Surgery, Gastroenterology and Oncology

|
|
Background: Successful biliary cannulation is a crucial step in ERCP, and different techniques are employed to overcome challenging cannulation, aiming to enhance success rates and minimize post-ERCP complications, particularly post-ERCP pancreatitis. Our study aimed to compare the efficacy of needle knife fistulotomy (NKF) and double guide wire (DGW) techniques in addressing difficult biliary cannulation following repeated unintentional pancreatic duct cannulation during ERCP.
Methods: Forty subjects undergoing ERCP at Menoufia University hospitals, following failed biliary cannulation attempts of 5 minutes with repeated unintentional pancreatic duct cannulation, were included. Early intervention with NKF or DGW was performed for successful biliary cannulation. Patients were divided into two groups: DGW group (20 patients) and fistulotomy group (20 patients).
Results: Our study found no significant difference between the groups in terms of ERCP
success rates, with a success rate of 75% in the DGW group and 90% in the fistulotomy group (p-value = 0.2). Similarly, there was no significant difference in post-ERCP pancreatic inflammation between the groups, with rates of 30% in the DGW group and 10% in the fistulotomy group (p-value = 0.1).
Conclusion: The double-guidewire technique emerges as a viable and safe alternative to
needle-knife fistulotomy in cases of difficult biliary cannulation.
INTRODUCTION
In the contemporary medical landscape, endoscopic retrograde cholangio-pancreatography (ERCP) serves as a global standard for treating pancreatic and biliary disorders. Achieving selective deep biliary cannulation stands as a pivotal precursor to subsequent therapeutic interventions within the biliary system, yet approximately ten to twenty percent of cases encounter difficulties in achieving this with a native major papilla (1).
The successful cannulation of the intended duct plays a critical role in ensuring the efficacy of biliary and pancreatic techniques during ERCP (2). In instances where conventional methods fall short in achieving selective biliary cannulation, alternative techniques are sought. However, prolonged and repeated manipulations of the papilla during various methods heighten the risk of post-ERCP pancreatitis (PEP) (3).
Challenges in achieving cannulation of the common bile duct (CBD) exacerbate post-ERCP complications, notably post-ERCP pancreatic inflammation and cholangitis. Consequently, extensive efforts have been made to develop effective endoscopic procedures that facilitate proper cannulation while mitigating PEP. Among these, precut sphincterotomy techniques such as NKF and needle knife papillotomy (NK) have emerged as commonly utilized approaches for cases with difficult cannulation (4,5).
Notably, NKF may be associated with a lower incidence of post-ERCP pancreatic inflammation compared to needle knife papillotomy, possibly attributed to the incision type being a few millimeters away from the papillary opening (6). Additionally, double guide wire technique (DGT) has proven valuable in managing challenging biliary cannulation (7,8).
Our study aims to assess whether needle knife fistulotomy or the double guide wire technique is superior in addressing complicated biliary cannulation resulting from inadvertent repetitive pancreatic duct cannulation and its correlation with post-ERCP pancreatitis.
MATERIAL AND METHODS
Patients supplied informed consent after our study was authorised by the Menoufia University Faculty of Medicine's ethical committee. The study was done on forty patients who were admitted in Menoufia University hospital for diagnostic and therapeutic ERCP purposes. Patients were recruited from Menoufia University Hospital, encompassing both the internal medicine outpatient clinic and inpatient ward, during the period spanning from December 2021 to September 2023. All sequential patients undergoing ERCP, following unsuccessful biliary cannulation despite multiple attempts lasting 5 minutes, coupled with repetitive inadvertent cannulation of the pancreatic duct, underwent prompt intervention with either early NKF or DGW technique to facilitate successful biliary cannulation. Side-view endoscopes (Olympus TJF-160) was used. The following electrosurgical units were utilised: WEM SS-200E, Erbe ICC 200, and ValleyLab Force FX.
