Surgery, Gastroenterology and Oncology

|
|
Introduction: Uterine artery embolization (UAE) is a minimally invasive interventional technique that has found increasingly widespread application in modern obstetric and gynecological practice. Initially introduced for the management of postpartum hemorrhage, the procedure has gradually established its role in the treatment of gynecological conditions such as uterine fibroids, adenomyosis, arteriovenous malformations, and ectopic pregnancy. Objective: This review aims to present the current indications, contraindications, efficacy, and limitations of UAE in both emergency and elective clinical settings. Special emphasis is placed on its comparison with alternative therapeutic approaches, the assessment of its impact on fertility, and its role in gynecologic oncology.
Methods: A systematic review of the current literature was conducted, encompassing clinical studies, meta-analyses, and guidelines from professional organizations related to the use of UAE in obstetrics and gynecology.
Results: UAE demonstrates high clinical efficacy in the treatment of uterine fibroids (85-90%), adenomyosis (up to 80%), arteriovenous malformations (88-95%), and non-tubal ectopic pregnancy (>90%). In cases of postpartum hemorrhage, the procedure achieves hemostasis in over 95% of patients. For malignant tumors, UAE is employed with palliative or preoperative intent. The risk of serious complications remains below 1%.
Conclusion: UAE is a safe and effective therapeutic option with proven benefits in a wide range of obstetric and gynecological conditions. With appropriate patient selection and a multidisciplinary approach, the technique represents a valuable alternative to conventional surgical interventions, particularly in the context of organ-preserving treatment.
INTRODUCTION
In recent decades, minimally invasive techniques have made significant advancements and have found wide application across various fields of medicine. One such method is uterine artery embolization (UAE) - a procedure employed in both gynecology and obstetrics for the control of excessive uterine bleeding. Although originally developed for the treatment of postpartum hemorrhage, current indications for UAE include symptomatic uterine fibroids, arteriovenous malformations, abnormal placentation, and certain forms of ectopic pregnancy.
The method is favored over traditional surgical interventions due to its tissue-sparing nature. In many cases, UAE can replace surgical approaches such as hysterectomy by controlling hemorrhage through the selective occlusion of blood flow to the pathological site. The procedure is associated with symptom relief and reduction in fibroid volume - clinical studies have reported shrinkage of up to 60% from the original size. With technical refinement, the application of UAE has expanded to include conditions such as adenomyosis and vascular anomalies in the pelvis.
Today, UAE is considered by many specialists as an alternative to surgical treatment, offering a shorter recovery period and the potential for uterine preservation. The aim of this review is to present the contemporary role of uterine artery embolization in gynecological and obstetric practice, with emphasis on its indications, contraindications, efficacy, and future prospects.
MATERIAL AND METHOD
We identified a narrative review type of article as the most appropriate for focusing on a broad range of particular questions from different perspectives.
The review and the consensus process were performed between April 2025 and June 2025. A detailed and comprehensive literature search of articles (studies written in English) regarding UAE in different conditions was performed. We conducted a computer-based, extensive review of the following databases: Google Scholar, Cochrane Library, SciELO, and publishers’ databases (Elsevier/ScienceDirect, Wiley, Wolters Klouwer/Lippincott, Taylor & Francis, Springer, Sage, Hindawi, Termedia, and Via Medica). We used the following keywords and Medical Subject Headings (Mesh) terms: “uterine artery embolization”, “fibroids”, “adenomyosis”, “ectopic pregnancy”, “arteriovenous malformation”, “postpartum hemorrhage”, “interventional radiology”, “gynecologic oncology”, “organ-preserving treatment”, “minimally invasive therapy”, and “complications”. References from recent review papers were scanned to identify other related articles. Mainly articles from the 21st century were included. Only a few old articles (dedicated mainly to the history of UAE) were incorporated. The final selection of references was performed after full-text reading. We included all types of articles (original research, systematic reviews, meta-analyses, narrative reviews, and case reports). The majority of the publications had a retrospective nature due to the rarity of the disease. Some studies were repeated because they were considered in different contexts, but we tried not to repeat information in the different subsections of this manuscript.
Historical Development of the Method
The first attempts at vascular embolization in medical practice date back to the 1970s, when the technique was primarily used in cases of traumatic hemorrhage and oncological conditions (1). In 1979, Dr. Jean-Jacques Merland and his team in Paris were the first to successfully employ uterine artery embolization to control postpartum hemorrhage, marking the beginning of its application in obstetric care (2).
