Surgery, Gastroenterology and Oncology

|
|
Background: Inguinal hernias continue to be a significant surgical issue due to their prevalence. Males are estimated to have a lifetime risk of 27% inguinal hernia, while females have a lifetime risk of 3%. Our objective was to assesss the surgical outcomes of the combined modified Guarnieri Desarda technique and the Lichnichtien tension-free mesh hernioplasty for inguinal hernia.
Methods: This comparative prospective randomized clinical trial was carried out on forty adult male patients who presented with inguinal hernia at General Surgery Department at Kasr Al Ainy Hospital in Cairo, Egypt. Two equal groups were randomly assigned to patients: the conventional Liechtenstein mesh-based repair (L group) and the combined tissue-based repair (C group). All patients underwent clinical examination, abdomino-pelvic ultrasound, testicular duplex & ultrasound.
Results: NRS after 2 weeks and after 1 month was significantly lower at the technique of Combined modified C Group in relation to L group (p=0.005, 0.001), both groups after 3 months showed no significant difference. C Group showed a significantly lower mid- intercourse pain than the L Group (p=0.044).
Conclusions: Most of the postoperative morbidity is related to recurrence, and the time required to resume daily activities, the technique of Modified Combined (Guarnieri and Desarda) was found to be comparable to Lichtenstein's mesh repair. Moreover, no significant statistical difference was found in the two groups regarding developing varicocele as a postoperative duplex finding. The combine technique showed less postoperative pain, higher satisfaction rate, and not complicated with postoperative foreign body sensation compared to Lichtenstein's mesh repair.
INTRODUCTION
Inguinal hernias continue to be a significant surgical issue due to their prevalence. Males are estimated to have a lifetime risk of 27% inguinal hernia, while females have a lifetime risk of 3%. Inguinal hernia patients experience an annual mortality rate of 100 to 300 per 100,000 (1). Dr. Irving Lichtenstein introduced the technique of Lichtenstein tension-free in 1984 with the objective of eradicating the suture tension adverse effects that had been noticed in previous techniques. The development of this technique is contingent upon an understanding of the metabolic etiology of IH, which includes the ratio of type 1/type 3 collagen and the dysfunction of collagen metabolism (2). The Lichtenstein technique involves the implantation of a polypropylene mesh between the aponeurosis of the external oblique muscle (EOM) and the floor of the inguinal region. The purpose of this mesh is to eliminate the necessity for tension sutures and the utilization of compromised tissues to repair IH. The EOM contraction effectively utilizes the intra-abdominal pressure for repair by exerting counterpressure on the mesh, which is propelled by the increased intra-abdominal pressure during exertion (3). This technique surgical outcomes have been exceedingly promising, with less than 1% recurrence rate (4).
In contrast, it is not without its own constraints, including chronic pain, cord fibrosis, wound infection, and sensation of foreign body. The inguinal hernia correction technique developed by Desarda is a new approach that is distinguished by its feasibility, low recurrence rate, and low cost. Desarda (5) indicated that Lichtenstein's "notension" principle is achieved through this repair procedure. The posterior wall of the inguinal canal is not subjected to tension, even though the strip is transferred from the anterior to the posterior wall. A novel and intriguing concept is the undetached, movable aponeurotic strip that "physiologically" enforces the posterior wall of the inguinal canal (6).
In December 1988, Antonio Guarnieri developed the technique of Guarnieri for inguinal hernia repair. This technique fundamental principle was to alter the inguinal canal anatomy that causes the hernia without altering the physiology (7). The expert surgeon should strive to conduct this operation without mesh, while still respecting the physiology of the inguinal canal. The technique can be performed with or without mesh. The objective of this technique is to repair pure tissue. Even in the absence of mesh, this technique can be regarded as "tension-free" and can be employed in any circumstance without the need for patient selection (8).
We hypothesized that modified Desarda with Guarnieri provided effective and safe new technique in inguinal hernia treatment.
The purpose of our research was to assess the surgical outcomes of the Lichnichtien tension- free mesh inguinal hernia hernioplasty and the combined modified Guarnieri Desarda technique in terms of postoperative complications and pain (seroma, hematoma, wound infection), chronic inguinodenia, early recurrence, and testing of testicular vascularity and size using a testicular duplex and ultrasound.
PATIENTS AND METHODS
This comparative prospective randomized clinical trial carried out at the Department of General Surgery at Kasr Al Ainy Hospital in Cairo, Egypt, from February 2022 to October 2023, on 40 adult male patients who presented with inguinal hernia.
Kasr Al Ainy Hospital ethics committee in Cairo, Egypt, granted its approval (Approval code: MD-255-2022). All patients agreed to provide written informed consent. This investigation adhered to the 1964 Helsinki declaration and later amendments.
Inclusion and Exclusion Criteria
Inclusion criteria were adult male patients, with age above 18 years old and with non- complicated inguinal hernia.
Exclusion criteria involved patients under the age of 18 and all complicated hernias (obstructed, inflamed, or strangulated), recurrent inguinal hernia, patient with weak, thin, weak external oblique aponeurosis (intraoperative findings), prior surgery at inguinal region and refusal of the patients to participate in the study.
Randomization
The sealed opaque envelope technique was employed to allocate participants to the treatment group, and randomization was conducted in accordance with computer-generated random number tables. According to randomization, patients were split into two groups each comprising 20 patients:
• Combined tissue-based repair (C group);
• Conventional Liechtenstein mesh-based repair
(L group).
Preoperative Assessment
The preoperative evaluation of all patients who met the inclusion criteria of the study involved a clinical examination, history recording, and basic laboratory investigations, such as random blood sugar, complete blood picture, kidney, and liver function tests, INR, abdomino-pelvic ultrasound to detect organomegaly if present, testicular duplex & ultrasound to document testicular vascularity and to be repeated after 3 months from surgery. Further investigations were carried out on elderly patients (over the age of 60) as part of the preanesthetic workup, such as echocardiography.
OPERATIVE TECHNIQUE
Anesthesia was according to the opinion of anaesthetist after detailed evaluation of preanesthetic. The same surgeon performed all operations, and the operative time was estimated from skin incision to skin closure.
Combined modified (Guarnieri and Desarda) technique (C Group)
A transverse inguinal skin incision is performed, followed by the fascia of camper and the fascia of Scarpa opening. The external oblique's fiber axis was used to incise the aponeurosis. The inguinal canal was accessed in order to identify and retract the ilioinguinal nerve. After that, the cord was dissected and secured with adhesive. Although the strip is transferred from the anterior to the posterior wall of the inguinal canal, the posterior wall is not subjected to tension. The undetached, movable aponeurotic strip that "physiologically" enforces the posterior wall of the inguinal canal is a novel and intriguing concept. The internal spermatic fascia and cremaster's proximal tract are separated, and the spermatic cord's components (vessels and vas difference) are subsequently isolated. Then we performed a modified Guarnieri technique as follows; after retraction of the fleshy part of conjoint tendon, starting on the deep ring and moving medially and cranially, an incision of 2-cm was performed on the transversalis fascia and transversus aponeurosis. After bringing the spermatic cord's components to the incision's medial angle, Prolene 2/0 was utilized to begin the suture first layer. The thread formed a fresh, readily calibrated deep ring on its first passage. After that, the incision was sutured shut, sealing the original ring, the cremaster and internal spermatic fascia of the first layer were covered by a second layer that was made in the opposite direction using the same suture. Now the new internal ring was located deep to the fleshy medial fibres of conjoint tendon to augment the inguinal canal shutter mechanism, also the spermatic cord contents medialization acted in a valve manner which guard against recurrence. Here we didn't proceed to the rest of the Guarnieri technique as it is much sophisticated, and we replaced it by Desarda technique to reinforce the posterior wall (fig. 1).
