findings demonstrate that Shaklee energy makes total testosterone, free testosterone, and SHBG levels go up significantly in very obese men, treating male obesity-related secondary hypogonadism (MOSH) (24). After gastric sleeve surgery, levels of sex hormone-binding globulin and free testosterone increase to demonstrate that not all decreases in testosterone concentration are as a result of obesity's effect on SHBG levels and weight loss (25). This current work is in line with other previous literatures researching on how bariatric surgery affects testosterone concentrations in men (26).
Our study found that gastric sleeve surgery improves male reproductive system health metrics without affecting orgasm (27). Erectile function has not been thoroughly explored in existing literature although optimal hormonal surveillance should accompany bariatric surgery procedures too. Nonetheless, these results are in line with earlier studies endorsing weight loss interventions through IIEF parameters (28). Various previous studies have investigated the advantages of significant weight loss post- bariatric surgery. At first, many case studies mostly addressed the harmful impact of roundness surgery for male fertility. Subsequent prospective research using small sample sizes have contradicted these anecdotal results (29).
El Bardisi et al (30). Performed a study on the impact in sleeve gastrectomy on semen parameters. After 12 months, researchers noticed improved sperm motility in men that had previously had low sperm count and absence of sperm in their semen. Samavat et al (31). Saw improvements in both the amount and movement of semen six months after surgery. On the contrary, a decrease in the level of awareness and total number of sperm has been registered in two recent studies. Legro et al., on the one hand, and Reis et al., on the other, found no change in sperm parameters at 12- and 24-months post-surgery (32).
CONCLUSION
In general, both gastric bypass as well as sleeve gastrectomy are related to enhancements of overall sperm count and other sperm characteristics in men who are obese. Sleeve gastrectomy surgery effectively enhances testosterone levels, sexual function, and sperm count for obese men, causing significant weight loss.
Conflict of interest
All authors declared no any conflict of interesting.
Funding
No funding sources.
Ethical Statement
This work approved by Department of Surgery, College of Medicine (No. 12 in 2022).
REFERENCES
-
McCracken K, Phillips DR. Global health: An introduction to current and future trends. Routledge; 2017.
-
Afolabi HA, Zakaria Z, Salleh SM, Ch’ng ES, Nafi SN, Aziz AA, Al-Mhanna SB, Irekeola AA, Wada Y, Daku AB. IntechOpen. Obesity: a prerequisite for major chronic illnesses. InObesity-Recent Insights and Therapeutic Options 2023.
-
Narinx N, David K, Walravens J, Vermeersch P, Claessens F, Fiers T, et al. Role of sex hormone-binding globulin in the free hormone hypothesis and the relevance of free testosterone in androgen physiology. Cell Mol Life Sci. 2022;79(11):543.
-
Wrzosek M, Wo?niak J, W?odarek D. The causes of adverse changes of testosterone levels in men. Expert Rev Endocrinol Metab. 2020; 15(5):355-362.
-
Chaudhuri GR, Das A, Kesh SB, Bhattacharya K, Dutta S, Sengupta P, et al. Obesity and male infertility: multifaceted reproductive disruption. Middle East Fertility Society J. 2022;27(1):8.
-
Cannarella R, Crafa A, Curto R, Condorelli RA, La Vignera S, Calogero AE. Obesity and male fertility disorders. Mol Aspects Med. 2024;101273.
-
Nguyen NT, Varela JE. Bariatric surgery for obesity and metabolic disorders: state of the art. Nat Rev Gastroenterol Hepatol. 2017; 14(3):160-169.
-
Fernandez CJ, Chacko EC, Pappachan JM. Male obesity-related secondary hypogonadism–pathophysiology, clinical implications and management. Eur Endocrinol. 2019;15(2):83-90.
-
Molina-Vega M, Muñoz-Garach A, Damas-Fuentes M, Fernández-García JC, Tinahones FJ. Secondary male hypogonadism: A prevalent but overlooked comorbidity of obesity. Asian J Androl. 2018;20(6):531-538.
-
Guo D, Wu W, Tang Q, Qiao S, Chen Y, Chen M, et al. The impact of BMI on sperm parameters and the metabolite changes of seminal plasma concomitantly. Oncotarget. 2017;8(30):48619-48634.
-
Emokpae MA, Brown SI. Effects of lifestyle factors on fertility: practical recommendations for modification. Reprod Fertil. 2021; 2(1):R13-R26.
-
Lee Y, Dang JT, Switzer N, Yu J, Tian C, Birch DW, et al. Impact of bariatric surgery on male sex hormones and sperm quality: a systematic review and meta-analysis. Obes Surg. 2019;29(1):334-346.