During the 1980s, UAE began to be used in gyneco-logical and oncological pathologies associated with bleeding. Clinicians gradually recognized that the method not only provides effective control in emergencies such as postpartum hemorrhage, but also holds potential in other conditions where surgical intervention carries elevated risks or yields unsatisfactory outcomes.
The application of UAE expanded to include hypervascular pelvic tumors, such as cervical and endometrial cancers, as well as benign conditions like adenomyosis and chronic menorrhagia refractory to medical treatment. The method gradually gained recognition for its uterine-sparing potential - an important consideration for women wishing to preserve their reproductive function.
A major milestone in the field occurred in 1995, when French interventional radiologist Dr. Jacques Ravina first applied UAE in patients with uterine fibroids. His observations, published in 2000, demonstrated significant symptom relief and fibroid volume reduction, establishing UAE as a standard therapeutic approach for fibroid disease (2-4).
By 2004, key clinical studies had been published, demonstrating efficacy rates of 85-90% in cases of symptomatic fibroids, with minimal long-term risks (5-6). In 2007, results from multicenter trials confirmed that 80-90% of women who underwent UAE reported substantial improvement in quality of life (7).
Despite these positive outcomes, attention since 2010 has shifted toward the need for more precise definition of the method’s indications and contraindications (8). Advances in embolic materials (e.g., gelatin particles, polyvinyl alcohol) and modern imaging technologies (e.g., reduced radiation exposure during angiography) have further enhanced the safety and efficacy of the procedure (9-11).
According to data from the Society of Interventional Radiology (2012), between 13,000 and 14,000 UAE procedures are performed annually in the United States, confirming the method’s status as a leading alternative to hysterectomy in the treatment of fibroids (12).
Indications and contraindications for uterine artery embolization (UAE)
With the expansion of clinical experience and refinement of technique, the range of indications for UAE has significantly broadened from the late 20th century to the present. Initially used primarily for acute obstetric hemorrhage, the procedure has gradually established itself as an effective treatment for a variety of gynecological conditions characterized by pathological vascularization or symptomatic hypermenorrhea.
Primary indications for UAE
Table 1 summarizes the most common gyneco-logical and obstetric conditions in which UAE is applied with proven efficacy.
Table 1 - Common Indications for UAE.
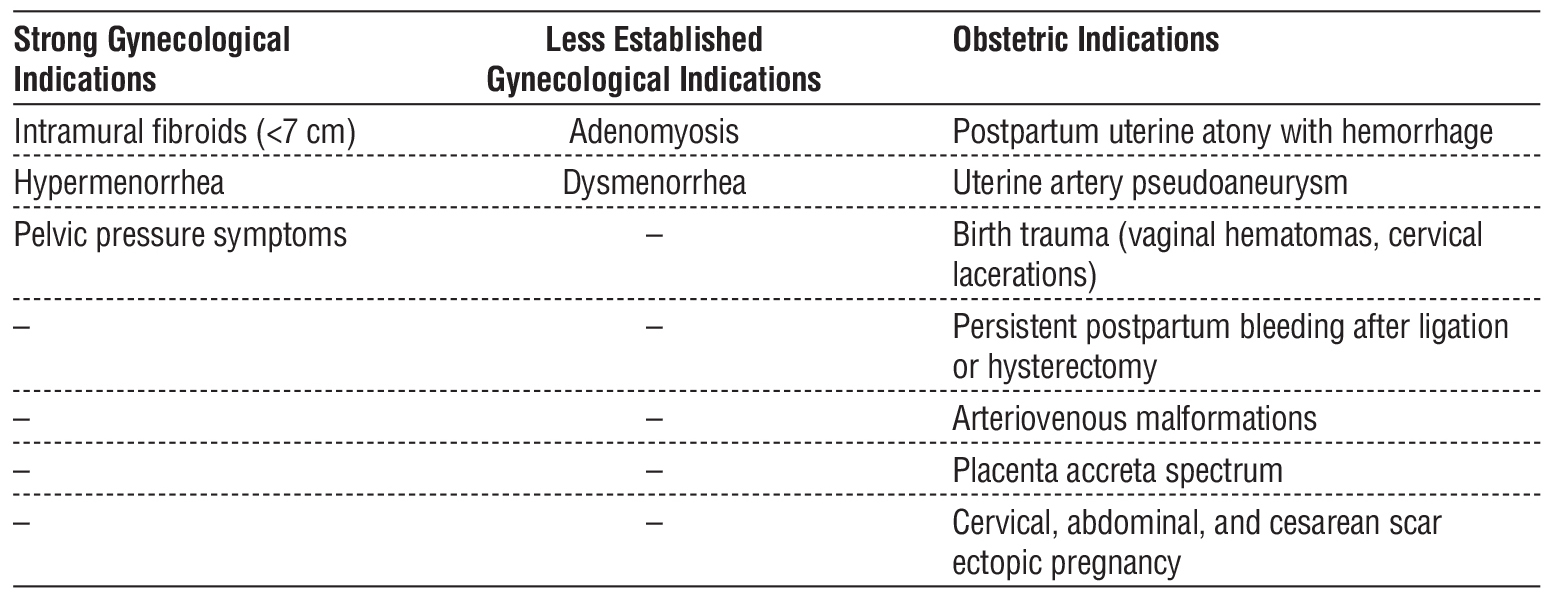
As evident, UAE has broad applications in both gynecological and obstetric practice. It is increasingly considered an alternative to hysterectomy, particularly in patients with a strong desire for uterine preservation or in cases where surgical intervention is contraindicated.