Figure 1 - (I) Guarnieri portion of the repair of left side inguinal hernia. A: Obliterated old internal ring.
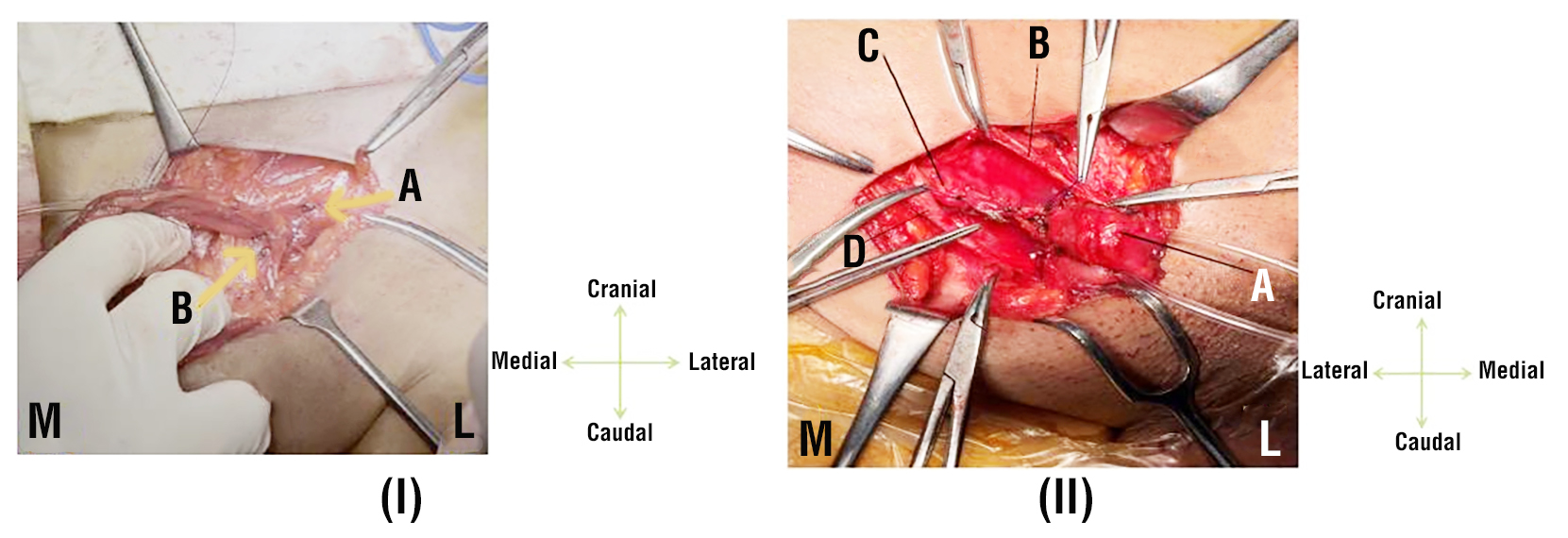
B: Spermatic cord emerging from the new internal ring. (M= Medial.
L= Lateral), (II) “Guarnieri portion of the repair of right-side inguinal hernia” A: Spermatic cord emerging from the new internal ring. B: Upper leaflet of EOA. C: Obliterated old internal ring. D: Lower leaflet of EOA.
Modified Desarda Technique
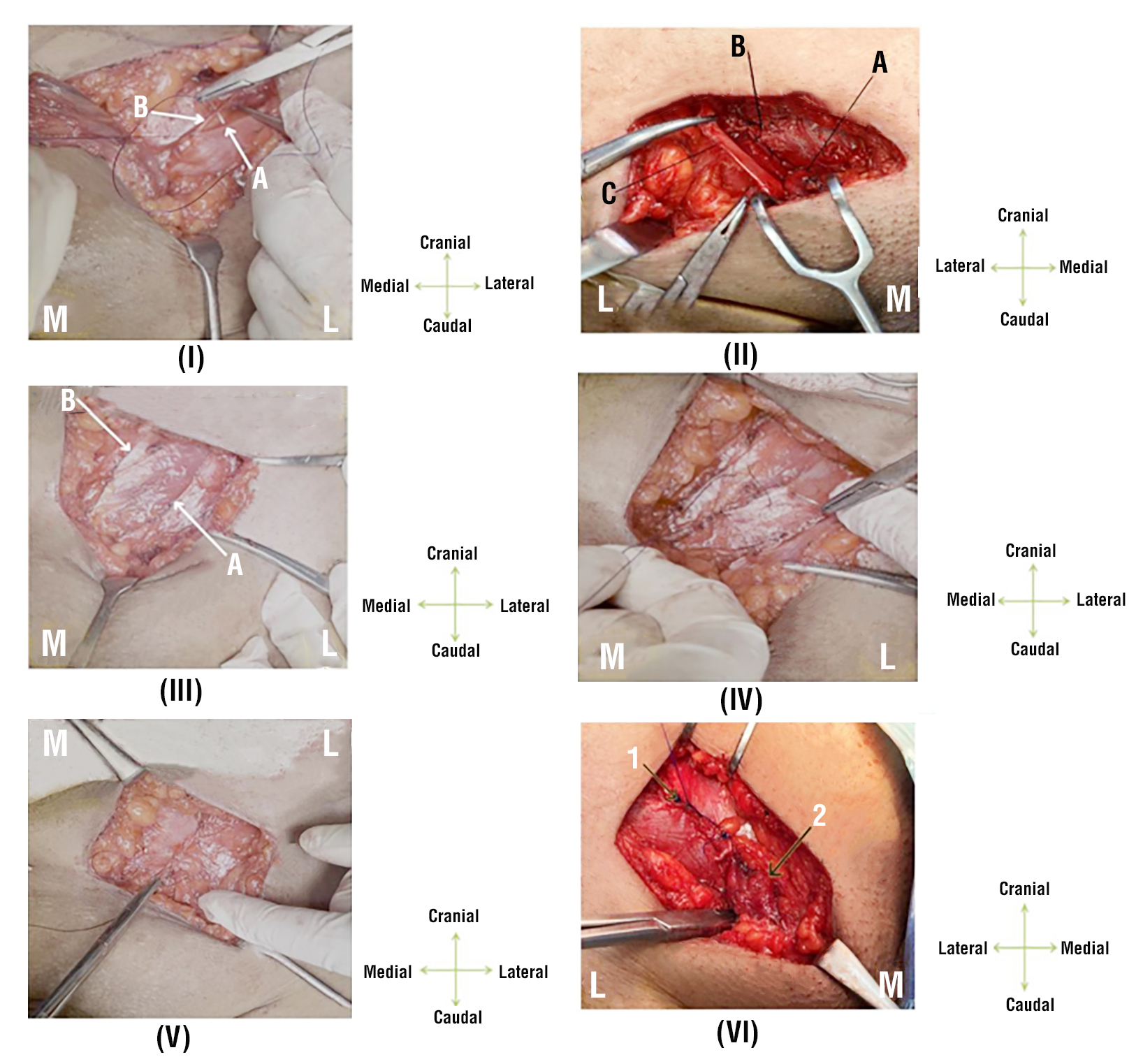
Suturing the lower border of upper leaflet of EOA to the inguinal ligament's reflection (iliopubic tract) starting from lacunar ligament till a point lateral to the occluded internal ring utilizing proline 2/0 running suture. A fragment of EOA was left in the inguinal canal floor, 2 cm above the previous sutured line, following an incision in the EOA. The last stage involved sewing the EOA's lower leaf upper border to the lower border of its higher leaf. Interrupted absorbable sutures were utilized to close the scarpa’s fascia. Finally, the skin was sealed. The operative duration was documented from the commencement of the skin incision to the closure. On the initial postoperative day, patients were discharged, and subsequent appointments were scheduled for two weeks, one month, three months, and six months to evaluate early and late pain scores, complications, return to full activity, and recurrence (fig. 2).
