Surgery, Gastroenterology and Oncology

|
|
Background: hepatic hemangiomas, primarily affecting adults in their fourth and fifth decades, are common benign mesenchymal hepatic tumors. The management of giant hepatic hemangiomas, defined variably as greater than 4 cm to 10 cm in diameter, is a clinical challenge due to their potential size and associated symptoms. This study compares two minimally invasive treatment methods: trans-catheter arterial bleomycin chemoembolization (TACE) and ultrasound and fluoroscopy-guided transhepatic bleomycin sclerotherapy (PLIB), in the treatment of giant hepatic hemangiomas.
Methods: this prospective cohort study was conducted in Baghdad, Iraq, involved 20 patients with giant hepatic hemangioma. The study assessed the efficacy of TACE and PLIB by comparing tumor size reduction, symptom improvement, changes in radiological features, laboratory parameters, and treatment-related complications.
Results: the study observed no significant age difference between the two groups. Post-treatment CT scans revealed different enhancement patterns between TACE and PLIB, with TACE showing more uniform ischemic effects and PLIB demonstrating a variety of enhancement patterns. Both treatments effectively reduced the size of the hemangiomas, with PLIB showing a greater reduction in mass volume than TACE.
Conclusion: both TACE and PLIB are effective in reducing the size of giant hepatic hemangiomas, with initial results favoring PLIB for greater volume reduction. Further studies with larger samples and longer follow-up are needed to confirm these findings and establish long-term safety and efficacy profiles for these treatments.
Introduction
Hemangiomas are the most frequent benign mesenchymal hepatic tumors, with postmortem prevalence ranging from 3 % to 20% (1). These tumors primarily affect females and adults in their fourth and fifth decades of age (2). Because hepatic hemangiomas are frequently asymptomatic and individuals have normal liver function, their identification is usually accidental. Because the therapeutic plan for hepatic hemangioma is determined by tumor size, defining giant hepatic hemangioma is critical. Various definition criteria have been provided. The majority of authors employ the diameter > 4 cm threshold (3), while others use a size > 5 cm (4), and a minority choose a width > 10 cm (5). Giant hepatic hemangioma is found in less than 10% of cases (6).
The treatment of patients with a large hemangioma of the liver is still debatable. Surgical resection, radio-frequency ablation, microwave ablation, transarterial embolization, and percutaneous sclerotherapy are all options for treating hemangiomas (7). Surgical treatment has traditionally been the most successful treatment. However, it is frequently associated with significant trauma, difficulties, and substantial risks.
Transarterial embolization (TAE) produces arterial blood supply blockage and tumor shrinkage, and it is used to diminish hemangioma size, particularly when the tumor is greater than 20 cm in size (8). It is also used to treat preoperative hepatic hemangioma rupture (9). Its use has been linked with the possibility of ischemia, intracavitary hemorrhage, and infection (10).
Percutaneous sclerotherapy (PS) has been studied for treating hepatic hemangioma (7,11). Hepatic hemangiomas are classified as low-flow venous anomalies by the International Society for the Study of Vascular Anomalies (12), and PS is considered to be the preferred therapy for subcutaneous low-flow vascular abnormalities (7). In a preliminary study, patients with giant liver hemangioma received percutaneous sclero-therapy with a mixture of bleomycin and ethiodized oil. The volume and greatest diameter of the tumors, as well as pain severity, had decreased at the 5-month follow-up (13); however, the long-term efficacy of this kind of therapy in a larger number of patients is still unknown.
Bleomycin is a sclerosing agent with one of the lowest complication rates. Its adverse events have been both minimal and transient, so it can be used in any modality of radiological intervention (14). However, it may increase the risk of skin hyperpigmentation and ulceration if injected too superficially under the skin. It induces an endothelial-to-mesenchymal transition that enhances its scleroembolic effect (15).
There is currently no single radio-interventional approach consensus on the optimum care for patients with symptomatic and/or large hemangiomas. Therefore, we conducted this study to evaluate the efficacy and differences in different modalities of minimally invasive methods in the treatment of giant liver hemangioma.
Material andMethods
The study was conducted at Gazi Alhariry Teaching Hospital/Medical City Complex and Ibn Sina Hospital in Baghdad, Iraq, within the Department of Interventional Radiology. This prospective cohort study spanned from December 2022 to May 2023 and included a study population of 20 individuals with giant hepatic hemangioma to compare the effectiveness of trans-catheter arterial bleomycin chemoembolization and ultrasound and fluoroscopy-guided transhepatic bleomycin sclero-therapy in the treatment of giant hepatic hemangioma.