Contraindications for UAE
As with any interventional technique, UAE requires careful patient selection based on the overall clinical context. Contraindications are classified as absolute and relative (table 2).
Table 2 - Contraindications for UAE.
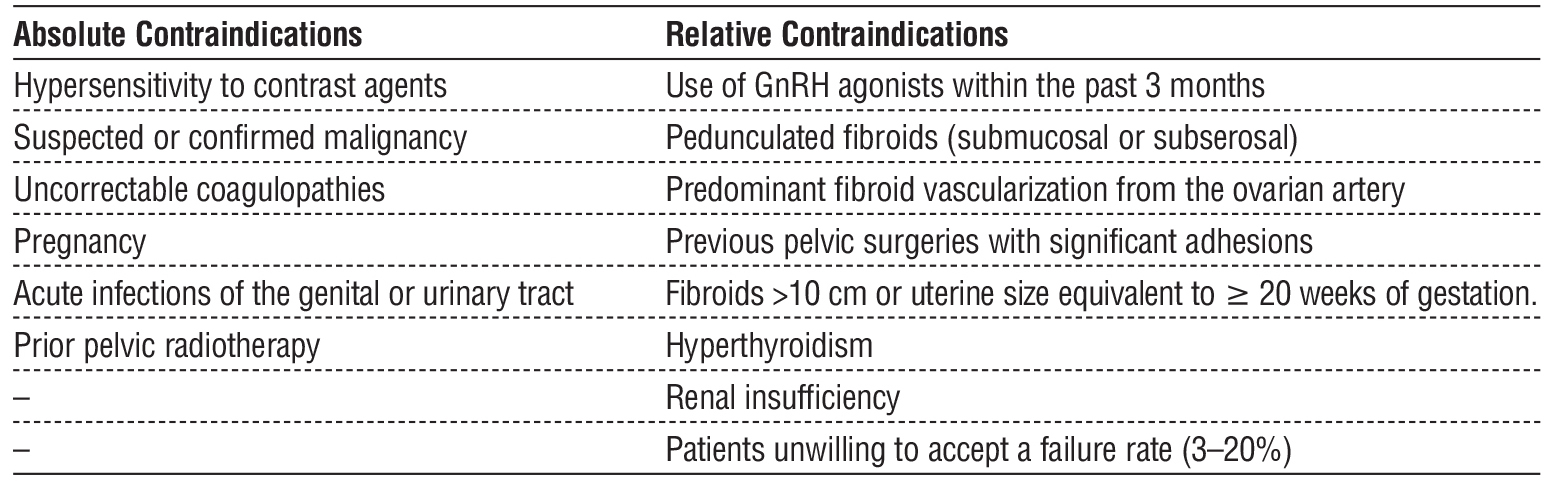
It is essential that the decision to perform UAE is based on an interdisciplinary approach involving both an obstetrician-gynecologist and an interventional radiologist. Individual assessment of risk factors, the clinical characteristics of the lesion, and the patient's reproductive intentions play a key role in the success of the therapy.
Application of Uterine Artery Embolization in Various Gynecological and Obstetric Pathologies
UAE for uterine fibroids
Uterine fibroids are the most common benign tumors in women of reproductive age. UAE has been established as an effective, uterus-preserving approach for managing symptoms related to fibroid disease, particularly in patients seeking to avoid hysterectomy or myomectomy.
