Surgery, Gastroenterology and Oncology

|
|
Background: Para-umbilical hernias, a part of the ventral hernias group, are identified close to or right of the umbilicus. Objective: To compare open and laparoscopic surgery with mesh by analyzing differences in complication rates, efficacy, and recurrence in handling para-umbilical hernias.
Methods: This retrospective study was conducted at Al-Yarmouk Teaching Hospital and Al Arabi Privet Hospital in Baghdad, Iraq, on 40 patients with umbilical hernias. Forty patients were divided into two groups: 20 treated with open surgery and 20 treated with laparoscopic mesh tissue repair.
Results: The open procedure group consisted of more males than the laparoscopic group, which had more females. There was no significant difference between the two groups in terms of BMI. The medical history of the patients was the same, where they had hypertension 60 percent of the time and had laparoscopic repair 50% of the time. The incidence of diabetes mellitus, cardiovascular attack, renal failure, or hypothyroidism was not considerably different between the two groups. Of those in the open procedure group, 10% had multiple sclerosis, equalling 5% of the laparoscopic group; thus, there was no significant difference. Seventy% of the patients in the open procedure group had no postoperative
complications, and only 25% in the laparoscopy group had no postoperative complications. There were differences in perioperative characteristics; however, the overall operative time was longer in the open group. However, the open procedure group had a higher rate of wound infection. The recurrence rates approached statistical significance at 20% for the open procedures and 10% for the laparoscopic procedures. Thus, the effectiveness of conversion in the two groups did not vary.
Conclusion: Concerning the post-surgery effects, such as infection and hematoma, there is a clear indication that patients who undergo laparoscopic paraumbilical hernia repair procedures recover much faster than those who undergo an open procedure. Furthermore, most patients with para-umbilical hernia treated with hematoma and seroma are treated with aspiration. The current study and review results support the general premise that laparoscopic surgery may be superior to open surgery in minimizing complications and enhancing recovery, making it the best option for para-umbilical hernia repair. Predictive models must be further investigated to increase their reliability and update the surgical recommendations.
Introduction
Para-umbilical hernias, part of the ventral hernias group identified close or right on the umbilicus, accounted for approximately 10% of all abdominal hernias (1). These hernias are common in children and young adults, although they spontaneously close in the early years of life (2-4).
Many surgical approaches for treating umbilical hernias range from anatomic sutures to prosthetic meshes at different sites, such as inlay, inlay, and replacement sites (5). Of these options, mesh augments have displayed insignificant promise for lowering these rates in suture-based repairs, where recurrence can range from 19-54% (6,7).
Managing para-umbilical hernias in adults has been a subject of changing practice throughout the past 100 years, using several techniques to minimize recurrence and enhance the patient's quality of life (8). Mayo repair, developed by James Mayo in 1901, is classified under the classical repair technique whereby the fascial layer is joined by a double-breasted suture (9-11).
Although improvements have been made in laparoscopic skills and methods of open mesh repair for para-umbilical hernias, the exact applicability of laparoscopic repair remains contentious (12). The conservative laparoscopic technique, known as laparoscopic intraperitoneal onlay mesh (IPOM) repair, has been used for ventral hernia management, but its effectiveness and safety in managing umbilical hernias have not been adequately researched. While many studies have compared the results of open and laparoscopic repair for ventral hernias, patients often have incisional or mixed ventral hernias, not para-autilical hernias (13-16).
This study aimed to determine the comparative effectiveness of open and laparoscopic onlay mesh techniques in managing para-umbilical hernias, emphasizing risk, effectiveness, and recurrence. The results suggest potential improvements to the implementation of ideal procedures for this relatively common yet complex pathology.
Patients and Methods
Study design and setting
This was a retrospective clinical study using a convenience sampling technique conducted in Al-Yarmouk Teaching Hospital and Al Arabi Privet Hospital, Baghdad, Iraq. Patients were recruited from January 2022 to August 2024 using non-randomized selection.
Inclusion Criteria
The study included 40 patients with a para-umbilical hernia who were forwarded to the surgery department. The patients were divided into two groups. All patients had a hernia size less than (4 cm) ecluded form both groups, where 20 patients were treated with open surgery and the other 20 with laparoscopic mesh tissue repair. All patients were fitted with general anesthesia, and those affordable for mesh tissue repair were included in the laparoscopic procedure.
Exclusion Criteria
At the same time, those patients who refused the laparoscopic method and were unfit for general anesthesia. All patients had paraumbilical, supra-, and infra-positions. A defect size of > 4 cm was confirmed by ultrasound.
