Surgery, Gastroenterology and Oncology

|
|
Aim of the study: Managing wound closure in complicated appendicitis presents major challenges. This quasi-experimental study, employing propensity score matching, aimed to evaluate the effectiveness of primary closure compared with delayed primary closure for preventing surgical site infections (SSIs) in complicated appendicitis.
Methods: Patients with complicated appendicitis undergoing open appendectomy were selected using a quasi-experimental design. Propensity score matching minimized confounding factors, and comparative statistical analyses, including chi-square tests, were conducted to determine significant differences in SSI rates.
Results: Among 42 patients, primary closure resulted in an SSI rate of 2.38%, comparable to delayed primary closure. Propensity score matching balanced patient characteristics, strengthening the study’s validity.
Conclusion: Primary closure may be a viable option in complicated appendicitis with adequate infection control. However, research with larger samples is needed to confirm this finding.
INTRODUCTION
Complicated appendicitis, characterized by perforation, abscess, or gangrene, poses substantial challenges in surgical management, particularly regarding wound closure techniques (1). Traditionally, delayed primary wound closure (DPC) has been recommended in cases involving infection or contamination, aiming to minimize the risk of surgical site infections (SSIs) by allowing wound drainage and partial healing before final closure (2). Although effective in lowering SSIs, DPC often results in extended hospital stays, slower wound healing, and increased patient discomfort. This has spurred interest in alternative approaches, such as primary wound closure (PWC), to enhance recovery and patient outcomes.
PWC, involving immediate suturing of the incision following appendectomy, has demonstrated favorable results in uncomplicated appendicitis, including low SSI rates, improved cosmetic outcomes, and faster recovery. However its efficacy in complicated appendicitis remains uncertain owing to concerns regarding infection risks in a contaminated surgical field. However, prior studies have shown that, with appropriate infection control measures, primary closure may yield SSI rates comparable to delayed closure, challenging traditional views on delayed closure’s superiority.
The shift toward evaluating primary closure in complicated cases has been supported by evidence from randomized controlled trials and systematic reviews. These studies indicate that factors such as effective perioperative antibiotic use and adherence to aseptic techniques may allow primary closure to achieve similar outcomes to delayed closure. For example, previous meta-analyses suggest that SSI risk may depend more on antibiotic protocols, patient comorbidities, and surgeon expertise rather than on wound closure timing itself (3).
However, inconsistencies in patient selection criteria and control of confounding variables in the literature limit the reliability of existing findings. In complicated appendicitis, factors including age, sex, comorbidities, and perioperative management markedly influence SSI outcomes. To address these gaps, this study employs a quasi-experimental design with propensity score matching to control for confounding variables and provide a more precise comparison of primary and delayed wound closure in complicated appendicitis.
By matching patients with similar baseline characteristics, this study aims to determine whether primary closure is a viable option in complicated appendicitis without increasing SSI risk. The findings will contribute to a more nuanced understanding of wound closure techniques in contaminated surgical fields. Ultimately, this research seeks to inform clinical decision-making by assessing whether primary closure can safely be used in high-risk cases, potentially improving recovery and optimizing hospital resource use.
MATERIALS AND METHODS
Study Design
This quasi-experimental, retrospective analysis compared PWC and DPC in complicated appendicitis. Propensity score matching was employed to minimize confounding biases due to patients’ different baseline characteristics, creating comparable groups based on key demographic and clinical variables.
Setting and Duration
The study was conducted at the Department of Surgery, Faculty of Medicine, Vajira Hospital, Navamindrahiraj University, Bangkok, Thailand, covering cases between January 2020 and December 2023.
Population and Sample Size
The medical records of 87 patients diagnosed with complicated appendicitis and treated via open appendectomy at Vajira Hospital were initially reviewed. After applying inclusion and exclusion criteria (described below), 42 patients were included in the final analysis. Sample size determination was based on power analysis to detect significant differences in SSI rates between groups, although the sample size limitation is acknowledged as a potential study constraint.
Inclusion and Exclusion Criteria
Inclusion criteria: Patients aged 18 years or older diagnosed with complicated appendicitis, defined as appendicitis with perforation, abscess formation, or gangrene, who underwent open appendectomy with either PWC or DPC.
Exclusion criteria: Patients with prior abdominal surgery within 3 months, generalized peritonitis, immune-compromised status (e.g., HIV-positive or receiving long-term immunosuppressive therapy), and/or insufficient medical records or follow-up data.