Figure 2 - (I) Desarda Repair of left side inguinal hernia (First Step + EOA sutured to iliopubic tract). A: Iliopubic tract. B: Upper leaflet of EOA. (II) Desarda Repair of right-side inguinal hernia (First Step). A: Medialized spermatic cord. B: EOA sutured to iliopubic tract. C: Lower leaflet of EOA, (III) Utilizing continuous proline 2/0 suture, the top border of the EOA slit was sutured cautiously to the aponeurotic portion of the conjoint tendon avoiding making any tension. Now, we calibrated the newly formed internal ring to admit the little finger's tip and ensure that the contents of the spermatic cord are not compressed by the new internal ring. (III) " Desarda Repair (Third step), tendinous part of conjoint tendon sutured to lower leaflet of splitting incision" in left side hernia repair. (V) Desarda Repair Last Step" of left side inguinal hernia ( Upper leaflet of splitting incision at EOA sutured to lower leaflet of EOA). (VI) " Last step of Desarda Repair of right inguinal hernia". 1. Upper leaflet of splitting incision at EOA sutured to lower leaflet of EOA. 2. Spermatic cord.
Lichtenstein Tension-Free Repair (L group)
Through the use of a prosthetic mesh to reinforce the inguinal floor, the Lichtenstein technique reduces tension during the repair, thereby expanding the inguinal canal's domain. Accordingly, Cord structures are initially exposed and mobilized in a manner that is consistent with other open approaches. And hernio-tomy is done. The pubic tubercle, the inguinal ligament shelving margin, and an adequate area for mesh were exposed by dissecting the inguinal canal. The mesh, which was a 6 × 11 cm rectangle with a tapered medial edge, was 2 to 3 centimeters in size and extended above the triangle of Hesselbach. The superior tail occupied two-thirds of the mesh's width, while the inferior tail occupied the remaining one-third. The lateral portion of the mesh was divided into two halves. The inferior margin of the mesh was secured using a synthetic monofilament suture that was permanent. From the medial to lateral shelving border of the inguinal ligament, the fixation was extended until it reached the internal ring. The medial edge of the mesh was affixed to the rectus sheath, and the upper tail was secured to the internal oblique aponeurosis using a synthetic, absorbable suture (9) (fig. 3).
Figure 3 - Lichtenstein tension-free hernioplasty
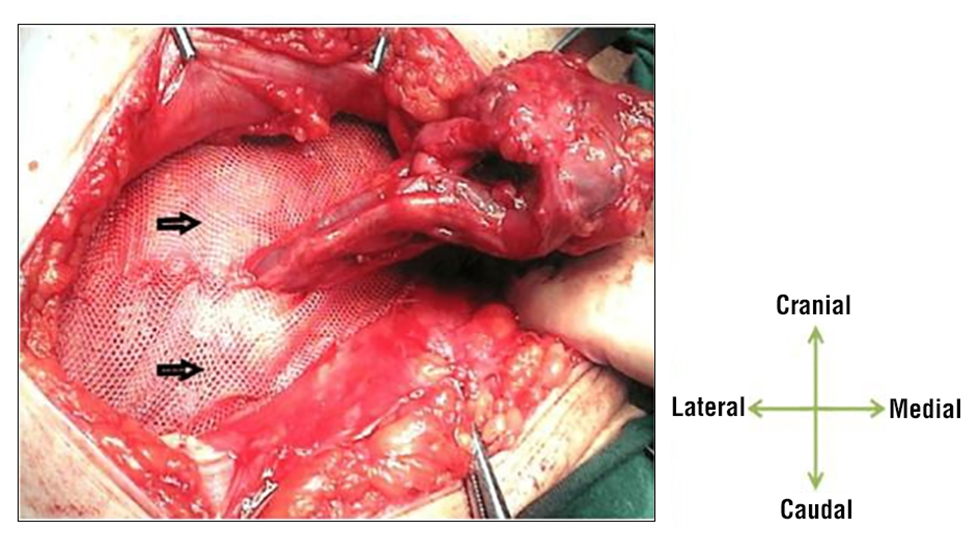
The mesh's lateral ends were designed to tightly encircle the cord at the internal ring, but not so tightly that they would cause it to be strangled. The tails were subsequently attached to the inguinal ligament using an interrupted thread, below the external oblique aponeurosis.
Postoperative Assessment
The postoperative management of all patients was consistent, with the routine administration of a single dose of Diclofenac injection. Then, diclofenac tablets were administered twice daily for a period of three days. The patients then were discharged and come back for follow up multiple times as follows: after 2 weeks to assess post-operative pain, the infection of surgical site, seroma formation, hematoma formation and cord Induration, after 1 month to assess pain at inguinal region and foreign body sensation, also, after 3 months patients perform testicular duplex and ultrasound to assess testicular size, testicular vascularity, presence of secondary hydrocele, and pain at inguinal region and then after 6 months to assess early hernia recurrence and chronic inguinodynia. Further follow up was done for patients who completed 1 year after surgery to detect delayed recurrence.
Postoperative pain was assessed using an 11-point numerical rating scale (NRS 11), with 0 denoting no pain and 10 representing the most severe pain imaginable (10). Additionally, chronic inguinodynia was evaluated. At 24 hours postoperatively, patient satisfaction was assessed using a five-point Likert scale, with one indicating extreme dissatisfaction and five indicating extreme satisfaction (11).
The primary outcome was the feasibility of the technique, while the secondary outcome was the recurrence.
Statistical Analysis
The statistical analysis was carried out using SPSS v27, which is produced by IBM*, Armonk, NY, USA. To determine if the data distribution was normal, we used histograms and the Shapiro-Wilk test. The mean and standard deviation (SD) were calculated from the quantitative parametric data, which had been analyzed using an unpaired student t-test. We used the Mann- Whitney U test to look at non-parametric quantitative data that was summarized by the median and IQR. Qualitative variables were reported as frequency or percentage (%) as applicable, and data was analyzed using either Fisher's exact test or a Chi-square test. To determine statistical significance, two-tailed p values were set at less than 0.05.