Procedure
The laparoscope used in this study was obtained from Karl Storz (Germany). During laparoscopy, a Verres needle was inserted at the palmer point of the abdominal wall for CO2 insufflation. Three ports were used: 10 mm for the camera in the left lumbar region, and 5 mm for the left iliac fossa. The third port, the so-called working port in the right hand, introduces the mesh using 11 mm in the left hypochondrium and also for an absorbable tacker (manufactured by Covidean, USA).
In this technique, dual mesh 20 × 15 cm (manufactured by Covidien, USA) was used for the part that was adhered to the abdominal wall, which is a polyene type, and the wall phasing the bowel with Vicryl mesh. The suture passer was then fixed to the abdominal wall. Subsequently, an absorbable tack was applied to fix the mesh over the posterior abdominal wall.
In the open procedure, transverse or longitudinal incisions were performed directly over the hernia site; after releasing the sac open, the sca released the content, excised the sac, and both margins were free from the fatty layer for direct tissue repair using a nylon loop suture single layer; then, a polypropylene mesh was used to cover the defect site onlay mesh and then fixed by nylon 2/0 suture. Depending on the size of the defect, the mesh was cut to cover the margin of the defect, the refractive drain, and the wound closed in layer.
Statistical Analysis
The statistical analysis was performed using SPSS version 28. The mean values and SD to describe the ordinal data, whereas frequency, and percentage to describe nominal data. Chi-square used to compared between groups of the study. p-value <0.05 was consider significant difference.
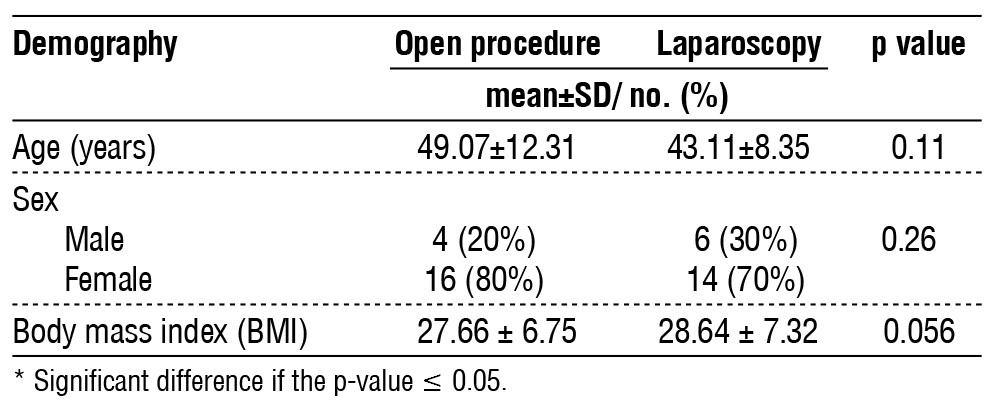
Table 1 - Demographic distribution of patients
Results
The demographic data presented in the form of average age and standard deviation in table 1 shows that the age distribution of patients undergoing open procedure was 49.07±12.31 years, and for those who received laparoscopy was 43.11±8.35 years, and there was no significant difference in patient’s age (p=0.11). Regarding sex distribution, it was the open procedure group 20% was males and 30% males in the laparoscopy group, while females constituted the largest majority of the group, with 80% in the open group and 70% in the laparoscopy group. The gender distribution was also not statistically different (chi-square = 3.163; p=0.26). Besides, the mean BMI was 27.66±6.75 for the open procedure group and 28.64±7.32 for the laparoscopy group; p=.05693, thus having no statistical difference. Altogether, there were no differences in the studied parameters, such as age, sex, and BMI between the open procedure and laparoscopy groups (all p>0.05).