Propensity Score Matching
To control for confounding, propensity scores were calculated for each patient using demographic and clinical characteristics, including age, sex, body mass index (BMI), comorbidities (e.g., diabetes or hypertension), and white blood cell count at admission. Nearest-neighbor matching with a caliper of 0.2 was performed at a 1:1 ratio between PWC and DPC cases, resulting in balanced groups with similar baseline characteristics.
Data Collection
Data were extracted from electronic medical records and surgical reports, including the following variables:
- Demographic data: age, sex, BMI, and comorbidities.
- Clinical and perioperative data: White blood cell count, diagnosis of ruptured or gangrenous appendicitis, prophylactic antibiotic use, operative time, estimated blood loss, and post-operative care
protocols.
Outcome measures: SSI rates (categorized as superficial or deep SSI, based on Centers for Disease Control and Prevention criteria), wound seroma formation, postoperative hospital stay, and need for reoperation or additional interventions. Follow-up data were collected at out-patient visits on postoperative days 7, 30, and 90.
Surgical Protocol
All patients underwent open appendectomy followed standardized protocols, involving the following steps:
- Incision and exposure: a McBurney or lower midline incision was used based on infection extent and surgeon discretion.
- Appendectomy procedure: the appendix was excised under aseptic conditions, with thorough irrigation using sterile saline for cases involving pus or abscess.
- Wound management: in the PWC group, wounds were closed immediately using nonabsorbable sutures, and drains were selectively placed based on intraoperative findings. In the DPC group, wounds were left open initially and closed 3-5 days postoperatively if infection or substantial drainage was absent.
- Antibiotic regimen: all patients received prophylactic intravenous antibiotics, typically a second-generation cephalosporin and metronidazole, beginning preoperatively and continuing post-operatively, as per hospital guidelines.
Statistical Analysis
Descriptive statistics were calculated for baseline characteristics and outcomes. Continuous variables were reported as means ± standard deviations or medians (with ranges) and analyzed using t-tests or Mann-Whitney U tests based on data distribution. Categorical variables, expressed as frequencies and percentages, were analyzed using chi-square or Fisher’s exact tests as appropriate. Statistical significance was set at p <0.05.
Ethical Considerations
This study was approved by the Ethics Committee of Vajira Hospital, with informed consent waived owing to its retrospective design. Patient data confidentiality was maintained, with data access restricted to authorized personnel.
RESULTS
Patient Characteristics
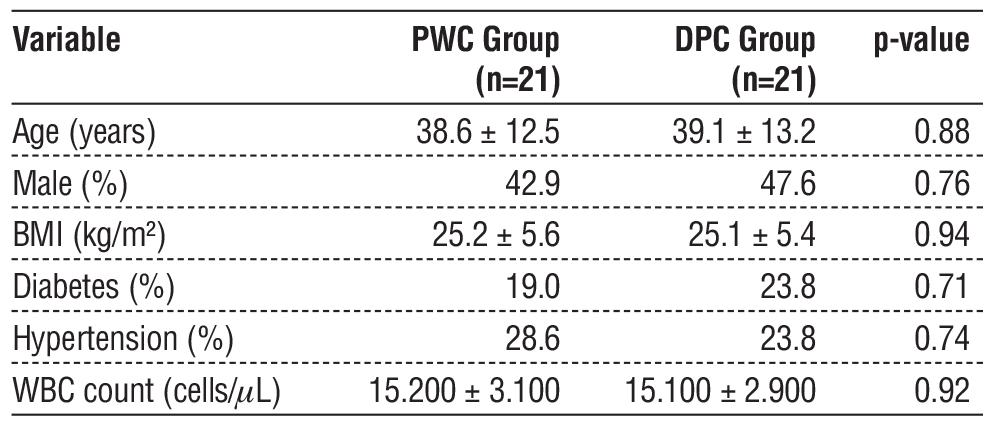
After propensity score matching, 42 patients with complicated appendicitis were analyzed, with 21 patients each in the PWC and DPC groups. Baseline characteristics were well-matched, showing no significant differences in age, sex, BMI, comorbidities (e.g., diabetes or hypertension), or white blood cell count between groups. Table 1 summarizes the demographic and clinical characteristics of each group.