RESULTS
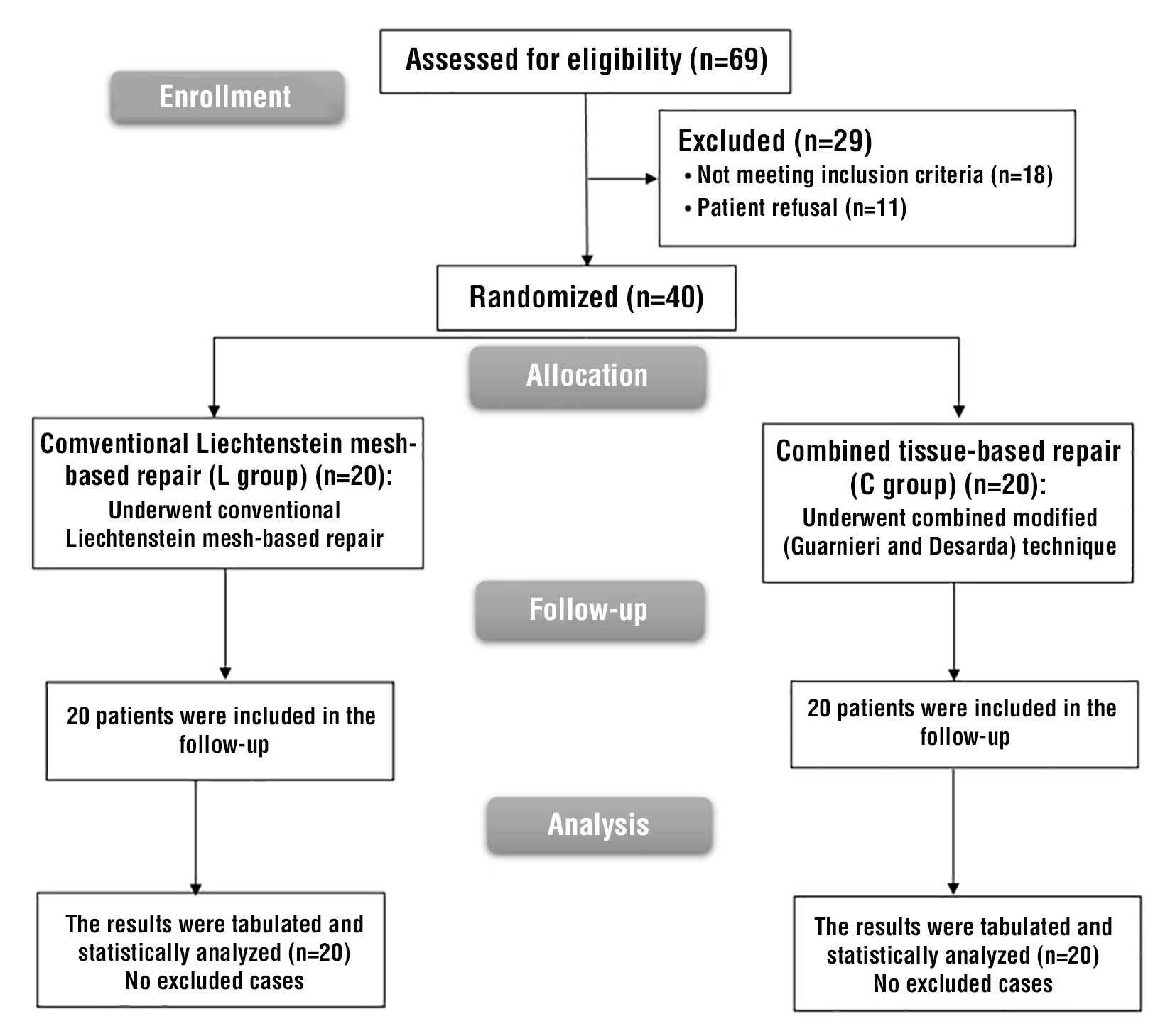
69 patients were evaluated for eligibility in this investigation; the criteria were not met by 18 patients, and 11 patients declined to participate. Two groups were randomly allocated to the remaining 40 patients, with 20 patients in each. The statistical analysis and follow-up of all allocated patients were conducted (fig. 4).
Figure 4 - CONSORT flowchart of the enrolled patients
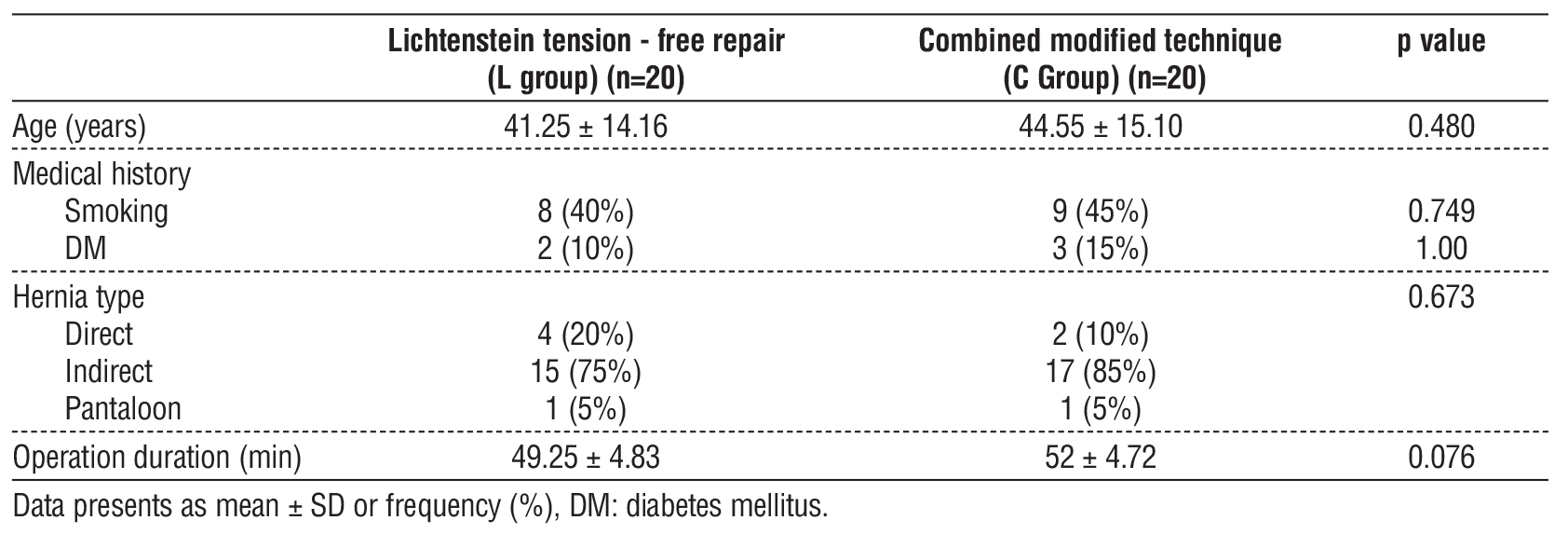
An insignificant difference was found among both groups regarding age, medical history (smoking and DM), hernia type and operation duration (table 1).