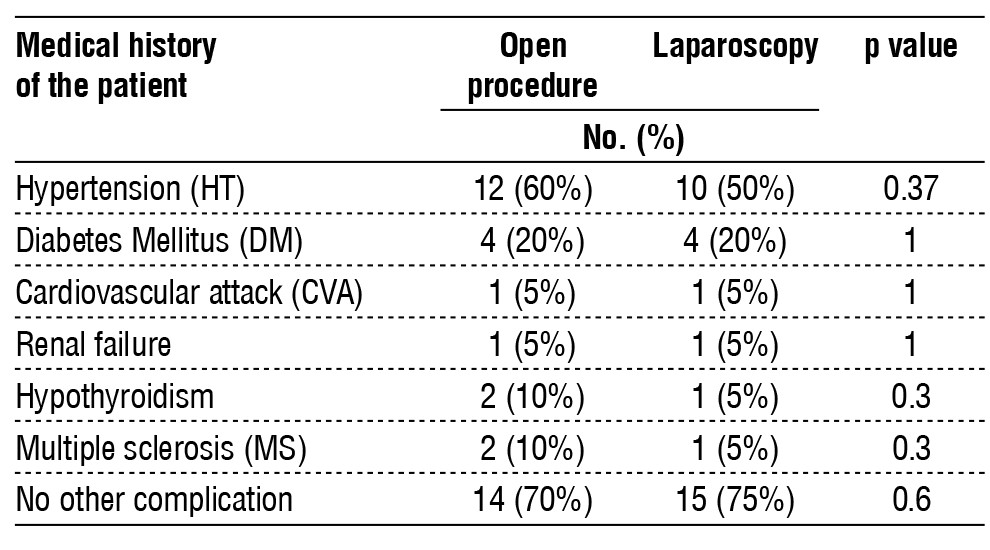
The patients’ medical history of umbilical hernia is shown in table 2, which compares patients who underwent the open technique with those who underwent laparoscopic repair. patients with hypertension was 60 % in the open procedure group and 50 % in the laparoscopy group. No statistically significant differences were observed (p=0.37). Both the groups had the same percentage matched percentage of patients with Diabetes Mellitus (DM) 20% (p=1). Similarly, there were no differences between the two groups regarding cardiovascular attacks (CVA) with p≥1.00), renal failure (p=0.09), or hypothyroidism (p= 0.3). Ten percent of the open procedure group and 5% of the laparoscopic group had multiple sclerosis (MS), again showing no statistically significant difference (p=0.3). Moreover, most patients in the open procedure group had 0% complications, while only 25% in the laparoscopy group had 0% complications with p=0.6055) compared to the two groups of all recorded medical conditions in complications.
Table 2 - the medical history of para-umbilical hernia patients
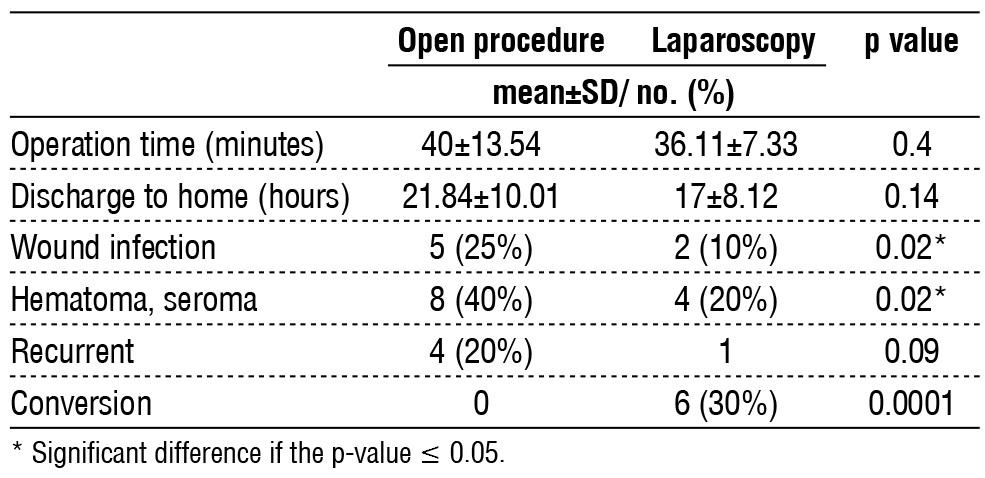
By analyzing the perioperative characteristics of the open and laparoscopic procedures, it was possible to distinguish several differences in the results. The overall operative time appeared to be somewhat longer in open procedures (40±13.54 min) than in laparoscopic procedures (36.11±7.33 min), but the difference was not statistically significant (p=0.4). Discharge times were also similar: open procedures required a mean of 21.84 ± 10.01 h compared with 17±8.12 h for laparoscopy (p=0.14). However, the wound infection rates were higher in the open procedure group. The same observation was seen with hematoma or seroma, with a higher incidence in the open procedure at 40%) than in the laparoscopy at 20%) (p=0.02). The recurrence rates nearly reached a significant level: 20% for open procedures and 10% for laparoscopic procedures (p=0.09), the conversion rates were 30% for laparoscopic procedures (p=0.32). These findings indicate that RC may have benefited from laparoscopic approaches in terms of reduced infection incidence and lower hematoma/seroma rates than open techniques.
Table 3 - Perioperative characteristics
Discussion
Based on our findings, it can be concluded that the open procedure is associated with greater postoperative pain. This is mainly because bilateral extension of the fascial defect must be performed to achieve a vest-over-pant double-breast fascia flap. Abdominal wall tension increases pain following surgery and compromises early ambulation, thus prolonging hospital admissions. However, this technique had the highest recurrence rate in our study, in which all recurrences were reported in patients who underwent day-case suture herniorrhaphy with a short incision.