Patients classified into two groups
Patients were divided into groups using a simple randomization method, where individuals were listed and then assigned to either the Double Guide Wire or Fistulotomy group through random numbers generated by a random number generator. The Double Guide Wire group consisted of 20 treatment-naive patients indicated for diagnostic and therapeutic ERCP, while the Fistulotomy group comprised 20 similarly indicated patients.
Inclusion criteria encompassed cases aged 15 years or older with native papillae, while exclusion criteria included age younger than 15 years, pregnancy, upper gastrointestinal stricture, prior surgeries such as gastrectomy and choledochoenterostomy, and ampullary tumors.
Patients underwent comprehensive evaluations, including history taking (age & gender), thorough clinical examination (temperature, weight loss, biliary colics, and itching), laboratory investigations (pre- and post-ERCP) comprising CBC, AST, ALT, total and direct bilirubin, alkaline phosphatase, amylase, and lipase, along with pelviabdominal ultrasound and MRCP.
Endoscopic Retrograde Cholangiopancreatography was performed using a standard technique with a side-view endoscope (Olympus TJF-160). Cholangiography ensued after selective cannulation of the CBD with a catheter, and a 0.035-inch guidewire (Boston Scientific, Corp, MA, USA) was introduced via the catheter to access the biliary system. Following successful cannulation of the Common Bile Duct, an initial cholangiogram was obtained to assess the duct's diameter and width relative to the endoscope's shaft.
Group 1: Needle-knife fistulotomy technique (NKFT)
A 4.4 Fr sphincterotome and a 0.035-inch guidewire were used to cannulate the papillary ostium. Direct cutting current (50 watts). Fistulotomy required a 30-watt pure cut current.
Unsuccessful cannulation was diagnosed if it lasts more than 10 min, required more than 5 cannulation attempts, or when more than two pancreatic duct permeations happened. Complicated patients were directed to PF. In techniques that last for long time, prophylactic plastic stenting of pancreatic duct was done.
A needle-knife catheter (MicroKnife XL; Boston Scientific) was used to make an incision on the mucosal surface, working from distal to proximal and aiming towards the papilla's tip. It includes everything above the papillary orifice and the first two-thirds of the papillary protuberance. A pure cutting current (30 watts) was applied to cut the mucosa and the choledochal sphincter. The incision was ended after restoration of biliary secretion, opening the mucosa of the bile duct, or identification of bulged bile duct mucosa. a guidewire and sphincterotome were used to cannulate the fistula through the bile duct, and it was widened through incising the sphincter, to the limit of the transverse mucosal fold. Demographic, Clinical and Laboratory data of the cases were tabulated.
Group 2: Double-guidewire technique (DGT)
Guidewire was inserted into the pancreatic duct in subjects when CBD cannulation was unsuccessful, and the guidewire selectively passed through the duct on each attempt. The first guidewire was left in place in the critical pancreatic duct, and a second guidewire was threaded alongside it and through the duodenoscope's working channel to insert a sphincterotome.
Statistical analysis
IBM SPSS Statistics Version 22. 2013. Statistical Analysis with IBM SPSS for Windows, Release 22.0 Data was analyzed using IBM software developed in Armonk, New York. statistical data was represented by Mean and Standard Deviation (mean ± SD), qualitative variables were expressed as frequency or percentage, chi square test was done to evaluate the relation between two qualitative groups, t-test was to evaluate the relation between two quantitative groups.
Details about tools were used in this study: US: company manufacturing (Philips), country (Netherlands), city (Amsterdam). MRCP: company manufacturing (Siemens), country (Germany), city (Berlin). ERCP: company manufacturing (Olympus Corporation), country (Japan), city (Tokyo).