Study design
This study employed a follow-up cohort design to assess and compare the outcomes of two treatment approaches for giant hepatic hemangioma. Patients meeting the inclusion criteria were followed up over the study period to evaluate the efficacy of both interventions.
Inclusion Criteria
- Adults aged more than 18 years.
- Diagnosis of giant hepatic hemangioma with a size larger than 5 cm.
- Presence of symptoms such as pain and heaviness at the liver site.
- Abnormal investigation results, including low platelet counts, anemia, and abnormal liver function.
- Typical radiological features confirming the presence of hepatic hemangioma.
Exclusion Criteria
• Age younger than 18 years.
• Pregnancy status.
• Presence of small hemangiomas (5 cm or smaller).
• Asymptomatic cases.
• Atypical radiological features inconsistent with hemangioma.
• Elevated alpha-fetoprotein levels.
• Contraindication to sclerotherapy and catheterization procedures.
Data collection and procedures
Participants meeting the inclusion criteria underwent either trans-catheter arterial bleomycin chemo-embolization or ultrasound and fluoroscopy-guided transhepatic bleomycin sclerotherapy based on clinical indication. Data on patient demographics, medical history, symptomatology, laboratory investigations, and radiological features were collected at baseline.
Treatment plans (Fig. 1)
• Percutanous local injection of 60 IU of bleomycin.
• Trans arterial chemo embolization by (bleomycin-lipiodol emulsion).
Figure 1 - Hemangioma pre and post-embolization

Follow-up and Outcomes
Patients were closely monitored during the study period. Follow-up visits were scheduled at specific intervals to assess treatment outcomes, symptom improvement, changes in radiological features, and potential complications. Clinical assessments, laboratory investigations, and radiological imaging were conducted during follow-up visits.
Primary outcome
The primary outcome of this study is to compare the efficacy of trans-catheter arterial bleomycin chemo-embolization and ultrasound and fluoroscopy-guided transhepatic bleomycin sclerotherapy in terms of reducing the size of giant hepatic hemangiomas. The change in size will be assessed using radiological imaging (e.g., CT scans or MRI) at follow-up visits. Reduction in the size of the hemangioma indicates successful treatment response.
Secondary outcomes
- Symptom Improvement: The study will evaluate the improvement in symptoms such as pain and heaviness at the liver site after both treatment interventions. Participants' self-reported symptom relief will be recorded during follow-up visits.
- Changes in Radiological Features: Apart from size reduction, the study will assess other radiological changes in the hemangiomas, such as changes in internal structure, enhancement pattern, and vascularity. These changes will provide additional insight into the effectiveness of each treatment method.
- Laboratory Investigations: The study will monitor changes in laboratory parameters, including platelet counts, hemoglobin levels, and liver function tests. Improvements in these parameters may indicate a positive treatment response and overall liver health.
- Complications and Adverse Events: Both primary and secondary adverse events related to the treatment procedures will be recorded. This includes complications such as bleeding, infection, and any procedure-related adverse events.
- Patient Satisfaction: Participants' satisfaction with the treatment outcomes will be assessed using structured questionnaires. This will provide insights into the patients' perception of the treatment methods and their impact on their quality of life.
- Long-Term Follow-up: While the study's main period is from December 2022 to May 2023, the study may aim to include long-term follow-up data to assess the durability of treatment effects and the potential recurrence of hemangiomas.
Ethical considerations
Ethical approval was obtained from the institutional review board of both participating hospitals. Informed consent was obtained from all study participants before enrollment. Patient confidentiality and data privacy were maintained throughout the study.
Limitations
Possible limitations of the study include the relatively small sample size and potential biases inherent in observational cohort studies. Additionally, the study's generalizability might be limited to the specific population and settings under investigation.
Data analysis
In the data analysis of this study, the SPSS version 24 (IBM, NY, US) was used. The Chi-Square Test was utilized to explore associations between categorical variables. For continuous data, the Independent Sample T-Test was used to compare the means between two independent groups, particularly useful for data following a normal distribution. In instances where the data did not meet the normality assumption, the Mann-Whitney U Test was employed as a non-parametric alternative to the Independent Sample T-Test. Additionally, the Paired Sample Test was used for comparing means within the same group at different times. Confidence interval at 95% was considered in this study and significant variables were applied at P-Value <0.05.