Fibroid types suitable for UAE according to the FIGO classification
According to the classification of the International Federation of Gynecology and Obstetrics (FIGO), the following fibroid types are considered suitable for treatment with UAE (16-18):
1) Type 2 (submucosal-intramural): More than 50% of the volume is located within the myometrium; commonly associated with heavy bleeding.
2) Type 3 (intramural, adjacent to the endometrium): Although not in contact with the endometrium, proximity often results in symptoms such as menorrhagia and pain.
3) Type 4 (entirely intramural): The most common type, demonstrating excellent response to UAE when symptomatic.
4) Type 5 (intramural with <50% subserosal component): Typically easy to embolize with favorable outcomes.
5) Type 6 (predominantly subserosal): Suitable for treatment when symptoms include pressure or pain from compression of adjacent structures.
Comparison between UAE and myomectomy
Effectiveness and impact on quality of life
According to systematic reviews and randomized controlled trials, both procedures result in clinically significant symptom relief. However, long-term quality of life is often reported to be higher following myomectomy (19,20).
Recovery time
Studies indicate a shorter hospital stay and recovery period with UAE. The average recovery time is 9.8 days, compared to 25.9 days for myomectomy (21,22).
Complications and need for reintervention
Intraoperative risks are higher with myomectomy, but UAE is associated with a greater likelihood of requiring reintervention. The risk of repeat procedures is 24% after UAE versus 13% after myomectomy (23,24).
Fertility
Available data suggest a higher pregnancy and live birth rate following myomectomy (25,26).
Nevertheless, UAE remains a fertility-sparing option, particularly in carefully selected patients.
Conclusion
Myomectomy is the preferred method for women planning future pregnancies. UAE, on the other hand, offers a minimally invasive alternative for symptomatic fibroids, especially in patients with contraindications to surgery or a strong preference for uterine preservation.
Comparison of UAE with other therapeutic approaches for hypermenorrhea and dysmenorrhea
UAE versus hysterectomy
Hysterectomy is a radical but effective solution for hypermenorrhea. Data from the EMMY trial indicate that 35% of women treated with UAE subsequently require hysterectomy. Nevertheless, quality of life outcomes are similar between the two procedures, with high patient satisfaction reported (78% for UAE versus 87% for hysterectomy) (6,27).
UAE versus laparoscopic uterine artery occlusion
Studies show comparable clinical efficacy between the two techniques in terms of bleeding reduction. Advantages of laparoscopic occlusion include lower pain scores and reduced need for analgesics (28,29). However, UAE provides greater fibroid volume reduction, allows for superselective embolization, and is more suitable for patients with a history of abdominal surgery (30-33).
UAE versus medical treatment
Tranexamic acid achieves up to a 48% reduction in menstrual blood loss (34), though its effect is temporary. UAE offers a durable solution for structural causes of hypermenorrhea, such as fibroid disease or adenomyosis.
UAE for adenomyosis
Adenomyosis is a common cause of dysmenorrhea and menorrhagia. In several studies, over 80% of patients reported significant symptom relief following UAE (35-37). The best outcomes are observed in focal forms of the disease and hypervascular lesions (37,58).
Imaging findings (MRI) show a reduction in uterine volume by 25-55% and a decrease in junctional zone thickness by approximately 30% (59,60). Symptom relief can last up to 27 months (55).
UAE is emerging as a conservative alternative to hysterectomy for selected patients with adenomyosis, particularly those with contraindications to surgery or who refuse operative treatment.
UAE for arteriovenous malformations (AVMs)
Uterine arteriovenous malformations (AVMs) are rare but potentially life-threatening vascular anomalies characterized by direct connections between arteries and veins, lacking a capillary network. While they may be congenital, the majority are acquired-typically resulting from procedures such as curettage, cesarean section, myomectomy, or other invasive interventions (61,62).
Clinical presentation and diagnosis
The most common clinical manifestation of uterine AVM is heavy uterine bleeding, often occurring after surgical procedures. Diagnosis is confirmed via color Doppler ultrasound, MRI, and angiography - the
latter being the gold standard, which also allows for therapeutic intervention.
Role of UAE
Selective embolization is the treatment of choice in hemodynamically stable patients, offering effective bleeding control while preserving the uterus. UAE allows for the use of various embolic agents - PVA particles, gelatin sponges, or glues such as NBCA -depending on the lesion's anatomy and size.