As for the results of demographic comparisons, no differences were found in participants’ age, distribution by sex, and BMI between the experimental and control groups. The open procedure group comprised 49.07±12.31 years of mean age, while the laparoscopy procedure group comprised 43.11±8.35 years of mean age. This is consistent with the results of a study conducted by Patterson et al. (17) There was no apparent age difference in the surgical outcomes between the open and laparoscopic approaches to hernia repair. The sex distribution was similar in both groups, with slightly more females than males, suggesting that hernias are more common in female patients (5). In addition, the BMI comparison was not significant (p = 0.05693), which is consistent with the results of the meta-analysis by Liu et al. (18), indicating that BMI does not constitute a significant factor in the choice of surgical modality.
When comparing patients’ medical histories for comorbidities, no statistically significant differences were identified with respect to hypertension (p = 0.37) or diabetes mellitus (p = 1). These findings reaffirm the data obtained by Sun et al.(19), who did not identify the presence of comorbidities as a factor influencing the differences between laparoscopic and open procedures. The complication rates also showed that most patients in the open procedure had no complications, while 25% in the laparoscopic group had no complications (p > 0.05). This is particularly relevant in the literature; Shi Z et al. (20) reported that the global overall complication rate was significantly lower for laparoscopic procedures, indicating the possible benefits of laparoscopic approaches.
Concerning perioperative characteristics, an increase in operative time for open procedures was also observed in the present study, which aligns with similar investigations, such as that conducted by Haladu et al.(21). The reason for such differences suggested by the authors may be that laparoscopic surgeries are characterized by shorter operative times because there is less tissue manipulation.
However, in this study, the mesh was fixed to the umbilicus to decrease the space between the mesh and skin, which led to a decrease in hematoma and seroma formation(22).
Open procedures took 21.84±10.01 h for discharge compared to laparoscopic procedures, which were 17±8.12 h; however, this difference was not statistically significant (p=0.14). This aligns with a systematic review by Buia et al. (22) that revealed that patients who underwent laparoscopic operations were more likely to record earlier recovery and shorter hospital discharge.
In the complication analysis, wound infection increased, with 25% in the open procedure group compared to 10% in the laparoscopic group, p=0.02); hematoma/seroma also trended higher in the open group (40% vs. 20%, p= 0.02). These outcomes are consistent with those of the study by Caroff et al. (23) reported that open surgical methods are associated with considerably higher infection risks when given a higher tissue insult. The recurrence rates were nearly statistically significant (20% in open compared to 10% in laparoscopic, p=0.09) and comparable to the results of Yang and Deng et al. (24) reported lower recurrence rates after laparoscopic surgery.
The incidence of wound infection is higher in open surgery than in laparoscopic procedures because of the increase in wound size (20).
Conclusions
Both procedures are effective in treating para-umbilical hernias despite a decrease in the infection rate and hematoma serum malformation in laparoscopic procedures compared to the open procedure. Furthermore, most patients with para-umbilical hernia treated with hematoma and seroma are treated with aspiration. The current study and review results support the general premise that laparoscopic surgery may be superior to open surgery in minimizing complications and enhancing recovery, making it the best option for para-umbilical hernia repair. Predictive models must be further investigated to increase their reliability and update the surgical recommendations.
Acknowledgement
Sincre thanks to the surgical team of Al-Yarmouk Teaching Hospital and Al Arabi Privet Hospital.
Conflict of Interest
The authors has no conflict of interest.
Source of Funding: self-funding
Ethical Statement
Ethical considerations and agreement were signed from each patient enrolled in this study. The study approved by the scientific committee of surgery department, college of medicine, Mustansiriyah University.
References
1. Mannion J, Hamed MK, Negi R, Johnston A, Bucholc M, Sugrue M. Umbilical hernia repair and recurrence: need for a clinical trial? BMC Surg. 2021;21(1):365. doi: 10.1186/s12893-021-01358-1.
2. Barlow A. Understanding Pediatric Umbilical Hernias. US Pharm. 2022;47(12):17-20.
3. Dipp Ramos R, O’Brien WJ, Gupta K, Itani KMF. Incidence and Risk Factors for Long-Term Mesh Explantation Due to Infection in More than 100,000 Hernia Operation Patients. J Am Coll Surg. 2021;232(6):872-880.e2.
4. Shankar DA, Itani KMF, O’Brien WJ, Sanchez VM. Factors associated with long-term outcomes of umbilical hernia repair. JAMA Surg. 2017 May 1;152(5):461-466.