Table 1 - Baseline chracterestics of the studied groups
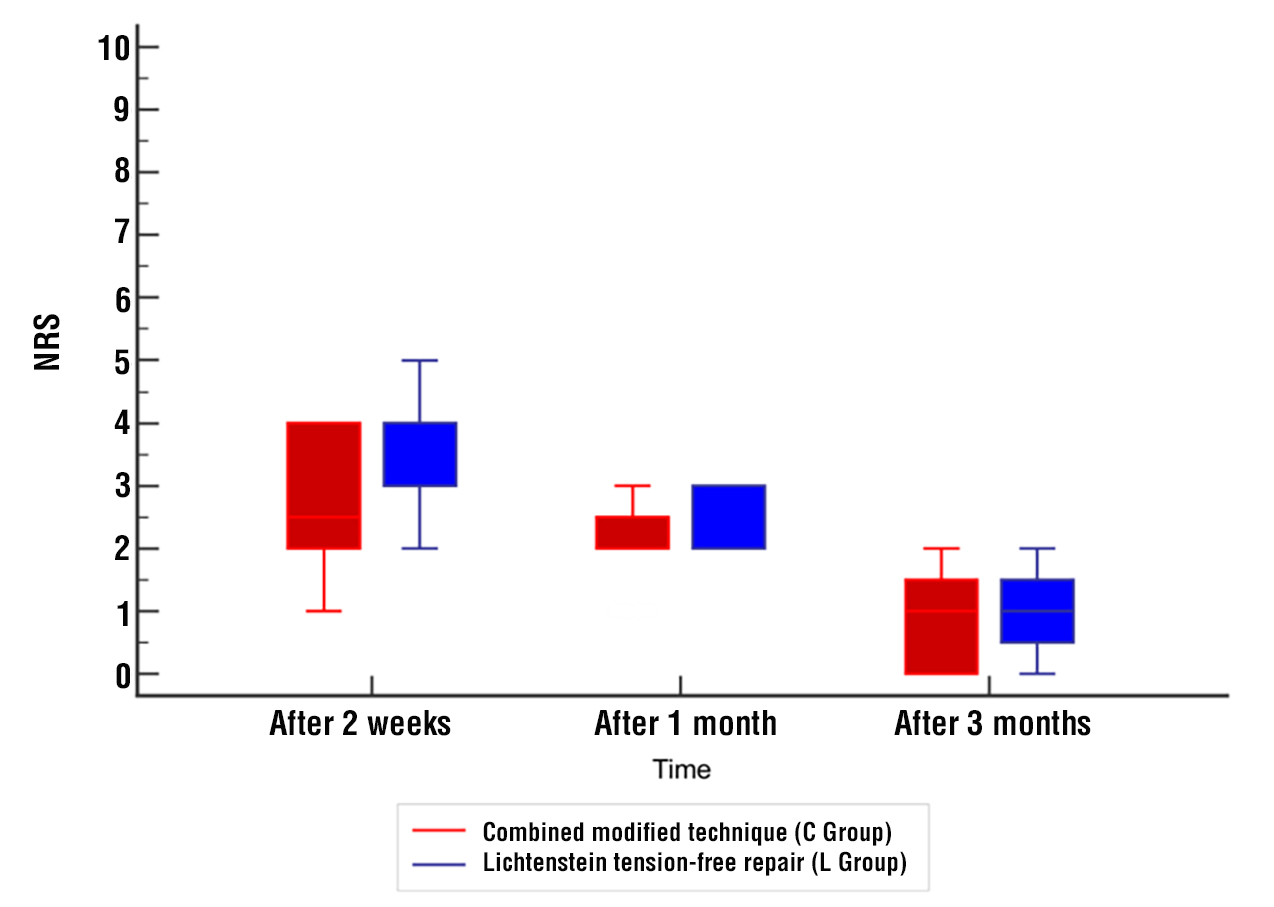
Regarding the postoperative pain, NRS after 2 weeks and after 1 month was significantly lower at Combined modified technique (C Group) compared to Lichtenstein tension-free repair (L group) (p=0.005, 0.001), both groups after 3 months showed no significant difference (fig. 5).
Figure 5 - Postoperative NRS of the studied groups
The duration of the postoperative inpatient hospital stay and the postoperative recovery (return to daily activity and return to work activity) were not significantly different among the two groups. The pain of mid-intercourse was significantly lower in the C Group compared to the L group in terms of the outcome (p=0.044). Nevertheless, no significant difference among the two groups was found in terms of chord induration and chronic inguinodynia (table 2).
Table 2 - Hospital stays duration, postoperative recovery and outcome of the studied groups

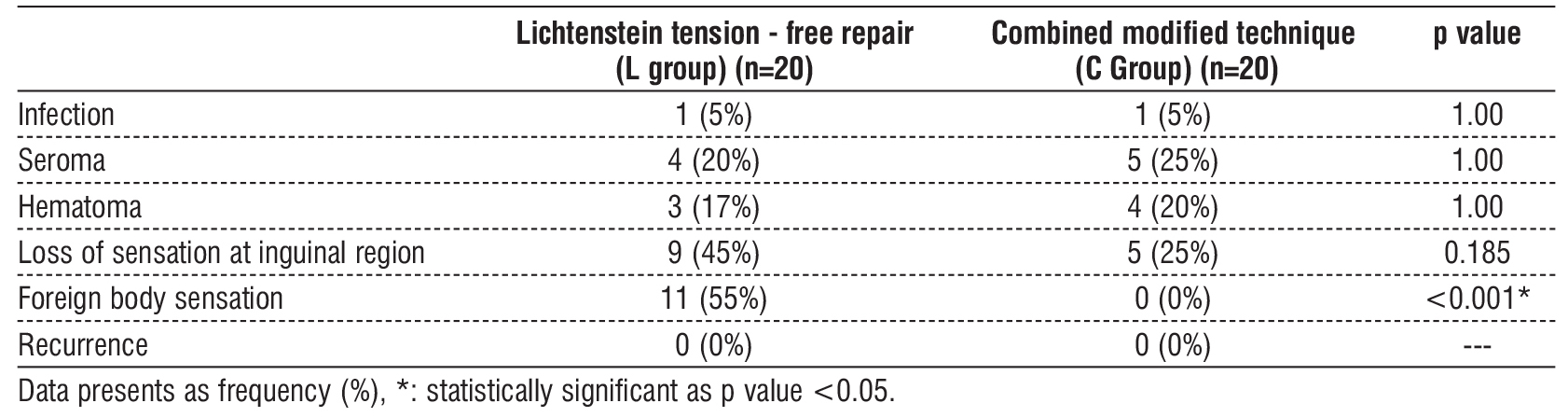
Regarding complications, infection occurred in 1 (5%) patient in Lichtenstein tension-free repair (L group) and 1 (5%) patient in combined modified technique (C Group), seroma occurred in 4 (20%) patients in Lichtenstein tension-free repair (L group) and 5 (25%) patients in combined modified technique (C Group), and hematoma occurred in 3 (17%) patients in Lichtenstein tension-free repair (L group) and 4 (20%) patients in combined modified technique (C Group), 9 (45%) cases in Lichtenstein tension-free repair (L group) complained of hypoesthesia or numbness at the inguinal region, while 5 (25%) cases in combined modified technique (C Group) had the same complain, 11 (55%) cases have complained of sensing a subcutaneous foreign body at inguinal region. Evidently in combined modified technique (C Group). Regarding the recurrence, within six months from the surgery, neither Lichtenstein tension-free repair (L group) nor combined modified technique (C Group) have had any cases with recurrence of inguinal hernia. Recurrence was assessed for cases that have completed one year after surgery, nine cases in Lichtenstein tension-free repair (L group), ten cases in combined modified technique (C Group), and results show that none of them encountered recurrence.