RESULTS
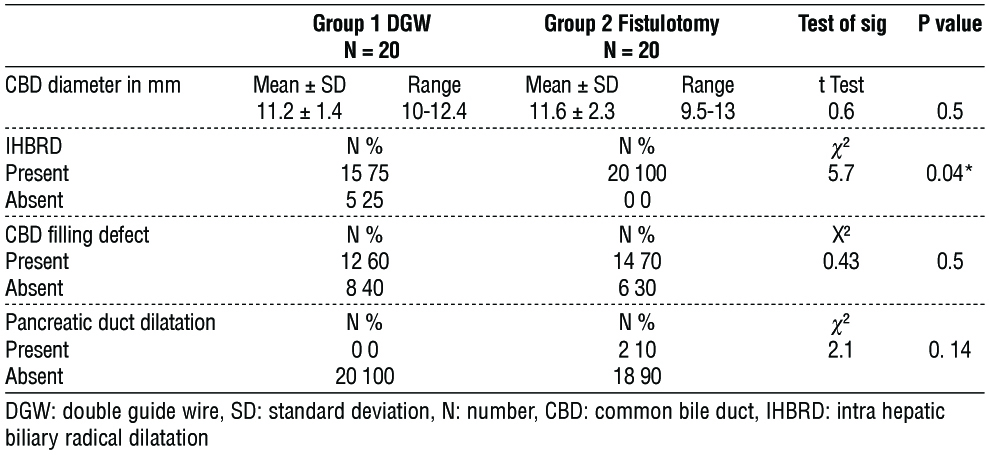
The studied groups exhibited similarity in socio-demographic and clinical characteristics, ERCP indications, CBD diameter, presence of CBD filling defect, and CBD stones (p-value > 0.05). However, IHBRD was significantly higher in the fistulotomy group compared to the DGW group (p-value = 0.04) (table 1).
Figure 1 - Study flow diagram