Results
In the table 1, we present the demographic and treatment-related data for two groups, Group I (TACE) and Group II (PLIB), in a comparative analysis. The mean ages of the two groups were 38.88±4.97 years for Group I and 40.10±7.89 years for Group II, with no statistically significant difference observed (p = 0.708). The age range within each group was 16 years for Group I and 29 years for Group II, demonstrating the diversity of ages in both groups.
Table 1 - Age and Enchantment after the treatment distribution among the studied groups
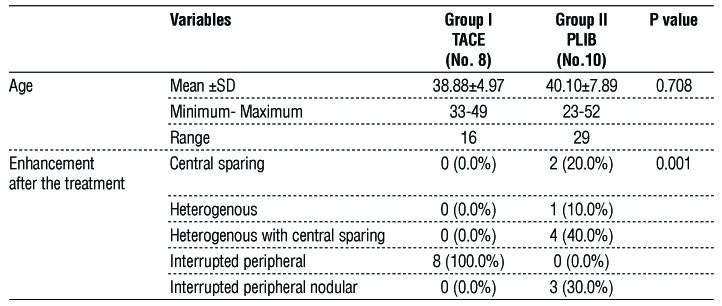
One of the treatment outcomes assessed in this table is the enhancement pattern observed after treatment. In Group I, all patients (100.0%) exhibited an interrupted peripheral enhancement pattern, while no patients had central sparing, heterogenous enhancement, or heterogenous enhancement with central sparing. In contrast, in Group II, the enhancement pattern showed a different distribution, with 20.0% of patients having central sparing, 10.0% exhibiting heterogenous enhancement, and 40.0% showing heterogenous enhancement with central sparing. None of the patients in Group II had an interrupted peripheral enhancement pattern. The differences in enhancement patterns between the two groups were statistically significant, with a p-value of 0.001.
The table 2 provide a comparative analysis of two groups, before treatment, the mean volume of the mass in Group I was 1262.27±1154.4 cubic units. In contrast, Group II had a lower mean volume of the mass before treatment, measuring 755.08±462.04 cubic units. After treatment, the mean volume of the mass in Group I decreased to 858.47±906.1 cubic units. Group II, on the other hand, exhibited a substantially lower mean volume of the mass after treatment, measuring 162.53±117.58 cubic units. Furthermore, the mean differences in volume (pre-treatment volume minus post-treatment volume) were calculated for both groups (fig. 2). Group I had a mean difference of 403.79 ±266.7 cubic units, while Group II had a larger mean difference of 592.54±490.83 cubic units. These mean differences were statistically significant, indicating notable changes in mass volume after treatment. Overall, this table demonstrates that both treatment modalities, TACE (Group I) and PLIB (Group II), were effective in reducing the volume of the mass. However, Group II (PLIB) showed a greater reduction in mass volume, as evidenced by the lower mean volume after treatment and a larger mean difference in volume compared to Group I (TACE).
Table 2 - Mass volume differences among the studied groups
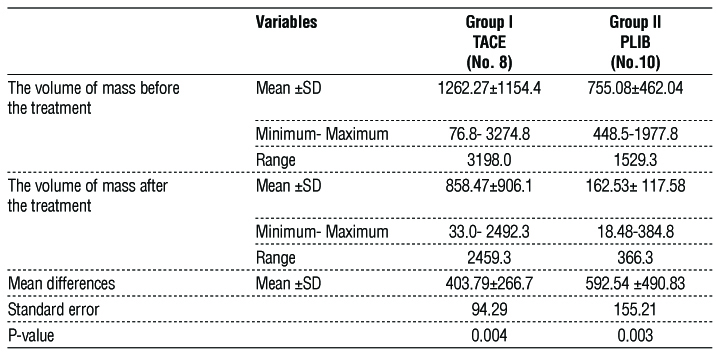
Figure 2 - Mass volume differences before and after treatment among the studied groups
Discussion
Symptomatic cases of hemangiomas are, generally, treated by surgery. However, giant liver hemangiomas, which are tumors larger than 5cm in diameter, pose a clinical challenge due to their high risk of surgical complications (16). Over the past years, several methods of interventional radiology have evolved as nonsurgical alternatives (17), however, there is no well-established optimal strategy for managing these lesions (16). In the pursuit of effective treatment options, we compared the efficacy of trans-catheter arterial bleomycin chemoembolization (TACE) with ultrasound and fluoroscopy-guided transhepatic bleomycin sclerotherapy (PLIB) in two distinct groups. In this study, a wide spectrum of adult ages was observed. This suggests that both TACE and PLIB can be applied across a broad age range of patients. It is notable that despite the broader age range in Group II, the lack of statistical significance indicates that age did not play a differential role in treatment response.