-
Abouelgreed TA, Elatreisy A, El-Sherbeiny AF, Abdelaal MA, Saafan T, Shalkamy O, et al. Long-term effect of sleeve gastrectomy surgery on Hormonal Profile, Semen Parameters and sexual functions of obese infertile men; a prospective observational study. Basic Clin Androl. 2023;33(1):16.
-
Wood GJ, Tiseo BC, Paluello DV, de Martin H, Santo MA, Nahas W, et al. Bariatric surgery impact on reproductive hormones, semen analysis, and sperm DNA fragmentation in men with severe obesity: prospective study. Obes Surg. 2020;30(12):4840-4851.
-
Liu Y, Ding Z. Obesity, a serious etiologic factor for male subfertility in modern society. Reproduction. 2017;154(4):R123-R131.
-
Rahman MB, Schellander K, Luceno NL, Van Soom A. Heat stress responses in spermatozoa: Mechanisms and consequences for cattle fertility. Theriogenology. 2018;113:102-112.
-
Castro AM, Macedo-De la Concha LE, Pantoja-Meléndez CA. Low-grade inflammation and its relation to obesity and chronic degenerative diseases. Revista Médica del Hospital General de México. 2017;80(2):101-5.
-
Rajab IM, Hart PC, Potempa LA. How C-reactive protein structural isoforms with distinctive bioactivities affect disease progression. Front Immunol. 2020;11:2126.
-
Baharuddin DM, Payus AO, Fahmy EH, Sawatan W, Than WW, Abdelhafez MM, et al. Bariatric surgery and its impact on fertility, pregnancy and its outcome: A narrative review. Ann Med Surg (Lond). 2021;72:103038.
-
Pontiroli AE, Zakaria AS, Fanchini M, Osio C, Tagliabue E, Micheletto G, et al. A 23-year study of mortality and development of co-morbidities in patients with obesity undergoing bariatric surgery (laparoscopic gastric banding) in comparison with medical treatment of obesity. Cardiovasc Diabetol. 2018;17(1):161.
-
Schutta MH. Diabetes and hypertension: epidemiology of the relationship and pathophysiology of factors associated with these comorbid conditions. J Cardiometab Syndr. 2007;2(2):124-30.
-
Maia M, Costa Santos D. Body contouring after massive weight loss: a personal integrated approach. Aesthetic Plast Surg. 2017;41(5): 1132-1145.
-
Mineroff J, Nguyen JK, Jagdeo J. Potential treatment modalities for suprapubic adiposity and pubic contouring. Arch Dermatol Res. 2023;315(6):1615-1619.
-
Winters SJ. SHBG and total testosterone levels in men with adult onset hypogonadism: what are we overlooking? Clin Diabetes Endocrinol. 2020;6:17.
-
Emami MR, Safabakhsh M, Khorshidi M, Moghaddam OM, Mohammed SH, Zarezadeh M, et al. Effect of bariatric surgery on endogenous sex hormones and sex hormone-binding globulin levels: a systematic review and meta-analysis. Surg Obes Relat Dis. 2021;17(9):1621-1636.
-
Lee Y, Dang JT, Switzer N, Yu J, Tian C, Birch DW, et al. Impact of bariatric surgery on male sex hormones and sperm quality: a systematic review and meta-analysis. Obes Surg. 2019;29(1):334-346.
-
Xu J, Wu Q, Zhang Y, Pei C. Effect of bariatric surgery on male sexual function: a meta-analysis and systematic review. Sex Med. 2019; 7(3):270-281.
-
Jäger P, Wolicki A, Spohnholz J, Senkal M. Review: Sex-specific aspects in the bariatric treatment of severely obese women. Int J Environ Res Public Health. 2020;17(8):2734.
-
Eisenberg ML, Esteves SC, Lamb DJ, Hotaling JM, Giwercman A, Hwang K, et al. Male infertility. Nat Rev Dis Primers. 2023; 9(1):49.
-
Abouelgreed TA, Elatreisy A, El-Sherbeiny AF, Abdelaal MA, Saafan T, Shalkamy O, et al. Long-term effect of sleeve gastrectomy surgery on Hormonal Profile, Semen Parameters and sexual functions of obese infertile men; a prospective observational study. Basic Clin Androl. 2023;33(1):16.
-
Alipour H, Van Der Horst G, Christiansen OB, Dardmeh F, Jørgensen N, Nielsen HI, et al. Improved sperm kinematics in semen samples collected after 2 h versus 4–7 days of ejaculation abstinence. Hum Reprod. 2017;32(7):1364-1372.
-
Magalhaes DP, Mahalingaiah S, Perry MJ. Exploring the causes of semen quality changes post-bariatric surgery: a focus on endocrine-disrupting chemicals. Hum Reprod. 2022;37(5):902-921.
Full Text Sources:
Abstract:
Views: 5862

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.