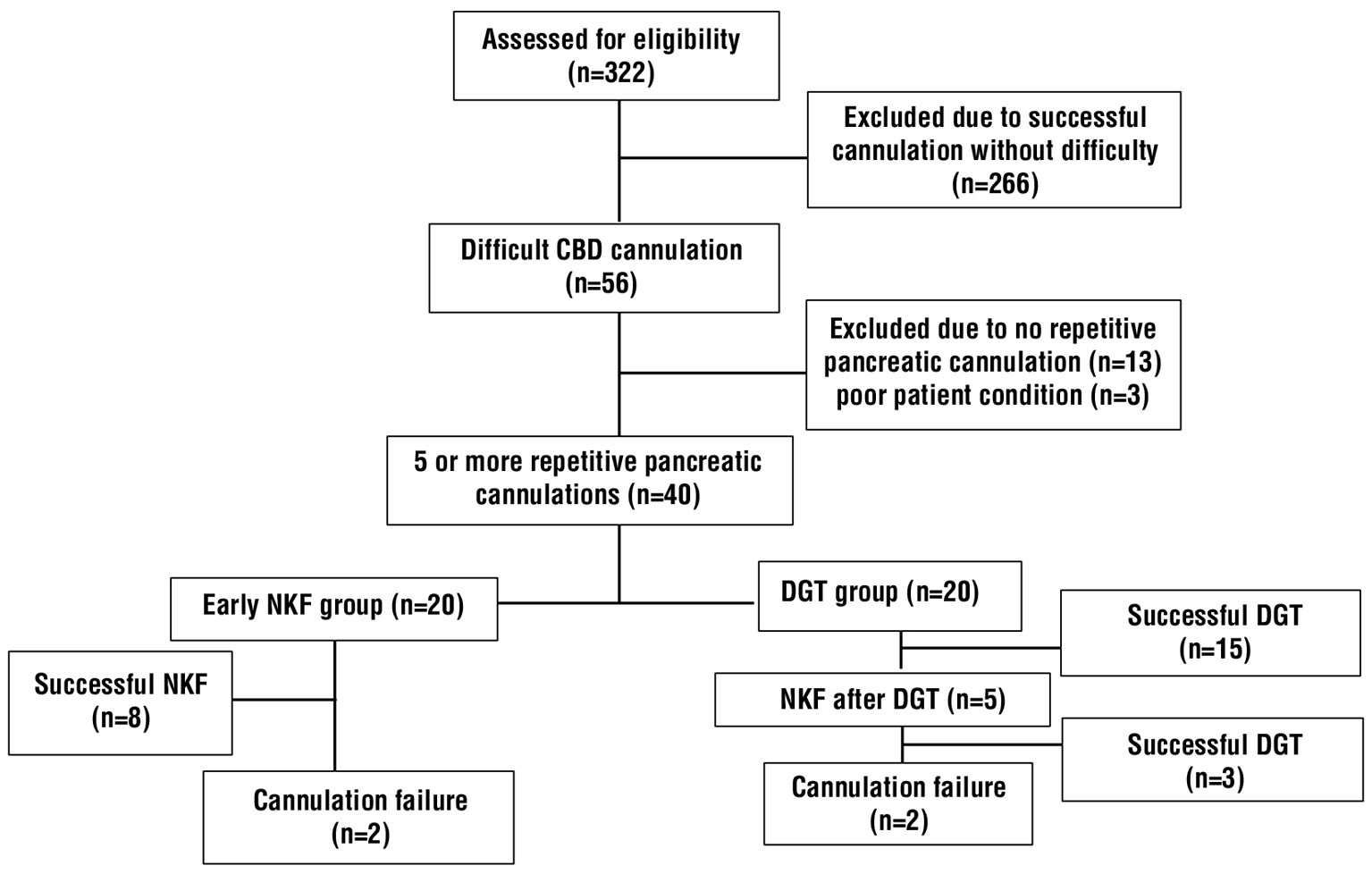
Table 1 - MRCP findings in patients of studied groups
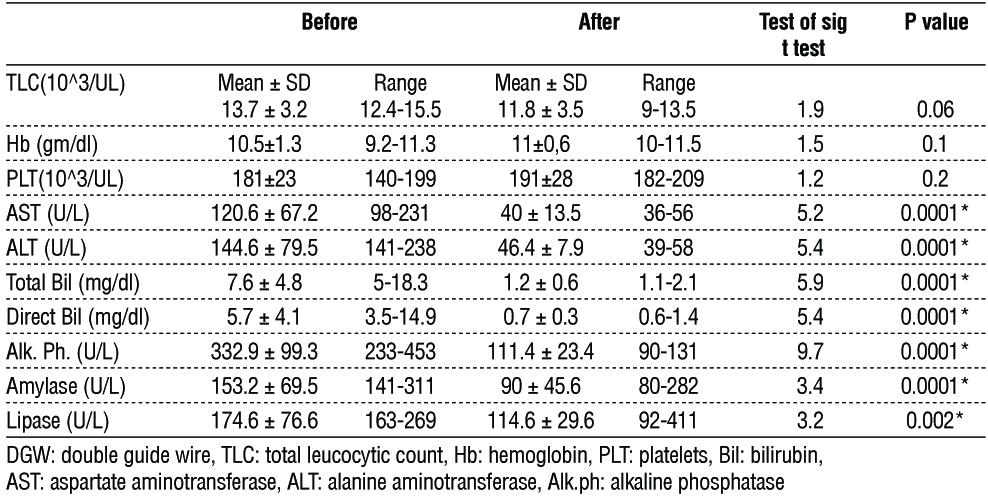
Regarding the DGW groups, no significant difference was noted in CBC before and after ERCP. However, a highly significant difference was observed in liver enzymes, total bilirubin, direct bilirubin, alkaline phosphatase, amylase, and serum lipase before and after ERCP (table 2).