In a systematic review by Labarta et al. (2022), encompassing 95 studies and 371 patients with uterine AVM, UAE demonstrated an overall success rate of 88.4%, with a very low complication rate (1.8%). More than 75% of patients who subsequently conceived had normal pregnancies (66).
UAE for uterine artery pseudoaneurysm (UAP)
Pseudoaneurysm of the uterine artery is a rare but potentially fatal condition characterized by the
formation of a pathological vascular dilation, most often following surgical trauma (cesarean section, myomectomy, curettage). The clinical hallmark is delayed onset of massive bleeding, often without preceding pain (49,50).
Diagnosis is established via color Doppler and CT angiography, though conventional angiography remains the gold standard for definitive diagnosis and treatment.
Embolization as the treatment of choice
Selective UAE provides rapid and effective control of hemorrhage, uterine preservation, and minimal complication risk. Success rates exceed 95% according to multiple studies (49-53). In cases of vascular anastomoses with ovarian vessels, careful angiographic mapping is essential.
UAE for postpartum hemorrhage (PPH)
Postpartum hemorrhage (PPH) remains a leading cause of maternal mortality world-wide, with uterine atony accounting for 70-80% of cases. When medical and mechanical treatments fail, UAE is considered a second-line therapy before resorting to hysterectomy (76-78).
Clinical effectiveness
In a study by Rossetti et al. (2016) involving 73 patients with PPH, UAE was successful in 95.7% of cases, with most women regaining regular menstrual cycles. Similarly, Kim et al. (2020) reported a 99.1%
success rate in 117 cases, with a minimal rate of late complications (81,82).
Indications and limitations
UAE is appropriate for hemodynamically stable patients experiencing continued bleeding despite ineffective medical therapy. Failure may occur in cases of disseminated intravascular coagulation (DIC) or atypical vascular supply. In such scenarios, a more extensive angiographic evaluation is required, including the ovarian and internal pudendal arteries.
UAE for birth trauma
Birth-related injuries, including vaginal hematomas and cervical lacerations, are a common yet often underestimated cause of postpartum hemorrhage. When surgical hemostasis fails, UAE can serve as a life-saving measure (83-85).
Case reports in the literature demonstrate the effectiveness of selective embolization of the vaginal or uterine artery, even in the presence of severe coagulopathy and hypovolemic shock.
UAE for persistent postpartum bleeding after arterial ligation or hysterectomy
In cases of ongoing postpartum bleeding following surgical intervention, residual vessels (e.g., from vaginal, sacral, or ovarian branches) may sustain active hemorrhage. In such scenarios, superselective embolization - even after prior arterial ligation - can successfully control the condition (87-89).
Fernandez et al. (2024) reported 100% efficacy with repeat embolization, with only 6% of patients requiring hysterectomy.
UAE for placenta accreta spectrum (PAS)
Placenta accreta represents a severe form of abnormal placentation, in which chorionic villi invade the myometrium. Traditionally managed by hysterec-tomy, UAE is increasingly being employed as a conservative, uterus-preserving option (90–93).
Indications for UAE in PAS:
i. Postpartum hemorrhage;
ii. Prophylactic UAE in prenatally diagnosed
placenta accreta;
iii. Combination with other techniques: B-Lynch sutures, balloon tamponade, methotrexate.
In a systematic review including 227 patients - 46 of whom had PAS - UAE demonstrated an efficacy rate of 91.3%, with no serious complications reported (92).
UAE for cctopic pregnancy: cervical, cesarean scar, and abdominal pregnancies
Ectopic pregnancy is an acute obstetric condition requiring prompt diagnosis and targeted therapy. Particularly challenging are non-tubal forms - cervical, cesarean scar (isthmocele), and abdominal pregnancies. These locations are associated with a high risk of massive hemorrhage and uterine perforation, and historically, treatment often necessitated hysterectomy.
With the introduction of UAE into obstetric practice in the early 21st century, significant progress has been made in the conservative, uterus-sparing management of these rare but high-risk conditions (70,71).
Clinical Characteristics
Cervical and cesarean scar pregnancies most commonly present with:
- Painless vaginal bleeding;
- Elevated ?-hCG levels.
Ultrasound visualization of a gestational sac in an area with thin or absent myometrium.
Abdominal pregnancy is often undiagnosed until perforation or intraabdominal bleeding occurs. If left untreated, these conditions may lead to severe hemorrhage, rupture, and loss of reproductive potential.