The L group exhibited a significantly higher level of foreign body sensation than the C group (p<0.001) as there wasn’t any complains of foreign body sensation which is due to the fact that this technique is mesh-free. The incidence of infection, seroma and hematoma was insignificantly different among both groups (table 3).
Table 3 - Complications of the studied groups
Testicular Ultrasound and Duplex Findings
Regarding testicular vascularity which was assessed by duplex examination pre-operative and 3 months post-operative, there was no difference in testicular vascularity in any of the cases in both groups. Consequently, there was no post-operative testicular atrophy in both groups.
Varicocele
In Lichtenstein tension-free repair (L group), 7 cases showed varicocele, according to their post-operative duplex study, 4 of which have had the same finding in their pre-operative duplex study, while 3 cases of them developed varicocele as a new duplex finding. On the other hand, in combined modified technique (C Group), 8 cases showed varicocele, according to their post-operative duplex study, 6 of which have had the same finding in their pre-operative duplex study, while 2 cases of them developed varicocele as a new duplex finding. No significant statistical difference was noticed among the two groups regarding developing varicocele as a post-operative duplex finding.
Hydrocele
In Lichtenstein tension-free repair (L group), 10 cases showed mild hydrocele, according to their post-operative scrotal ultrasound, 6 of which have had the same finding in their pre-operative ultrasound, while 4 cases of them developed mild hydrocele as a new sonographic finding. On the other hand, in combined modified technique (C Group), 10 cases showed mild hydrocele, according to their post-operative duplex study, 9 of which have had the same finding in their pre-operative duplex study, while 1 case of them developed mild hydrocele as a new duplex finding, however, 1 case had pre-operative mild hydrocele but their post-operative ultrasound showed no evidence of hydrocele. No significant statistical difference was found among both groups regarding developing hydrocele as a post-operative sonographic finding. No one has developed acute vascular testicular emergency post-operative in both groups.
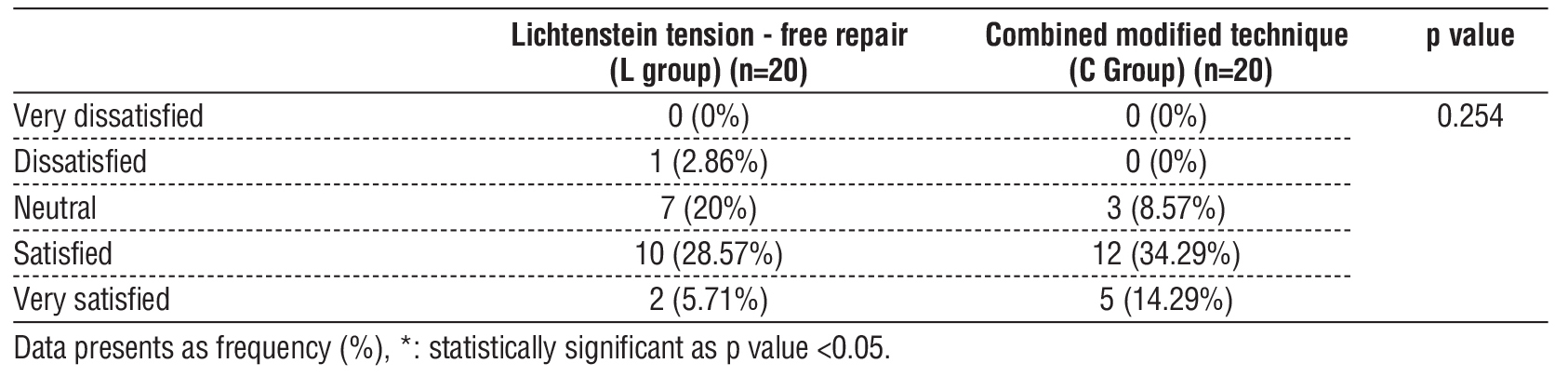
An insignificant difference was observed among both groups regarding satisfaction; however it seems to be higher among patients in Combined modified technique (C Group) (table 4).
Table 4 - Satisfaction of the studied groups
DISCUSSION
The aim of hernia repair surgery is to create a posterior wall that is highly mobile, robust, and physiologically dynamic. The inguinal hernia correction is the most frequently conducted general surgery procedure nowadays (12). A tension-free closure of the hernia defect is essential for the successful surgical repair of inguinal hernias, which can lead to the lowest possible recurrence rate (13). Bassini's repair and its modifications were the standard treatment for inguinal hernias for an extended period before the Lichtenstein tension-free repair was introduced. This resulted in a significant decrease in the scope of tissue-based remedies, such as Bassini's repair and shoulder repair. In a large multi-centre controlled investigation that followed Bassini and McVay restorations, recurrence rates of 8.6% and 11%, respectively, were reported (14).
The Lichtenstein mesh closure technique was founded on the principle of utilizing prosthetic material to cause fibrosis, thereby strengthening the posterior wall of the inguinal canal. The mesh-related complications are detailed, despite the fact that it meets the majority of the criteria for an ideal hernia surgery. Numerous biomaterials (prosthetic materials) have been developed; however, their efficacy in treating inguinal hernia remains uncertain (14,15).
In order to physiologically enforce the posterior wall of the inguinal canal, Dr. Desarda's technique is a tissue-based repair that utilizes an undetached, movable aponeurotic segment of external oblique muscle (16). In this strip, lateral tension is produced by the contraction of the external oblique muscle. On the other hand, the conjoined muscle contracts, creating superior tension by drawing the strip upwards. Because of this, the strip functions as a "shield" to prevent any herniation. The essential component of this operation is the aponeurotic strip, which provides the posterior wall of the inguinal canal with supplementary strength, thereby preventing herniation (17). The force of muscle contractions is used to grade the tension in this strip. The tension in this strip is exacerbated by the more severe abdominal muscle contractions that occur as a consequence of elevated intra-abdominal pressure, such as during coughing. During repose, the strip or suture line is tension-free. Therefore, this procedure establishes a posterior wall that is both physiologically dynamic and robust. One possible explanation for the reduced rate of hernia recurrence observed in this repair is this. Other authors' research has also supported this conclusion, indicating that desarda's repair and Lichtenstein's repair were comparable in terms of their recurrence rates (18).
This is the first study to compare the technique of Modified Combined (Guarnieri and Desarda) and the technique of Lichtenstein in the repair of inguinal hernias, to the best of our knowledge. The addition of Guarnieri to the Desarda reduced the lateral weakness post operative.
We showed that operative time was insignificantly different between both groups.
Operation duration is a variable that is dependent on the surgeon and is indicative of the operation's simplicity. Gedam et al. (19) showed that The Lichtenstein repair required an average of 73 ± 13.63 minutes, while the Desarda repair required an average of 72 ± 13.89 minutes (p=0.508). The results were not statistically significant. The operating duration is equivalent to that of Desarda repair, as the time required to fix the mesh is analogous to the time required to remove and fix the external oblique aponeurosis. Youssef et al. (20), Rodriguez et al. (21) demonstrated statistically significant differences in operative duration, which is in opposition to our results.