We reported a distinct enhancement pattern in post-treatment CT scans between the two groups. TACE (Group I) leads to a more uniform ischemic effect, as evidenced by the interrupted peripheral enhancement observed in all patients. This uniformity could be due to the arterial delivery of TACE, which may distribute the therapeutic agent more homogeneously. TACE involves injecting chemotherapy drugs directly into the primary blood vessels that supply the hemangioma, which are identified accurately by arteriography (18). Bleomycin is an antineoplastic agent that inhibits DNA biosynthesis used in treatment of squamous cell carcinoma, lymphomas, testicular carcinoma and others (19, 20). A study by Oikawa et al. in 1990 first reported that bleomycin also exerts antiangiogenic effects by causing sclerosis of blood vessels endothelial cells (21). It is often administered with iodized oil, known as lipiodol, which is an embolic agent that serves as a delivery method (22), and also has the ability to block blood flow to tumors due to its tumor-philic properties (23). This combination is delivered directly to hemangiomas through arterial catheters, where it selectively accumulates within tumor nodules, ensuring that the chemo-therapeutic agent comes into direct contact with the tumor cells (24) and remains for several weeks to over 12 months leveraging the tumor's high vascularity and lack of Kupffer cells (25). According to research by Halil Bozkaya et al. in 2014, a combination of bleomycin and lipiodol causes destruction of endothelial cells, and induces chronic sclerosing effect, resulting in tumor atrophy and fibrosis (26).
Conversely, post-treatment CT scans of patients with giant hepatic haemangioma typically revealed non-uniform enhancement patterns in this study. The most commonly observed was heterogeneous enhancement with central sparing (40%). While 30% displayed peri-pheral nodular interrupted enhancement. Less frequently observed were central sparing enhancement in 20% of the cases, and heterogeneous enhancement in 10% of the patients. These findings are similar to Rafid et al. study in Iraq, that showed heterogenous enhancement with central sparing was the most common pattern, followed by, peripheral nodular interrupted enhancement, central sparing enhancement, and lastly heterogeneous enhancement (27). The variety of enhancement patterns in PLIB (Group II) indicates a less consistent response than group I, potentially due to the different delivery method. In PLIB, percutaneous access to the hemangioma is achieved using spinal needle under ultrasound guidance, passing through normal liver parenchyma before entering the lesion to minimize the risk of bleeding. Then bleomycin is injected intralesionally under fluoroscopy, unlike the arterial drug delivery of TACE (28). The slow blood flow in hemangioma allows for the extended retention of bleomycin post-injection, potentiating its damage to the endothelial lining, and eventually leading to tissue ischemia and necrosis (16).
Moreover, the findings in this research indicate that both TACE and PLIB are effective in reducing size of hepatic hemangiomas. Up to date, there is currently no published study that directly compares the effectiveness of these two procedures. Nevertheless, numerous research studies have independently examined the efficacy of each procedure. A large retrospective study by Li et al. involving 836 patients with 1120 hepatic hemangioma lesions treated with transarterial embo-lization, reported a 100% treatment success rate (29). Similarly, a meta-analysis by Pooya et al. comprising 1450 patient showed symptomatic improvement following hemangioma size reduction in 63.3%–100% of the cases(30). Regarding efficacy of PLIB, a study by Hossein et al. (31) and another by Niloofar et al. (11) both revealed significant size reduction and symptoms improvement in patients with giant hepatic hemangioma. Findings in these mentioned studies align with this study regarding effectiveness of both procedures. Furthermore, in this research, it was found that PLIB (Group II) appears to be more effective than TACE (Group I) in terms of absolute volume reduction. However, patients follow up for more extended periods of time is needed to determine its safety and superiority over TACE. This finding contradicts some researches that considered transarterial embolization as the preferred interventional radiology option for multiple and/or giant lesions (16,29). Furthermore, only a few studies discussed percutaneous sclerotherapy as a treatment giant hepatic hemangioma. This is possibly due to its high risk of intraperitoneal hemorrhage caused by repeated puncture (16).