Role of UAE in Ectopic Pregnancy
Selective uterine artery embolization aims to interrupt blood supply to the gestational tissue, thereby minimizing the risk of hemorrhage during subsequent procedures (e.g., medical evacuation or hysteroscopic intervention). The technique is fully compatible with adjunctive medical treatment using methotrexate and can be employed both as a primary and preparatory step in therapy.
Clinical Effectiveness
In a prospective study of 90 patients with cervical and cesarean scar pregnancies, treatment with UAE combined with methotrexate achieved a 100% success rate, with no need for hysterectomy and complete restoration of menstrual cycles in all followed-up women (72).
In a retrospective analysis of 25 cases of non-tubal ectopic pregnancy, the UAE + methotrexate combination yielded a 96% success rate. Among 12 women with reproductive intentions, 10 later conceived successfully (73).
A Chinese meta-analysis covering 37 studies found an average success rate of 93.4% and serious complications in only 1.2% of cases (74).
There is also a documented case of a live birth following a successful series of UAE, hysteroscopy, and laparoscopic scar reconstruction in a cesarean scar pregnancy (75).
Advantages of UAE in Non-tubal Ectopic Pregnancy
Minimally invasive:
• Uterus- and fertility-preserving;
• Controls potentially life-threatening hemorrhage;
• Compatible with medical therapy;
• Suitable even in hemodynamically borderline conditions.
UAE has become established as an effective and conservative method that combines safety with future childbearing potential, particularly in women seeking to preserve reproductive function.
UAE in Gynecologic Malignancies
In gynecologic oncology, uterine artery embolization (UAE) is utilized in four main clinical contexts:
1. Hemorrhage control in tumor bleeding,
2. Palliative treatment in inoperable cases;
3. Preoperative management;
4. Combination with chemotherapy or radiotherapy.
Cervical Cancer
Hemorrhage control in advanced disease
In advanced cervical cancer, one of the most dramatic clinical manifestations is massive vaginal bleeding. UAE is highly effective in acute settings, achieving hemostasis in 95-100% of cases (96-98).
Palliative therapy
In inoperable or terminal stages, embolization is used to:
Alleviate pain
• Control anemia;
• Reduce infectious complications;
• Improve quality of life (97,98).
Superselective embolization
In select cases, targeted embolization of cervico-vaginal branches offers precise control of bleeding from the cervix and vagina (99).
Preoperative chemoembolization
Combining UAE with chemotherapy in locally advanced cancer can:
• Reduce tumor burden;
• Improve resectability;
• Lower intraoperative risks.
In a study of 268 patients, 96% underwent successful surgery following chemoembolization, with an
overall therapeutic response rate exceeding 87% (100).
Endometrial cancer
In advanced or recurrent endometrial cancer, UAE is used palliatively to control difficult-to-manage bleeding. In a study of 33 patients with advanced gynecologic malignancies (31 with cervical and 2 with endometrial cancer), hemostasis was achieved in 100% of cases without serious complications (102).
Other gynecologic malignancies
Although less common, UAE is also applied in:
• Vaginal tumors with hemorrhage;
• Pelvic metastases;
• Postoperative and post-radiation bleeding.
Advantages and considerations
Advantages:
• Rapid control of life-threatening hemorrhage;
• Minimally invasive approach;
• Compatibility with additional treatments (surgery, radiotherapy, chemotherapy);
• Improved quality of life for terminal patients.
Risks:
Although rare some of the risk include:
• Post-embolization syndrome (pain, fever);
• Ischemia of adjacent tissues;
• Temporary effect with resorbable agents.
Available data indicate an exceptionally low rate of serious complications (<1%) (97,103).
CONCLUSION
Uterine artery embolization (UAE) has established itself as an effective, safe, and minimally invasive therapeutic option in modern obstetric and gynecological practice. Initially introduced for the treatment of postpartum hemorrhage, the procedure is now widely applied in gynecological conditions such as fibroids, adenomyosis, arteriovenous malformations, and non-tubal ectopic pregnancies. In gynecologic oncology, UAE provides hemorrhage control and contributes to improved quality of life in advanced disease stages.
The advantages of the procedure include:
• Uterus-preserving approach;
• Short recovery time;
• Potential for fertility preservation;
• Low risk of complications.