Regarding pain, NRS after 2 weeks and after 1 month was significantly lower at C Group in relation to L group (p=0.005, 0.001), both groups after 3 months showed no significant difference between Gaur et al. (22) discovered that the pain intensity of the Lichtenstein and Desarda groups did not differ significantly at six hours, twenty-four hours, seven days, one month, and three months following the operation. Similar findings were demonstrated by Manyilirah et al. (23), Emile et al. (24) and Youssef et al. (20). However, Desarda group had less pain in a study showed by Gedam et al. (19). This study rejected the hypothesis that pain scores would be increased following the repair of Lichtenstein as a result of the extensive dissection necessary to position the mesh. The Desarda group exhibited decreased pain scores; however, The discrepancy was not statistically significant. This disparity in mean pain scores between the two groups was also not clinically significant (22).
Gedam et al. (19) showed that in comparison to the Lichtenstein group, the Desarda group experienced significantly less postoperative pain during the initial seven postoperative days (p=0.09). This observation was not made in any other study, including those conducted by Youssef et al. (20), Abbas et al. (25), and Mitura et al. (26). Many confounding factors, such as nerve traction, tissue handling, and intraoperative manipulation, may be responsible for this. The time required to return to fundamental and domestic activities was statistically significantly reduced by the Desarda technique (p=0.001 and (p=0.013), respectively). This implies that patients who underwent the Desarda technique were able to ambulate and resume these activities faster than those who underwent the Lichtenstein repair. Reduced tissue manipulation, fewer dissections, and reduced postoperative pain may facilitate the rapid return to domestic activities in the technique of Desarda. Youssef et al. (20), Abbas et al. (25), and Mitura et al. (26) and Desarda et al. (5) reported similar results.
Regarding complication, foreign body sensation was significantly greater in the L group in relation to C Group (p<0.001) as there wasn’t any complains of foreign body sensation which is due to the fact that this technique is mesh-free. The incidence of infection, seroma and hematoma was insignificantly different between both groups.
In a study by Szopinski et al. (27), In total, 208 male patients were randomly assigned to either the technique of Desarda or Lichtenstein group (105 and 103, respectively). Recurrence and chronic pain were the primary consequences that were assessed. There were two recurrences in each cohort during the follow-up (p=1.000). The rates of chronic pain reported by patients in groups D and L were 4.8% and 2.9%, respectively (p=0.464). The groups did not exhibit any differences in the rate of return to activity or a foreign body sensation. In the D group, seroma production was significantly reduced (p=0.004).
Nevertheless, Rodriguez et al. (28), conducted a comprehensive analysis that included 2,225 patients and identified 4 recurrence cases in the group of Desarda. They believed that the failure to properly lateralize the tendon and the internal ring insufficient constriction, as recommended by Desarda, were the causes. Desarda (5), reported that the clinical trial conducted at a small district hospital in India did not result in the recurrence of his technique, while the Lichtenstein repair did. The mesh group experienced 1.9% recurrences, while this technique did not. Szopinski et al. (27) exhibited a recurrence rate of 1.9% in Lichtenstein and 1.94% in the group of Desarda. Similar p values were acquired in the investigations carried out by Youssef et al. (20), Abbas et al. (25), and Mitura et al. (26)
Moghe et al. (17) in their study demonstrated that there was no statistically significant difference in the incidence of wound infections between patients who underwent inguinal hernia repair using Desarda's technique and those who underwent the procedure using Lichtenstein's technique. Furthermore, the two techniques required comparable durations of time to resume daily activities. Szopinski et al. (27), conducted a randomized controlled trial that revealed no statistically significant difference in clinical outcomes between Desarda's and Lichtenstein's techniques at the three-year follow-up of adult male patients who underwent primary inguinal hernia surgery. The two groups had comparable complication rates, with the exception of seroma development. Patients who underwent the author's technique experienced a shorter hospital stay, a shorter time to return to work, and fewer complications in comparison to mesh- based restorations, according to a study conducted by Dr. Desarda (29) A case-control investigation was also conducted by Manyilirah et al. (23) to compare Desarda's repair with Lichenstein's repair. Additionally, the findings suggested that the rates of wound infections in both repairs were comparable.
Moghe et al. (17) discovered that the investigation did not involve any patients who developed wound infections of grade 2 or higher. On the first postoperative day, grade 1 wound infections were observed in a total of 10 patients (40%) in group 1 and nine patients (36%) in group-2. The number of patients in group 1 and group 2 who developed grade 1 wound infections was eight and seven, respectively, on POD 10. However, the groups did not exhibit a statistically significant difference (p>0.05). Szopinski et al. (27) reported only one case was found in D group while two cases were reported un L group developed post-operative superficial wound infection, thus, no significant statistical difference among “C group” and “L group” was observed regarding post-operative wound infection.
Rodrà et al. (30) stated that seroma was the most prevalent complication in both groups, affecting 18 patients (1.4%).The Lichtenstein group experienced forty-five (7.0%) patients developing postoperative complications, while the group of Desarda experienced twenty-two (3.6%) patients developing complications (p<0.05).
We reported that no significant differences were observed among groups regarding testicular vascularity, testicular atrophy, varicocele, and hydrocele among patients preoperative and after three months follow- up period.
Koksal et al. (31) performed an elective hernio-rrhaphy procedure to treat an inguinal hernia in 32 male patients ranging in age from 33 to 72 years. The participants were part of a prospective randomized research. One group had Lichtenstein hernia repair (n=16) whereas the other group underwent hernia repair that was entirely extraperitoneal-preperitoneal (n=16). The testes Color Doppler ultrasonography was carried out on all patients on the day prior to the operation, 3 days after the procedure, and 6 months following the operation. The results of resistive index of the group of Lichtenstein hernia repair and the group of entirely extraperitoneal- preperitoneal hernia repair were statistically insignificant (p>0.05) in both the periods of preoperative, early, and late postoperative.
Lima Neto et al. (32) carried out a prospective clinical observational study on 39 male patients who had unilateral inguinal hernias of types III A and III B. Doppler ultrasound was employed to evaluate patients before the operation and selectively at the third and sixth months following the procedure. systolic and diastolic ,index of velocity resistance, index of pulsatility, and testicular volume were the variables that were analyzed. There were no statistically significant changes in the resistance index (p=0.998), pulsatility index (p=0.582), systolic velocity (p=0.257), diastolic velocity (p=0.554), and testicular volume (p=0.197) over time.
The study has limitations due to its small sample size and brief follow-up period.
Therefore, a larger sample size with multi-center cooperation and a longer follow-up period are recommended. Both techniques are recommended for patients who have inguinal hernias.
CONCLUSION
Lichtenstein's mesh repair was found to be comparable to the technique of Modified Combined (Guarnieri and Desarda) in terms of recurrence, most of postoperative morbidity, and the duration required to resume daily activities. Moreover, the two groups didn’t differ statistically regarding developing varicocele as a post-operative duplex finding. In comparison to Lichtenstein's mesh repair, the combined technique demonstrated a lower postoperative pain, a higher satisfaction rate, and a lack of complications with postoperative foreign body sensation. To avoid long-term mesh-related morbidity in younger patients with simple indirect hernias, the Desarda and Guarnieri approach could be a good alternative to mesh-based treatments.
Conflict of Interest: Nil
Financial support and sponsorship: Nil
REFERENCES
1. Konschake M, Zwierzina M, Moriggl B, Függer R, Mayer F, Brunner W, et al. The inguinal region revisited: the surgical point of view : An anatomical-surgical mapping and sonographic approach regarding postoperative chronic groin pain following open hernia repair. Hernia. 2020;24:883-94.