Table 2 - Laboratory findings in patients of group 1 (DGW group)
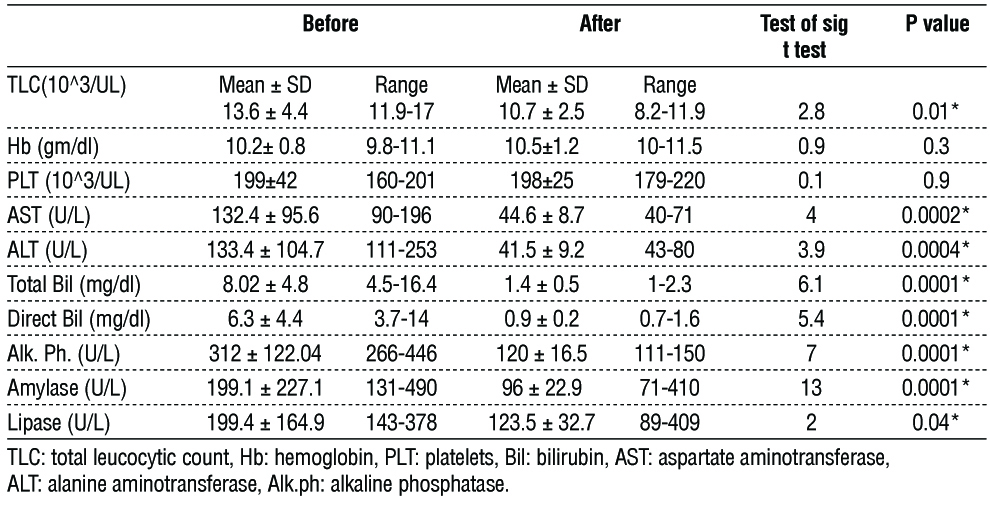
Similarly, among patients in the fistulotomy groups, there was no significant difference in Plt and Hb before and after ERCP. Nevertheless, a highly significant difference was evident in SGOT, SGPT, total bilirubin, direct bilirubin, ALP, amylase, TLC, and serum lipase before and after ERCP (table 3).
Table 3 - Laboratory findings in patients of group 2 (Fistulotomy group)
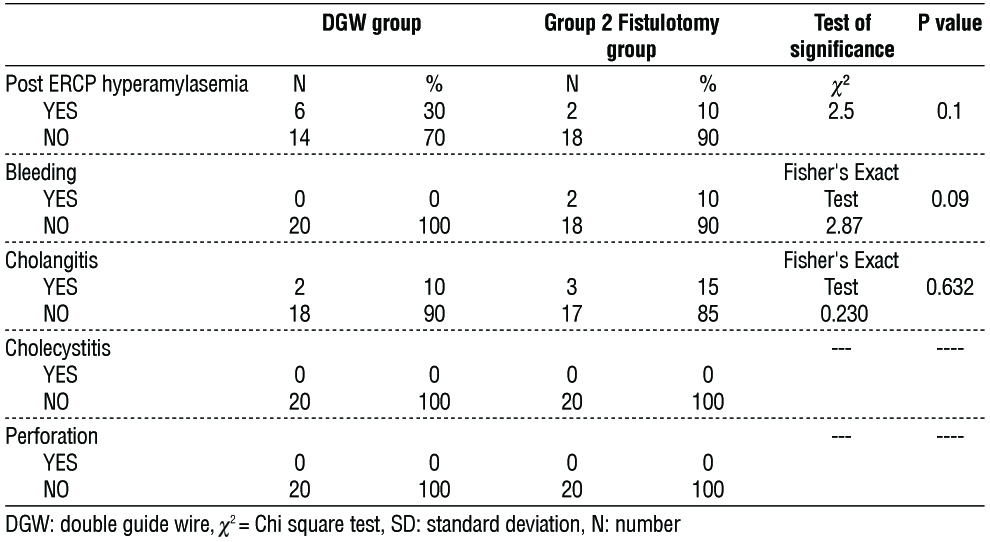
Furthermore, our study found no significant disparity between the studied groups concerning successful biliary cannulation and post-ERCP pancreatitis (tables 4, 5).