The clinical effectiveness of UAE is closely tied to appropriate patient selection, assessment of vascularization, and the involvement of a multidisciplinary team. With the accumulation of scientific evidence and advances in interventional radiology, UAE is increasingly becoming a modern standard in the management of selected obstetric and gyneco-logical pathologies.
Author’s Contributions
Conceptualization, A.Y. and D.S.; methodology, D.S.; formal analysis, E.T.; investigation, D.S.; resources, E.T.; data curation: E.T.; writing-original and draft preparation, D.S.; writing-review and editing, A.Y.; visualization, E.T.; supervision, A.Y. All authors have read and agreed to the published version of the manuscript.
Funding: none.
Conflicts of Interest
The authors declare no conflicts of interest.
Informed Consent Statement: Not applicable.
Data Availability Statement
The authors declare that all related data are available from the corresponding author upon reasonable request.
REFERENCES
1. Goodwin SC, Walker WJ. Uterine artery embolization for the treatment of uterine fibroids. Curr Opin Obstet Gynecol. 1998;10(4): 315-20.
2. Gonsalves C. Uterine artery embolization for treatment of symptomatic fibroids. Semin Intervent Radiol. 2008;25(4):369-377.
3. Ravina JH, Herbreteau D, Ciraru-Vigneron N, Bouret JM, Houdart E, Aymard A, et al. Arterial embolisation to treat uterine myomata. Lancet. 1995 Sep 9;346(8976):671-2.
4. Psilopatis I, Fleckenstein FN, Gebauer B, David M. Medical historical notes on myoma treatment by uterine artery embolization on the occasion of its introduction 30 years ago. Rofo. 2023;195(10):890-895. English, German
5. Pron G, Mocarski E, Bennett J, Vilos G, Common A, Zaidi M, et al. Tolerance, hospital stay, and recovery after uterine artery embolization for fibroids: the Ontario Uterine Fibroid Embolization Trial. J Vasc Interv Radiol. 2003; 14(10):1243-50.
6. Pinto I, Chimeno P, Romo A, Paúl L, Haya J, de la Cal MA, et al. Uterine fibroids: uterine artery embolization versus abdominal hysterectomy for treatment - a prospective, randomized, and controlled clinical trial. Radiology. 2003;226(2):425-31.
7. Hehenkamp WJK, Volkers NA, Donderwinkel PFJ, de Blok S, Birnie E, Ankum WM, et al. Uterine artery embolization versus hysterectomy in the treatment of symptomatic uterine fibroids (EMMY trial): peri- and postprocedural results. Am J Obstet Gynecol. 2005; 193(5):1618-29.
8. Edwards RD, Moss JG, Lumsden MA, Wu O, Murray LS, Twaddle S, et al. Uterine-artery embolization versus surgery for symptomatic uterine fibroids. N Engl J Med. 2007;356(4):360–70.
9. Maclean D, Vigneswaran G, Bryant T, Modi S, Hacking N. A retrospective cohort study comparing a novel, spherical, resorbable particle against five established embolic agents for uterine fibroid embolisation. Clin Radiol. 2021;76(6):452-457.
10. Durrani RJ, Fischman AM, van der Bom IMJ, Kim E, Nowakowski SF, Patel RS, et al. Radiation dose reduction utilizing noise reduction technology during uterine artery embolization: a pilot study. Clin Imaging. 2016;40(3):378-81.
11. Sone M, Arai Y, Shimizu T, Takeuchi Y, Higashihara H, Ohgi S, et al. Phase I/II multiinstitutional study of uterine artery embolization with gelatin sponge for symptomatic uterine leiomyomata: Japan Interventional Radiology in Oncology Study Group study. J Vasc Interv Radiol. 2010;21(11):1665-71.
12. Society of Interventional Radiology (USA) – 2012.
13. Wang X, Zhang W, Xue S, Lasmar RB, Zhao D, Wang X. Efficacy and safety of uterine artery embolization via the distal radial approach for uterine fibroids or adenomyosis: a single-center retrospective cohort study. Gland Surg. 2024;13(5):663-668.
14. Spies JB. Current evidence on uterine embolization for fibroids. Semin Intervent Radiol. 2013;30(4):340-346.
15. McLucas B, Adler L, Perrella R. Uterine fibroid embolization: non-surgical treatment for symptomatic fibroids. J Am Coll Surg. 2001; 192(1):95-105.
16. Munro MG, Critchley HO, Fraser IS; FIGO Menstrual Disorders Working Group. The FIGO classification of causes of abnormal uterine bleeding in the reproductive years. Fertil Steril. 2011;95(7): 2204-2208.e22083.