2. Hori T, Yasukawa D. Fascinating history of groin hernias: Comprehensive recognition of anatomy, classic considerations for herniorrhaphy, and current controversies in hernioplasty. World J Methodol. 2021;11:160-86.
3. Messias BA, Nicastro RG, Mocchetti ER, Waisberg J, Roll S, Junior M. Lichtenstein technique for inguinal hernia repair: ten recommendations to optimize surgical outcomes. Hernia. 2024;28:1467-76.
4. Cabrera-Vargas LF, Mendoza-Zuchini A, Aparicio BS, Pedraza M, Sajona-Leguia WA, Arias JSR, et al. Postoperative outcomes using Lichtenstein open hernioplasty versus Nyhus preperitoneal hernioplasty in inguinal hernia: A comparative analysis with 1-year follow-up. Health Sci Rep. 2023;6:e1151.
5. Desarda M, Ghosh A. Comparative study of open mesh repair and Desarda’s no-mesh repair in a District Hospital in India. East Central Afr J Surg. 2006;11:28-34.
6. Ahmadinejad I, Jalali A, Ahmadinejad M, Soltanian A, Ahamdinejad Y, Shirzadi A, et al. Inguinal hernia: Lichtenstein VS Shouldice technique repair: A randomized controlled trial. Surg Open Sci. 2024;17:70-4.
7. Guarnieri A, Moscatelli F, Guarnieri F, Ravo B. A new technique for indirect inguinal hernia repair. Am J Surg. 1992;164:70-3.
8. Ramshaw B, Chiu S. Open Non-mesh Inguinal Hernia Repair. In: LaPinska MP, Blatnik JA, editors. Surgical principles in inguinal hernia repair : A comprehensive guide to anatomy and operative techniques. Cham: Springer International Publishing; 2018. p. 33-8.
9. Destek S, Gul VO. Comparison of lichtenstein repair and mesh plug repair methods in the treatment of indirect inguinal hernia. Cureus. 2018;10:29-35.
10. Dang H, Stafseth SK. Documentation for assessing pain in post-operative pain management pre- and post-intervention. J Perianesth Nurs. 2023;38:88-95.
11. Chyung SY, Roberts K, Swanson I, Hankinson A. Evidence-based survey design: The use of a midpoint on the Likert scale. Performance Improvement. 2017;56:15-23.
12. Xu LS, Li Q, Wang Y, Wang JW, Wang S, Wu CW, et al. Current status and progress of laparoscopic inguinal hernia repair: A review. Medicine (Baltimore). 2023;102:e34554.
13. Gudigopuram SVR, Raguthu CC, Gajjela H, Kela I, Kakarala CL, Hassan M, et al. Inguinal hernia mesh repair: The factors to consider when deciding between open versus laparoscopic repair. Cureus. 2021;13:196-8.
14. Patil SM, Gurujala A, Kumar A, Kumar KS, Mithun G. Lichtenstein mesh repair (LMR) v/s Modified Bassini's Repair (MBR) + Lichtenstein mesh repair of direct inguinal hernias in rural population - a comparative study. J Clin Diagn Res. 2016;10:12-5.
15. Rodríguez M, Gómez-Gil V, Pérez-Köhler B, Pascual G, Bellón JM. Polymer hernia repair materials: Adapting to patient needs and surgical techniques. Materials (Basel). 2021;14:23-9.
16. Ndong A, Tendeng JN, Diallo AC, Diao ML, Diop S, Dia DA, et al. Is Desarda technique suitable to emergency inguinal hernia surgery? A systematic review and meta-analysis. Ann Med Surg (Lond). 2020; 60:664-8.
17. Moghe D, Prajapati R, Banker A, Khajanchi M. A comparative study of desarda’s versus lichtenstein’s technique for uncomplicated inguinal hernia repair. Cureus. 2022;14:23-33.
18. Pereira C, Varghese B. Desarda non-mesh technique versus
lichtenstein technique for the treatment of primary inguinal hernias: A systematic review and meta-analysis. Cureus. 2022;14:e31630.
19. Gedam BS, Bansod PY, Kale VB, Shah Y, Akhtar M. A comparative study of Desarda's technique with Lichtenstein mesh repair in treatment of inguinal hernia: A prospective cohort study. Int J Surg. 2017;39:150-5.
20. Youssef T, El-Alfy K, Farid M. Randomized clinical trial of Desarda versus Lichtenstein repair for treatment of primary inguinal hernia. Int J Surg. 2015;20:28-34.
21. Rodríguez P, Herrera P, Gonzalez O, Alonso J, Blanco H. A randomized trial comparing lichtenstein repair and no mesh desarda repair for inguinal hernia: a study of 1382 patients. East Central Afr J Surg. 2013;18:18-25.
22. Gaur AS, Sharma N, Garg PK. Chronic groin pain in Desarda versus Lichtenstein hernia repair - a randomised controlled study. S Afr J Surg. 2022;60:141-5.
23. Manyilirah W, Kijjambu S, Upoki A, Kiryabwire J. Comparison of non-mesh (Desarda) and mesh (Lichtenstein) methods for inguinal hernia repair among black African patients: a short-term double-blind RCT. Hernia. 2012;16:133-44.
24. Emile SH, Elfeki H. Desarda's technique versus Lichtenstein technique for the treatment of primary inguinal hernia: a systematic review and meta-analysis of randomized controlled trials. Hernia. 2018;22:385-95.
25. Abbas Z, Bhat S, Koul M. No mesh repair versus lichtenstein S open mesh repair of inguinal hernia. A Comp Study. 2015;22:56-63.
26. Mitura K, Rzewuska A, Skolimowska-Rzewuska M, Wyrzykowska D. Desarda technique as a valuable alternative for inguinal hernia patients refusing mesh implantation: long-term results fifteen years after a pure tissue repair in 198 patients. Mini Invasive Surg. 2021;5:22-6.
27. Szopinski J, Dabrowiecki S, Pierscinski S, Jackowski M, Jaworski M, Szuflet Z. Desarda versus Lichtenstein technique for primary inguinal hernia treatment: 3-year results of a randomized clinical trial. World J Surg. 2012;36:984-92.
28. Rodriguez P, Gonzàlez O, Rocha J, Herrera P, Castillo E, Casanova A, et al. A randomized trial comparing Desarda repair no mesh and Lichtenstein repair for inguinal hernia (A study of 2225 patients). Biomed J Sci Tech Res. 2018;6:5445-9.
29. Desarda MP. No-mesh inguinal hernia repair with continuous absorbable sutures: a dream or reality? (A study of 229 patients). Saudi J Gastroenterol. 2008;14:122-7.
30. Rodrà PRLp. A randomized trial. Comparing herniorrafia modifield desarda repair and hernioplastia lichtenstein repair for inguinal hernia (study of 1242 patients). Adv Res J Med Clin Sci. 2019;5:4-10.
31. Koksal N, Altinli E, Sumer A, Celik A, Onur E, Demir K, et al. Impact of herniorraphy technique on testicular perfusion: results of a prospective study. Surg Laparosc Endosc Percutan Tech. 2010; 20:186-9.
32. Lima Neto EVd, Goldenberg A, Jucá MJ. Estudo prospectivo dos efeitos da prótese de polipropileno sobre o volume e o fluxo arterial testicular em pacientes submetidos à correção cirúrgica de hérnia inguinal. Acta Cir Bras. 2007;22:266-71.
Full Text Sources:
Abstract:
Views: 943

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.