Discussion
Achieving proper cannulation of the intended duct is paramount in biliary and pancreatic techniques during ERCP. Conventional methods yield success rates for biliary cannulation ranging from 80% to 95% (8). In cases where traditional procedures fail, alternative methods are often pursued. However, the risk of post-ERCP pancreatitis (PEP) escalates with repeated or prolonged manipulation of the papilla.
Consequently, numerous endeavors have focused on refining endoscopic techniques to achieve effective cannulation and reduce the incidence of PEP. The most commonly employed methods in cases of unsuccessful cannulation include precut sphincterotomy, such as needle-knife fistulotomy (NKF) and needle-knife papillotomy (9). Additionally, the double-guidewire technique (DGT) has been utilized to address difficult bile duct cannulation (10).
Thus, the aim of this study was to assess the efficacy of needle knife fistulotomy versus the double guide wire technique in overcoming challenging biliary cannulation due to repetitive unintentional pancreatic duct cannulation, with a focus on post-ERCP pancreatitis. The study encompassed 40 patients admitted to Menoufia University Hospital for ERCP following unsuccessful cannulation attempts lasting 5 minutes, accompanied by repeated unintentional pancreatic duct cannulation. Early intervention with either NKF or DGT was performed to facilitate proper bile duct cannulation.
Our results indicate that the outcomes of the NKF technique were comparable to those of the DGW technique for managing difficult biliary cannulation, with similar risks of post-ERCP pancreatitis. The average age of participants was 53.6 ± 10.03 in the DGW group and 50.1 ± 15.1 in the Fistulotomy group, with a majority being females (55%). Clinical examination, laboratory parameters, ERCP indications, CBD diameter, presence of stones, CBD filling defect, and pancreatic duct dilatation did not significantly differ between the groups.
Notably, the fistulotomy group exhibited a higher percentage of intrahepatic biliary dilatation in response to biliary obstruction (IHBRD) and direct bilirubin compared to the DGW group. Similar to our findings, (11) also reported no significant differences in baseline characteristics (age, sex, ERCP indication).
Furthermore, our study demonstrated a significant decrease in AST, ALT, total bilirubin, direct bilirubin, alkaline phosphatase, amylase, and lipase levels after ERCP compared to baseline levels in the DGW group. However, TLC, hemoglobin, and platelet count did not significantly differ before and after ERCP in the DGW group.
In the Fistulotomy group, there was a significant decrease in TLC, AST, ALT, Total Bil, Direct Bil, Alk. Ph., Amylase, and Lipase levels after ERCP compared to pre-ERCP levels. However, there was no significant difference in Hb and PLT levels before and after ERCP. Regarding ERCP indications, in the DGW group, 12 (60%) patients had calculous obstructive jaundice, and 8 (40%) had malignant obstructive jaundice. In the Fistulotomy group, 14 (70%) patients had calculous obstructive jaundice, and 6 (30%) had malignant obstructive jaundice.
Consistent with our findings, Lee et al. (12) reported that ERCP was predominantly performed for CBD stones (73.0%) followed by malignancy-related biliary stenosis (22.1%). Guzmán-Calderón et al. (13) also observed that ERCP was conducted mostly for benign conditions (59.7%), with choledocholithiasis being the leading cause, followed by cancers (32.5%).
In our study, all participants underwent successful biliary cannulation utilizing various techniques, with standard cannulation being the primary approach and DWG and NJF techniques utilized in cases of unsuccessful cannulation. The Fistulotomy group achieved a 90% success rate, while the DGW group achieved a 75% success rate.
These results are consistent with Kim et al. (11), who reported a 79.1% success rate in the early NKF group and a lower rate of 44.8% in the DGW group. Similarly, Lee et al. (14) reported an overall cannulation success rate of 90.4% with Needle Knife Fistulotomy.