5. Kulaçoglu H. Current options in umbilical hernia repair in adult patients. Ulus Cerrahi Derg. 2015;31(3):157-61.
6. Shrestha D, Shrestha A, Shrestha B. Open mesh versus suture repair of umbilical hernia: meta-analysis of randomized controlled trials. Int J Surg. 2019;62:62-66.
7. Madsen LJ, Oma E, Jorgensen LN, Jensen KK. Mesh versus suture in elective repair of umbilical hernia: systematic review and meta-analysis. BJS Open. 2020;4(3):369-379.
8. Melkemichel M, Bringman S, Granåsen G, Widhe B. SUMMER Trial: mesh versus suture repair in small umbilical hernias in adults - a study protocol for a prospective randomized double-blind multicenter clinical trial. Trials. 2021;22(1):411.
9. Ohba G, Yamamoto H, Minato M, Nakayama M, Honda S, Taketomi A. Transumbilical Repair for Umbilical Hernia: A New Technique. Am Surg. 2023 ;89(6):2865-2867.
10. Bowley DMG, Kingsnorth AN. Umbilical hernia, Mayo or mesh? In: Hernia. 2000.
11. Kubat M, Æengül S. Comparison of Suture Repair and Mesh Repair in Repair of Small Umbilical Hernias: Retrospective Cohort Study. Forbes J Med 2023;4(1):62-7
12. Elhage SA, Pflederer CT, Ayuso SA, Shao JM, Deerenberg EB, Ku D, et al. Multicenter analysis of laparoscopic versus open umbilical hernia repair with mesh: outcomes and quality of life (QoL). Surg Endosc. 2022;36(9):6822-6831.
13. Wang T, Tang R, Meng X, Zhang Y, Huang L, Zhang A, et al. Comparative review of outcomes: single-incision laparoscopic total extra-peritoneal sub-lay (SIL-TES) mesh repair versus laparoscopic intraperitoneal onlay mesh (IPOM) repair for ventral hernia. Updates Surg. 2022;74(3):1117-1127.
14. Giuffrida M, Rossini M, Pagliai L, Del Rio P, Cozzani F. Laparoscopic Intraperitoneal Onlay Mesh (IPOM): Short- and Long-Term Results in a Single Center. Surgeries. 2023;4(1):98-107.
15. Korukonda S, Amaranathan A, Ramakrishnaiah VPN. Laparoscopic versus open repair of para-umbilical hernia - a prospective comparative study of short term outcomes. J Clin Diagn Res. 2017; 11(8):PC22-PC24.
16. Patil M, Gharde P, Reddy K, Nayak K. Comparative Analysis of Laparoscopic Versus Open Procedures in Specific General Surgical Interventions. Cureus. 2024;16(2):e54433.
17. Patterson TJ, Beck J, Currie PJ, Spence RAJ, Spence G. Meta-analysis of patient-reported outcomes after laparoscopic versus open inguinal hernia repair. Br J Surg. 2019;106(7):824-836.
18. Liu J, Li G, Chen Z, Jiang H. A meta-analysis of the effect of different body mass index on surgical wound infection after colo-rectal surgery. Int Wound J. 2023;20(6):2151-2158.
19. Sun V, Burhenn PS, Lai L, Hurria A. The Impact of Comorbidity on Surgical Outcomes in Older Adults with Cancer. Semin Oncol Nurs. 2017;33(1):80-86.
20. Shi Z. Laparoscopic vs. open surgery: a comparative analysis of wound infection rates and recovery outcomes. Int Wound J. 2024; 21(3):e14474.
21. Haladu N, Alabi A, Brazzelli M, Imamura M, Ahmed I, Ramsay G, et al. Open versus laparoscopic repair of inguinal hernia: an overview of systematic reviews of randomised controlled trials. Surg Endosc. 2022;36(7):4685-4700.
22. Bittner R, Bain K, Bansal VK, Berrevoet F, Bingener-Casey J, Chen D, et al. Update of Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias (International Endohernia Society (IEHS)) - Part A. Surg Endosc. 2019;33(10):3069-3139.
23. Caroff DA, Chan C, Kleinman K, Calderwood MS, Wolf R, Wick EC, et al. Association of Open Approach vs Laparoscopic Approach With Risk of Surgical Site Infection After Colon Surgery. JAMA Netw Open. 2019;2(10):e1913570.
24. Yang C, Deng S. Laparoscopic versus open mesh repair for the treatment of recurrent inguinal hernia: A systematic review and meta-analysis. Ann Palliat Med. 2020;9(3):1164-1173.
Full Text Sources:
Abstract:
Views: 7736

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.