Surgery, Gastroenterology and Oncology

|
|
Background: Pancreatic cysts are common and difficult to diagnose. CT scan is the best
radiology tool for evaluating pancreatic cysts. The study aimed to differentiate whether
pancreatic injuries are benign or malignant.
Methods: A prospective research with a total of fifty-eight cases from June 2021 to May 2022. Data collected including age, gender, symptoms, and CT scan findings. All cases underwent for CT scan examination.
Results: Most masses were homogeneous in 77.6% in content. About 74.1% of cases have thin walls. Cystic solid components in malignant cyst more than benign cyst. Types of cysts in the benign tumor were detected differently from malignant tumor.
Conclusions: MDCT scan is the easily applicable non-invasive tool of choice for the determination of cystic lesions of the pancreas. Solid components and types of cysts could be positively implicated in CT scan results.
Introduction
Pancreas cysts are commonest and raise challenge delimae of difficulty to the detection, because the quality of radiology techniques improves the detection of asymptomatic pancreatic cysts is increase (1). The commonly detected lesions are serous cystadenomas, pseudocysts, mucinous cystic neoplasms (MCN), intraductal papillary mucinous neoplasms (IPMN), and solid pseudopapillary tumors. Almost all cysts may be pseudocysts, and all cysts are required to be diagnosed to prove whether they are malignant or pre malignant (2). Recently, there have been no gold standard radiological tools for differentia tion (3). CT scan (4), PET scan (5), MR cholangio pancreatography, endoscopic EUSFNA (6), ERCP and tumor markers (2) have been utilized to diagnose cysts which are demonstrated different degrees of sensitive and specific pattern (3).
These lesions are grouped into neoplastic and non neoplastic. Neoplastic tumors can transforming into malignant ones. The pseudocysts, lympho epithelial cyst, and retention cyst are never trans formed into malignant. A percentage of diagnosed cyst has varies, ranging (0.7 36.7%) (7).
Early diagnosis of the cysts raised the dilemma of how to triage and treat cystic lesions (8).
Recently, a CT scan is the best radiology tool for the initial evaluation and follow-up of cyst (9,10). Advantageous properties are the high speed of acquisition with narrow collimations, big images resolution, multi planar imaging, and reformats using volumes
data (11). Additionally, CT is widely available, easily accessible, less costly, highly sensitive, highly accurately, reproducible, and easy to read (11).
The non neoplastic cysts are pseudocysts, retention cysts, cystic pancreatic lymphangioma, dermoid cysts (Epidermoid), and duplication cysts (Ciliated foregut). The neoplastic cysts (PANCREATIC CYSTIC NEOPLASMS) are Mucinous cystic lesions (Intra ductal papillary muci nous neoplasm (IPMNs), Mucinous cystic neoplasm (MCNs)), and Nonmucinous Cystic Neoplastic Lesions, Serous cystic neoplasm (SCNs), Solid pseudopapillary neoplasm (SPNs), cystic pancreatic neuroendocrine tumor, and Cystic acinar cell neoplasm. Others are Pancreatic ductal adenocarcinoma with cystic degener ation, and Intra ductal tubule papillary neoplasm (ITPN) (12).
Aims of the study to differentiate whether pancreatic lesions are malignant or non malignant.
Methods
Study Design and Setting
A prospective work with a total of fifty-eight patients with dorsal abdominal pain radiating to the anterior were enrolled in the study during the period from 12th June 2021 to 20th May 2022. The sample consisted of 19 (32.8%) male and 39(67.2%) female, their median age, of 42 years (mean= 41.59±11.9 years).
Data Collection
Participants' data including age, sex, and symptoms, and CT scan findings include: lesion sites, parenchymal atrophy, number of cystic lesions, diameter of largest cyst, calcification, ductal dilation, solid components, cyst contour, enhancement, cyst types, thick wall, lymphovascular invasion and communication cyst-duct.
Exclusion Criteria
1. Pregnant women
2. Allergy to contrast.
3. Unwilling.
4. Renal disorder.
Protocols
CT scan was performed utilizing the Siemens system (SOMATOM Definition AS VA44A; Siemens, Somaris/7 syngo CT 67002 2012B, Germany) and 64 slice multi detector) CT system (Philips).