The success rate in our study (75% in the DGW group) was comparable to previous studies by Ito et al. (15) and Angsuwatcharakon et al. (16), which reported rates of 73% and 73.9%, respectively, but significantly higher compared to Herreros de Tejada et al. (10) and Coté et al. (17), who reported rates of 47% and 50%, respectively.
The high success rate in our study may be attributed to its prolonged surgical duration and relatively small sample size. Even with limited resources and the guidance of a single endoscopic expert, effective bile duct cannulation can be achieved using DGT.
Our study indicates an insignificant difference in ERCP outcomes between the studied groups. Zou et al. (18) similarly observed proper biliary cannulation in 88.9% of cases in the sequential PDGP group compared to 70.0% in the NKPS group, with no significant difference between the two groups. In contrast, Kim et al. (11) reported a higher success rate in the fistulotomy group compared to the DGW group. Previous studies have indicated that biliary cannulation using NKF yields higher success rates (ranging from 83% to 96%), while DGT shows variable rates of proper biliary cannulation (ranging from 47% to 92.6%) (6,10,16,19-21).
Our study identified a post-ERCP PEP rate of 30% in the DGW group, which exceeded the rate reported by Guzmán-Calderón et al. (13) (22.2%) for DGW-T. Additionally, prior research by Herreros de Tejada (10) indicated an elevated incidence of PEP following DGW-T (17%).
Conversely, a study in Peru documented a lower incidence of PEP with DGW-T at 8.3% (22). Variations in post-ERCP pancreatitis rates may be linked to differences in surgical duration, while the use of prophylactic pancreatic stents in certain studies could contribute to the lower incidence of PEP observed in those investigations.
Moreover, our study found no significant disparity in post-ERCP pancreatitis between the studied groups. The double-guidewire approach was associated with a higher pancreatitis rate compared to the fistulotomy group, although the difference lacked significance.
In accordance with our results, Zou et al. (19) reported PEP in 12.7% of cases in the sequential PDGP group and 10.0% in the NKPS group, with no significant difference between the two groups. However, in contrast to our findings, Kim et al. (11) demonstrated a significantly lower rate of PEP in the early NKF group compared to the DGT group.
Conclusion
Needle knife fistulotomy technique demonstrates superior efficacy over the double guide wire technique in addressing challenging biliary cannulation while posing a lower risk of post-ERCP pancreatitis. The NKF technique emerges as a preferred method for achieving successful cannulation with reduced post-procedural complications compared to the DGW approach.
Conflict of interest
No conflict of interest.
Ethical statement
Patients supplied informed consent after our study was authorized by the Menoufia University Faculty of Medicine’s ethical committee under no/2-2023INTM5-1.
References
- Pécsi D, Farkas N, Hegyi P, Balaskó M, Czimmer J, Garami A, et al. Transpancreatic sphincterotomy has a higher cannulation success rate than needle-knife precut papillotomy – a meta-analysis. Endoscopy. 2017;49(09):874-887.
- Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005;61(1):112-25.
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman DJ, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001;54(4): 425-34.
- Udd M, Kylänpää L, Halttunen J. Management of difficult bile duct cannulation in ERCP. World J Gastrointest Endosc. 2010;2(3):97-103.
- Zhang QS, Xu JH, Dong ZQ, Gao P, Shen YC. Success and Safety of Needle Knife Papillotomy and Fistulotomy based on Papillary anatomy: a prospective controlled trial. Digestive diseases and sciences. 2022;67(5):1901-9.
- Katsinelos P, Gkagkalis S, Chatzimavroudis G, Beltsis A, Terzoudis S, Zavos C, et al. Comparison of three types of precut technique to achieve common bile duct cannulation: a retrospective analysis of 274 cases. Dig Dis Sci. 2012;57(12):3286-92.
- Maeda S, Hayashi H, Hosokawa O, Dohden K, Hattori M, Morita M, et al. Prospective randomized pilot trial of selective biliary cannulation using pancreatic guide-wire placement. Endoscopy. 2003;35(9): 721-4.
- Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005;61(1):112-25.
- Lim JU, Joo KR, Cha JM, Shin HP, Lee JI, Park JJ, et al. Early use of needle-knife fistulotomy is safe in situations where difficult biliary cannulation is expected. Digestive diseases and sciences. 2012; 57:1384-90.
- de Tejada AH, Calleja JL, Díaz G, Pertejo V, Espinel J, Cacho G, et al. Double-guidewire technique for difficult bile duct cannulation: a multicenter randomized, controlled trial. Gastrointestinal Endoscopy. 2009;70(4):700-9.
- Kim SJ, Kang DH, Kim HW, Choi CW, Park SB, Song BJ, et al. Needle-knife fistulotomy vs double-guidewire technique in patients with repetitive unintentional pancreatic cannulations. World J Gastroenterol. 2015;21(19):5918-25.
- Lee YS, Cho CM, Cho KB, Heo J, Jung MK, Kim SB, et al. Difficult Biliary Cannulation from the Perspective of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis: Identifying the Optimal Timing for the Rescue Cannulation Technique. Gut Liver. 2021;15(3):459-465.
- Guzmán-Calderón E, Martinez-Moreno B, Casellas JA, Aparicio JR. Transpancreatic precut papillotomy versus double-guidewire technique in difficult biliary cannulation: a systematic review and meta-analysis. Endosc Int Open. 2021;9(11):E1758-E1767.
- Lee YJ, Kang DH, Kim HW, Park SB, Kim SJ, Nam HS, et al. Usefulness and Complications of Needle Knife Fistulotomy as a Rescue Procedure in Patients with Pancreaticobiliary Disease. Korean J Gastroenterol. 2020;75(6):341-346.
- Ito K, Fujita N, Noda Y, Kobayashi G, Obana T, Horaguchi J, et al. Pancreatic guidewire placement for achieving selective biliary cannulation during endoscopic retrograde cholangio-pancreatography. World J Gastroenterol. 2008;14(36):5595-600; discussion 5599.
- Angsuwatcharakon P, Rerknimitr R, Ridtitid W, Ponauthai Y, Kullavanijaya P. Success rate and cannulation time between precut sphincterotomy and double-guidewire technique in truly difficult biliary cannulation. J Gastroenterol Hepatol. 2012;27(2): 356-61.
- Coté GA, Mullady DK, Jonnalagadda SS, Keswani RN, Wani SB, Hovis CE, et al. Use of a pancreatic duct stent or guidewire facilitates bile duct access with low rates of precut sphincterotomy: a randomized clinical trial. Dig Dis Sci. 2012;57(12):3271-8.
- Zou X, Leung J, Li Y, Yao Y, Pei Q, Wu Y, et al. Comparison of sequential pancreatic duct guidewire placement technique and needle knife precut sphincterotomy for difficult biliary cannulation. J Dig Dis. 2015;16(12):741-6.
- Fontana RJ, Hayashi P, Bonkovsky HL, Kleiner DE, Kochhar S, Gu J, and Ghabril M. Presentation and outcomes with clinically apparent interferon beta hepatotoxicity. Dig Dis Sci. 2013;58(6):1766-75.
- Schipf S, Knüppel S, Hardt J, Stang A. Directed acyclic graphs (DAGs) - the application of causal diagrams in epidemiology. Gesundheitswesen. 2011;73(12):888-92. German
- Recchia S, Coppola F, Ferrari A, Righi D, Zanon E, Verme G. Fistulosphincterotomy in the endoscopic approach to biliary tract diseases. Am J Gastroenterol. 1992;87(11):1607-9.
- Guzmán-Calderón E, Vera A, Díaz R, Alva E, Arcana R. Efficacy and complications of double guidewire technique in biliary tract cannulation. Rev Gastroenterol Peru. 2017;37(3):235-239. Spanish
Full Text Sources:
Abstract:
Views: 3190

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.