Table 1 - Baseline characteristics of patients (Matched Groups)
Surgical Outcomes
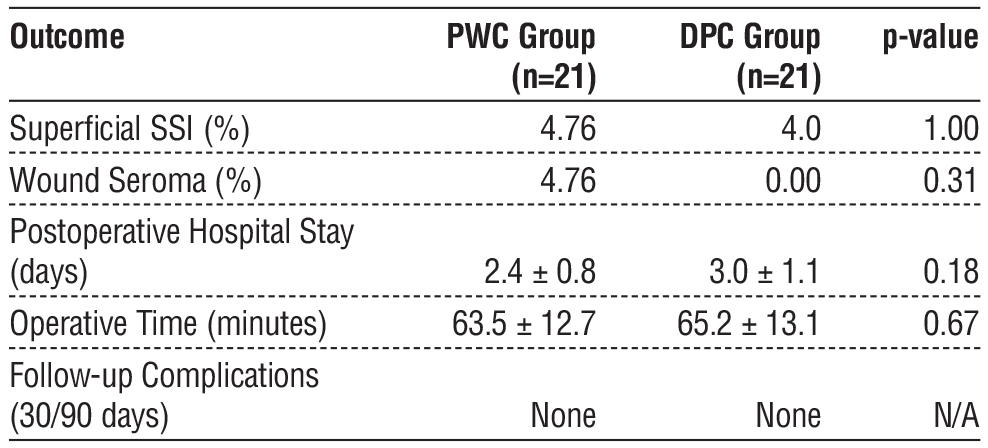
The primary outcome, SSI, was comparable between the two groups. One superficial SSI case each occurred in the PWC (4.76%) and DPC (4.0%) groups. Both cases were managed with wound cleansing and antibiotics, without requiring reoperation. Wound seroma formation was reported in one PWC group (4.76%), which was successfully treated with aspiration and localized wound care. Neither deep SSIs nor intra-abdominal abscesses were observed in either group.
Secondary outcomes included postoperative hospital stay, operative time, and follow-up outcomes. Median hospital stays were 2 days (range: 1-5 days) and 3 days (range: 2-6 days) for the PWC and DPC groups, respectively, with no significant difference observed (p = 0.18). Mean operative times were 63.5 ± 12.7 and 65.2 ± 13.1 min for the PWC and DPC groups, respectively, which were not significantly different (p = 0.67). Follow-up at 30 and 90 days revealed no additional wound complications or SSIs, indicating stable recovery in both groups (table 2).
Table 2 - Comparative outcomes between PWC and DPC groups
The comparison of SSI rates between the PWC and DPC groups revealed a risk ratio of 1.19, indicating a nonsignificant increase in SSI risk in the PWC group. The risk difference was 0.76%, reflecting a nonsignificant difference in SSI rates. Confidence intervals were wide owing to the small sample size, with 95% confidence intervals of 0.08-16.94 and -4.72%-6.24% for risk ratio and risk difference, respectively (table 3).
Table 3 - SSI rates, risk ratio, and risk difference with 95% CI

These findings suggest that PWC does not significantly elevate the SSI risk compared with DPC in complicated appendicitis. However, the wide confidence intervals for both risk ratio and risk difference highlight the need for further research with larger sample sizes to validate these results.
Discussion
In this study, the infection rate following PWC in complicated appendicitis cases was 2.38%, a low and acceptable rate. This suggests that PWC is a viable option in complicated appendicitis, challenging the traditional preference for DPC. Factors influencing the choice between PWC and DPC in cases involving perforated or gangrenous appendicitis include the extent of infection, wound condition, and patient overall clinical status.
Historically, DPC has been favored in contaminated or infected wounds, as it allows drainage and reduces infection risk before final closure. Studies dating back to the 1960s, such as that by Grosfeld and Solit, (4) supported DPC use for contaminated wounds, emphasizing its role in infection control and improved healing outcomes. However, DPC has notable limitations, including prolonged hospital stays, delayed wound healing, and patient discomfort due to extended open wound management (4,5).
In uncomplicated appendicitis, PWC has long been the standard approach, offering benefits such as improved cosmetic results, shorter hospital stays, faster recovery, and reduced infection risk through early closure. PWC involves immediate surgical incision closure after appendectomy and is typically preferred in cases without perforation or abscess formation. The main concern with PWC in complicated appendicitis is the risk of wound complications, such as infection or wound breakdown, if contamination persists.
Additionally, inadequate drainage during surgery may increase the risk of intra-abdominal abscess formation (6). To mitigate these risks, surgeons may use drains in PWC settings to manage residual infection or abscesses (7).