Ethical Approval
The study was approved by The Medical Ethical Committee of the College of Medicine, Babylon University.
Statistical Analysis
A SPSS version 24.0, Chicago: SPSS, Inc. was used. Findings were described into frequencies and percents for nominal and (mean, and SD) calculations for ordinal. Pearson’s test was used. A one sided P <0.05 was considered statistically significant.
Results
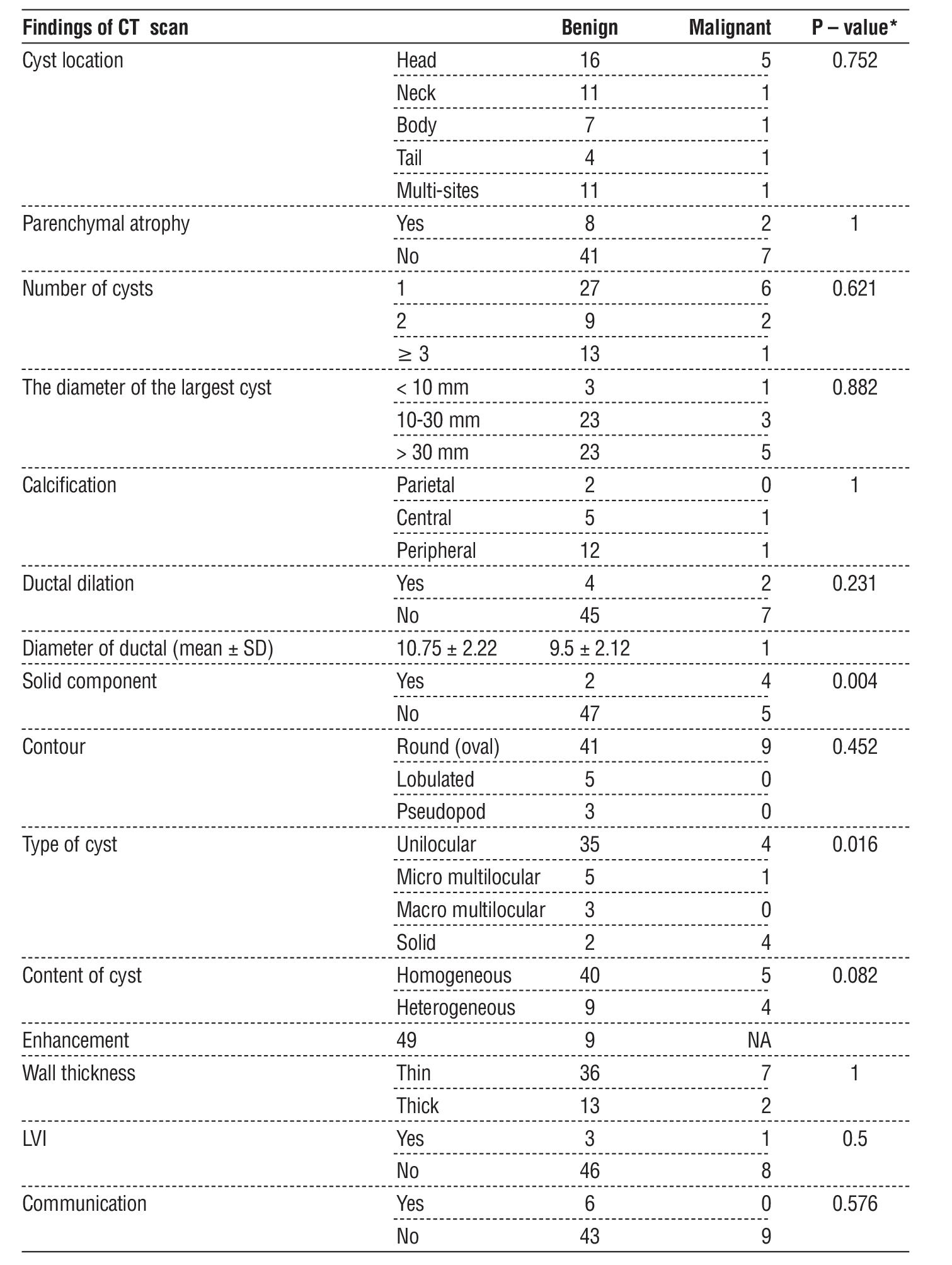
CT scan findings in non malignant and malignant cysts are listed in table 1. All pancreatic cysts features were insignificant between benign and malignant tumors. Additionally, solid components of cysts showed a statistically significant difference in malignant pancreatic cysts more than benign cysts (P= 0.004). Furthermore, types of cysts in benign pancreatic tumors were investigated significantly differently from malignant tumors (P= 0.016) (table 1).