Limitations of the study
The retrospective nature of the study introduces inherent biases and limits the establishment of causation. Additionally, the choice of treatment modalities was based on clinical indication, potentially leading to selection bias. The relatively small sample size may impact the generalizability of our findings to a broader population. Furthermore, the duration of the study may also be considered a limitation, as extended follow-up periods are essential to detect long-term treatment effects and potential complications. Lastly, the lack of a control group receiving no intervention, or an alternative treatment option limits our ability to make direct comparisons and draw definitive conclusions about the superiority of one approach over the other.
Conclusion
In conclusion, both TAC and PLIB demonstrate effectiveness in reducing the size of hepatic hemangiomas. Initial findings suggest that PLIB may yield a more significant absolute volume reduction compared to TACE. However, the determination of its safety
profile and long-term superiority over TACE necessitates extended follow-up periods.
Disclosure: None
References
1. Öztoprak HS, Balli TH, Aikimbaev K, Onan HB, Karluka I, et al, editors. Endovascular management of giant cavernous haemangiomas: single center experience2017: European Congress of Radiology-ECR 2017.
2. Singh AP, Tanger R, Mathur V, Gupta AK, Mehra S. Unusual presentation of capillary he mangioma of liver in a neonate: a case report. J Evol Res Paediatr Neonatol. 2016;2:13-5.
3. Schnelldorfer T, Ware AL, Smoot R, Schleck CD, Harmsen WS, Nagorney DM. Management of giant hemangioma of the liver: resection versus observation. J Am Coll Surg. 2010;211(6):724-30. Epub 2010 Oct 25.
4. Grieco MB, Bg M. Giant hemangiomas of the liver. 1978.
5. Van Tilborg AA, Nielsen K, Scheffer HJ, Van den Tol P, van Waesberghe J, Sietses C, et al. Bipolar radiofrequency ablation for symptomatic giant (> 10 cm) hepatic cavernous haemangiomas: initial clinical experience. Clin Radiol. 2013;68(1):e9-e14. Epub 2012 Nov 10.
6. Angeles GL-A, Barahona-Garrido J, Tellez-Avila FI, Burgos-Zuleta L, Lopez-Placier T, Llamas-Gutiérrez FJ, et al. A giant hepatic hemangioma treated successfully with hepatic enucleation. Ann Hepatol. 2009;8(4):377-8.
7. Lin Z, Zhu X, Zhou J. Ultrasound-guided percutaneous sclero-therapy versus surgical resection in the treatment of large hepatic hemangiomas: a retrospective study. BMC Surgery. 2022;22(1):130.
8. Vassiou K, Rountas H, Liakou P, Arvanitis D, Fezoulidis I, Tepetes K. Embolization of a giant hepatic hemangioma prior to urgent liver resection. Case report and review of the literature. Cardiovasc Intervent Radiol. 2007;30(4):800-2.
9. Ho H-Y, Wu T-H, Yu M-C, Lee W-C, Chao T-C, Chen M-F. Surgical management of giant hepatic hemangiomas: complications and review of the literature. Chang Gung Med J. 2012;35(1):70-8.
10. Seo H-I, Jo HJ, Sim MS, Kim S. Right trisegmentectomy with thoracoabdominal approach after transarterial embolization for giant hepatic hemangioma. World J Gastroenterol. 2009;15(27):3437-9.
11. Ayoobi Yazdi N, Mehrabinejad M-M, Dashti H, Pourghorban R, Nassiri Toosi M, Yazdi HR. Percutaneous sclerotherapy with bleomycin and ethiodized oil: a promising treatment in symptomatic giant liver hemangioma. Radiology. 2021;301(2):464-471.
12. Merrow AC, Gupta A, Patel MN, Adams DM. 2014 revised classification of vascular lesions from the international society for the study of vascular anomalies: radiologic-pathologic update. Radiographics. 2016;36(5):1494-516.
13. Yazdi NA, Dashti H, Batavani N, Borhani A, Shakiba M, Yazdi HR. Percutaneous sclerotherapy for giant symptomatic liver hemangiomas: a pilot study. J Vasc Interv Radiol. 2018;29(2):233-236.
14. Wen S-Q, Wan M, Len K-M, Hu Q-H, Xie X-Y, Wu Q, et al. Safety and efficacy of laparoscopic radiofrequency ablation for hepatic hemangiomas: a multicenter retrospective study. Ann Hepatol. 2018;17(2):268-273.