Studies by Duttaroy et al. (8) and Siribumrungwong et al. (9) compared superficial SSI rates between DPC and PWC in complicated appendicitis. Both found that PWC did not lead to significantly higher SSI rates compared with DPC. Duttaroy et al. (8) conducted a randomized trial evaluating wound management strategies in contaminated abdominal incisions, finding comparable infection rates between closure methods. Similarly, Siribumrungwong et al. (9,10) performed a randomized controlled trial, as well as a meta-analysis, concluding that with proper infection control, PWC is a viable option in complicated appendicitis, yielding similar outcomes to DPC. These findings collectively support the safety and efficacy of PWC in contaminated fields without increasing SSI risks.
Ultimately, the decision between PWC and DPC in complicated appendicitis should rely on the surgeon’s clinical judgment, considering the patient’s condition, infection severity, and other complicating factors. Effective infection control and optimal wound healing remain the primary goals. With appropriate infection management and patient selection, PWC may serve as a safe alternative, even in high-risk cases.
CONCLUSION
This study demonstrates that, in complicated appendicitis cases at Vajira Hospital, PWC did not result in a significantly higher wound infection rate compared with DPC. These findings challenge the traditional preference for DPC in contaminated surgical wounds, suggesting that PWC can be safely implemented in selected cases of complicated appendicitis. However, decisions on wound closure techniques should be individualized, factoring in patient characteristics, surgeon expertise, and specific clinical circumstances. Further research, particularly prospective studies and multicenter trials, is necessary to validate these findings and guide the development of comprehensive guidelines for managing wound closure in complicated appendicitis.
Author’s Contributions
TK, ST: Equally contributed to all aspects of the research, including conceptualization, methodology, data collection, data analysis, manuscript writing, and final approval of the manuscript.
Acknowledgments
The authors sincerely thank the patients, their families, and the Vajira Scientific Editing Center,
Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, for their support in facilitating the publication process.
Conflicts of Interest
The authors declare no conflicts of interest relevant to this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-
for-profit sectors. However, language editing support was provided by the Vajira Scientific Editing Center, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University.
REFERENCES
1. Mariage M, Sabbagh C, Grelpois G, Prevot F, Darmon I, Regimbeau JM. Surgeon's Definition of Complicated Appendicitis: A Prospective Video Survey Study. Euroasian J Hepatogastroenterol. 2019;9(1):1-4.
2. De Simone B, Sartelli M, Coccolini F, Ball CG, Brambillasca P, Chiarugi M, et al. Intraoperative surgical site infection control and prevention: a position paper and future addendum to WSES intra-abdominal infections guidelines. World J Emerg Surg. 2020;15(1):10.
3. Hureibi K, Abraham P, Al-Sunidar O, Alaraimi B, Elzaidi E. To close or not to close? A systematic review and meta-analysis of wound closure in appendicectomy. International Journal of Surgery Open. 2019;16:9-13.
4. Grosfeld JL, Solit RW. Prevention of wound infection in perforated appendicitis: experience with delayed primary wound closure. Ann Surg. 1968;168(5):891-5.
5. ElHawary H, Covone J, Abdulkarim S, Janis JE. Practical Review on Delayed Primary Closure: Basic Science and Clinical Applications. Plast Reconstr Surg Glob Open. 2023;11(8):e5172.
6. Khan KI, Mahmood S, Akmal M, Waqas A. Comparison of rate of surgical wound infection, length of hospital stay and patient convenience in complicated appendicitis between primary closure and delayed primary closure. J Pak Med Assoc. 2012;62(6):596-8.
7. Mehrabi Bahar M, Jangjoo A, Amouzeshi A, Kavianifar K. Wound infection incidence in patients with simple and gangrenous or perforated appendicitis. Arch Iran Med. 2010;13(1):13-6.
8. Duttaroy DD, Jitendra J, Duttaroy B, Bansal U, Dhameja P, Patel G, et al. Management strategy for dirty abdominal incisions: primary or delayed primary closure? A randomized trial. Surg Infect (Larchmt). 2009;10(2):129-36.
9. Siribumrungwong B, Chantip A, Noorit P, Wilasrusmee C, Ungpinitpong W, Chotiya P, et al. Comparison of Superficial Surgical Site Infection Between Delayed Primary Versus Primary Wound Closure in Complicated Appendicitis: A Randomized Controlled Trial. Ann Surg. 2018;267(4):631-7.
10. Siribumrungwong B, Noorit P, Wilasrusmee C, Thakkinstian A. A systematic review and meta-analysis of randomised controlled trials of delayed primary wound closure in contaminated abdominal wounds. World J Emerg Surg. 2014;9(1):49.
Full Text Sources:
Abstract:
Views: 3044

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.