Table 1 - CT scan findings in benign and malignant lesions.
Discussion
In correlation between benign and malignant in this study, the data showed that most pancreatic cyst features were differed insignificantly (P > 0.05). Additionally, solid components of cysts showed a statistically significant difference in malignant lesions more than benign lesions (P = 0.004). Furthermore, types in benign pancreatic tumors were detected significantly differently from malignant tumors (P = 0.016). Crippa et al. reported that MCNs documented 25% of all cystic malignancies and IPMNs were 50% (13). Another studies of 851 patients showed that IPMNs assumed for 38% of cysts, MCNs for 23%, SCNs for 16%, and solid pseudopapillary tumors for 3% (14). This misguidance can be diminished with a multi disciplinary team approach to study these cysts with the incorpora tion of the clinical, radiologic, and pathologic findings before reaching a definite diagnosis (15).
Multi detector CT (MDCT) improves spatial and temporal resolution and significant impact on the ability to assess a cyst's variety of pancreas with raised accuracy and sophistication (16). Cystic pancreatic tumors do have radiology findings that may permit them to provide a specific and accurate diagnosis or, to narrow the differential diagnosis. Moreover, CT scans now serve as the primary tool to risk stratify cysts and determine which lesions can be safely treated conservatively plus follow up (17). The prevalence ranged from 1.2% (18) to 2.6 % (19).
Recently in modern CT scans, images are taken with an extremely thin collimation plus a slice thickness of only 0.625 to 0.75 mm, then reconstructed into 3 to 5 mm axial sections (16, 20). 3 D reconstruction recently has now proven technique for the diagnosis of cyst lesions with two most commonly utilized include: (1) maximum intensity projection (MIP) imaging and (2) volume rendering (VR).
Raman and Fishman found this technique to be very helpful for cysts determination, assessment of the internal architecture of cysts, and demonstrating the association of a cyst to the neighboring duct (16).
Several researches in the past have shown MDCT to be very accurate in the characterization of cysts, with accuracy was 56% to 85%, with accuracies as high as 79% for distinguishing benign from malignant cysts and as high as 85% for distinguishing mucinous type and non mucinous types (21,22).
Optimal photos of cysts require helical (spiral) CT or multi detector CT (MDCT), in addition to rapid adminis tration of IV contrast. The helical scanning, axial images 5 mm collimation, 7 mm collimation, pitch 1.5 over the upper abdomen, and pitch 2 for the rest of the abdomen can be obtained. Acquisition starts from the top of the diaphragm at approximately 60 sec. The MDCT scanner acquired a two phase acquisition technique that can be employed (20) which are arterial dominant phase, portal dominant phase, and
dual phase pancreatic imaging.
Conclusions
MDCT scan is the easily non invasive applicable tool for the evaluation of pancreatic cysts. Detection of site and number of cyst, dilation of duct, solid components, and types are helpful in differentiating among malignant and benign lesions. Solid components of cyst and types of cyst could be positively implicated malignant lesions.
Conflicts of Interest
The authors declare no conflict of interest regarding this article.
Funding
None.
References
1. Katz DS, Friedel DM, Kho D, Georgiou N, Hines JJ. Relative accuracy of CT and MRI for characterization of cystic pancreatic masses. AJR Am J Roentgenol 2007;189:657e61.
2. Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology 2004;126:1330e6.