15. Gao J, Ji J-S, Ding X-M, Ke S, Xin Z-H, Ning C-M, et al. Laparoscopic radio-frequency ablation for large subcapsular hepatic hemangiomas: technical and clinical outcomes. PLoS One. 2016;11(2): e0149755.
16. Dong W, Qiu B, Xu H, He L. Invasive management of symptomatic hepatic hemangioma. Eur J Gastroenterol Hepatol. 2019;31(9): 1079-1084.
17. Jia K, Gao Z, Li M, Yu C. Interventional treatments for hepatic hemangioma: A state-of-the-art review. J Interv Med. 2022;5(1):6-9.
18. Kaca?a A, Dorochowicz M, Patrza?ek D, Janczak D, Guzinski M. Safety and Feasibility of Transarterial Bleomycin–Lipiodol Embolization in Patients with Giant Hepatic Hemangiomas. Medicina. 2023;59(8): 1358.
19. Hecht SM. Bleomycin: new perspectives on the mechanism of action. J Nat Prod. 2000;63(1):158-68.
20. Mir L, Tounekti O, Orlowski S. Bleomycin: revival of an old drug. Gen Pharmacol. 1996;27(5):745-8.
21. Oikawa T, Hirotani K, Ogasawara H, Katayama T, Ashino-Fuse H, Shimamura M, et al. Inhibition of angiogenesis by bleomycin and its copper complex. Chem Pharm Bull (Tokyo). 1990;38(6):1790-2.
22. Ohishi H, Uchida H, Yoshimura H, Ohue S, Ueda J, Katsuragi M, et al. Hepatocellular carcinoma detected by iodized oil. Use of anticancer agents. Radiology. 1985;154(1):25-9.
23. Sun J-H, Nie C-H, Zhang Y-L, Zhou G-H, Ai J, Zhou T-Y, et al. Transcatheter Arterial Embolization Alone for Giant Hepatic Hemangioma. PLoS One. 2015;10(8):e0135158.
24. Yazdi NA, Mehrabinejad M-M, Dashti H, Pourghorban R, Toosi MN, Yazdi HR. Percutaneous Sclerotherapy with Bleomycin and Ethiodized Oil: A Promising Treatment in Symptomatic Giant Liver Hemangioma. Radiology. 2021;301(2):464-471.
25. Shin SW. The current practice of transarterial chemoembolization for the treatment of hepatocellular carcinoma. Korean J Radiol. 2009; 10(5):425-34.
26. Bozkaya H, Cinar C, Besir FH, Par?ldar M, Oran I. Minimally invasive treatment of giant haemangiomas of the liver: embolisation with bleomycin. Cardiovasc Intervent Radiol. 2014;37(1):101-7. Epub 2013 Apr 12.
27. Abdulazeez RA MR, Kadhim ZH. Percutaneous trans-hepatic local sclerotherapy of symptomatic giant liver hemangioma. Onkologia i Radioterapia. 2023;17(7):116-120.
28. Ghaemi O, Mehrabi Nejad M-M, Rouhezamin MR, Ayoobi Yazdi N, Pourghorban R, Yazdi HR. A technical review of percutaneous sclerotherapy with bleomycin for giant hepatic venous malformation. CVIR Endovasc. 2023;6(1):46.
29. Li Y, Jia Y, Li S, Wang W, Wang Z, Wang Y, et al. Transarterial chemoembolization of giant liver haemangioma: a multi-center study with 836 cases. Cell Biochem Biophys. 2015;73(2):469-472.
30. Torkian P, Li J, Kaufman JA, Jahangiri Y. Effectiveness of Transarterial Embolization in Treatment of Symptomatic Hepatic Hemangiomas: Systematic Review and Meta-analysis. Cardiovasc Intervent Radiol. 2021;44(1):80-91. Epub 2020 Aug 17.
31. Ghanaati H, Abrishami A, Hashem Zadeh A, Ghiasi M, Nasiri Toosi M, Jafarian A. Computed Tomography Fluoroscopy–Guided Percutaneous Transhepatic Bleomycin/Ethiodized Oil Sclerotherapy for Symptomatic Giant Hepatic Hemangioma. J Vasc Interv Radiol. 2022;33(11):1342-1348.e1.
Full Text Sources:
Abstract:
Views: 5385

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.