3. Jones MJ, Buchanan AS, Neal CP, Dennison AR, Metcalfe MS, Garcea G. Imaging of indeterminate pancreatic cystic lesions: a systematic review. Pancreatology. 2013;13(4):436-42.
4. Le Borgne J, de Calan L, Partensky C. Cystadenomas and cystadenocarcinomas of the pancreas: a multiinstitutional retrospective study of 398 cases. French surgical association. Ann Surg 1999;230:152e61.
5. Kalra MK, Maher MM, Mueller PR, Saini S. State-of-the-art imaging of pancreatic neoplasms. Br J Radiol 2003;76:857e65.
6. Thosani N, Thosani S, Qiao W, Fleming JB, Bhutani MS, Guha S. Role of EUSFNA- based cytology in the diagnosis of mucinous
pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010;55:2756e66.
7. Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A, Komorowski RA, et al. Cystic pancreatic neoplasms: observe or operate. Ann Surg. 2004;239(5):651-7; discussion 657-9.
8. Karoumpalis I, Christodoulou DK. Cystic lesions of the pancreas. Ann Gastroenterol. 2016;29(2):155-161.
9. Thoeni RF. Imaging of Acute Pancreatitis. Radiol Clin North Am. 2015;53:1189-1208.
10. Bollen TL. Acute pancreatitis: international classification and nomenclature. Clin Radiol. 2016;71:121-133.
11. Bollen TL. Pancreatitis: Imaging assessment of etiology and severity of acute pancreatitis. In: Williams JA, Pandol SJ, Lerch MM, et al, (editors). American Pancreatic Association. Michigan Publishing, US. 2016; p. 226-8.
12. Adsay NV. Cystic lesions of the pancreas. Mod Pathol. 2007; 20(suppl 1):S71–S93.
13. Crippa S, Salvia R, Warshaw AL, Domínguez I, Bassi C, Falconi M, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg. 2008;247(4): 571-9.
14. Jais B, Rebours V, Malleo G, Salvia R, Fontana M, Maggino L, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut. 2016;65(2):305-12.
15. Pongpornsup S, Piyapittayanan S, Charoensak A. MDCT imaging findings for characterization pancreatic cystic lesion: differentiation between benign and malignant pattern. J Med Assoc Thai. 2011; 94(3):369-78.
16. Raman SP, Fishman EK. Multidetector Computed Tomography in the Evaluation of Cystic Tumors of the Pancreas. In : M. Del Chiaro et al. (eds.), Cystic Tumors of the Pancreas. Springer International Publishing Switzerland. 2016; p. 51-60.
17. Visser BC, Yeh BM, Qayyum A, Way LW, McCulloch CE, Coakley FV. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. AJR Am J Roentgenol. 2007;189:648–56.
18. Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A, Komorowski RA, et al. Cystic pancreatic neoplasms: observe or operate. Ann Surg. 2004;239(5):651–7. discussion 657–9.
19. Laffan TA, Horton KM, Klein AP, Berlanstein B, Siegelman SS, Kawamoto S, et al. Prevalence of unsuspected pancreatic cysts on MDCT. AJR Am J Roentgenol. 2008;191(3):802–7.
20. Balthazar EJ, Megibow AJ, Pozzi Mucelli R. Imaging of the Pancreas: Acute and Chronic pancreatitis. In : Baert ALL, Knauth MG, Sartor KH (edts). Medical Radiology, Diagnostic Imaging and Radiation Oncology. Springer-Verlag Berlin Heidelberg, NY, US. 2009; p. 54-59.
21. Sahani DV, Kambadakone A, Macari M, Takahashi N, Chari S, Fernandez-del Castillo C. Diagnosis and management of cystic pancreatic lesions. AJR Am J Roentgenol. 2013;200:343–54.
22. Chaudhari VV, Raman SS, Vuong NL, Zimmerman P, Farrell J, Reber H, et al. Pancreatic cystic lesions: discrimination accuracy based on clinical data and high-resolution computed tomographic features. J Comput Assist Tomogr. 2008;32(5):757-63.
Full Text Sources:
Abstract:
Views: 1692

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.