17. Gomez E, Nguyen MLT, Fursevich D, Macura K, Gupta A. MRI-based pictorial review of the FIGO classification system for uterine fibroids. Abdom Radiol (NY). 2021;46(5):2146-2155.
18. Cappelli A, Mosconi C, Cocozza MA, Brandi N, Bartalena L, Modestino F, et al. Uterine Artery Embolization for the Treatment of Symptomatic Uterine Fibroids of Different Sizes: A Single Center Experience. J Pers Med. 2023;13(6):906.
19. Gaetje R, Mavrova-Risteska L, Zangos S, Karn T, Kissler S, Vogl T, et al. Clinical Outcome after Myomectomy versus Uterine Artery Embolization for Uterine Fibroids. Geburtsh Frauenheilk 2007;67: 748-752.
20. Manyonda I, Belli A, Lumsden M, Moss J, McKinnon W, Middleton L, et al. Uterine-Artery Embolization or Myomectomy for Uterine Fibroids. N Engl J Med. 2020;383(5):440-451.
21. Goodwin SC, Bradley LD, Lipman JC, Stewart EA, Nosher JL, Sterling KM, et al. Uterine artery embolization versus myomectomy: a multicenter comparative study. Fertil Steril. 2006;85(1):14-21.
22. Daniels J, Middleton L, Cheed V, McKinnon W, Rana D, Sirkeci F, et al. Uterine artery embolisation versus myomectomy for premenopausal women with uterine fibroids wishing to avoid hysterectomy: the FEMME RCT. Health Technol Assess. 2022;26(22):1-74.
23. Kaneez F, Haya Waseem A, Arooba E, Furqanullah K, Aimen N, Waqar A, et al. Uterine artery embo-lization versus myomectomy: a systematic review and meta-analysis. SAGE Open Med. 2024; 12:20503121241236141.
24. Daniels J, Middleton L, Cheed V, McKinnon W, Sirkeci F, Manyonda I, et al. Uterine artery embolization or myomectomy for women with uterine fibroids: Four-year follow-up of a randomised controlled trial. Eur J Obstet Gynecol Reprod Biol X. 2021;13:100139.
25. Zanolli N, Bishop K, Kuller J, Price T, Harris B. Fibroids and Fertility: A Comparison of Myomectomy and Uterine Artery Embolization on Fertility and Reproductive Outcomes. Obstet Gynecol Surv. 2022; 77(8):485-494.
26. Middelkoop MA, Harmsen M, Manyonda I, Mára M, Ruuskanen A, Daniels J, et al. Uterine artery embolization versus surgical treatment in patients with symptomatic uterine fibroids: Protocol for a systematic review and meta-analysis of individual participant data. Eur J Obstet Gynecol Reprod Biol. 2021;256:179-183.
27. de Bruijn AD, Ankum W, Reekers J, Birnie E, van der Kooij SM, Volkers NA, et al. Uterine artery embolization vs hysterectomy in the treatment of symptomatic uterine fibroids: 10-year outcomes from the randomized EMMY trial. Am J Obstet Gynecol. 2016;215(6): 745.e1-745.e12.
28. Hald K, Langebrekke A, Kløw NE, Noreng HJ, Bugge Berge A, Istre O. Laparoscopic occlusion of uterine vessels for the treatment of symptomatic fibroids: Initial experience and comparison to uterine artery embolization. Am J Obstet Gynecol. 2004;190(1):37-43.
29. Ambat S, Mittal S, Srivastava DN, Misra R, Dadhwal V, Ghosh B. Uterine artery embolization versus laparoscopic occlusion of uterine vessels for management of symptomatic uterine fibroids. Int J Gynaecol Obstet. 2009;105(2):162-5.
30. Holub Z, Mára M, Kužel D, Jabor A, Maskova J, Eim J. Pregnancy outcomes after uterine artery occlusion: prospective multicentric study. Fertil Steril. 2008;90(5):1886-91.
31. Mára M, Kubinova K, Mašková J, Horak P, Belsan T, Kuzel D. Uterine Artery Embolization Versus Laparoscopic Uterine Artery Occlusion: The Outcomes of a Prospective, Nonrandomized Clinical Trial. Cardiovasc Intervent Radiol. 2012;35(5):1041-52.
32. Hald K, Noreng HJ, Istre O, Kløw N. Uterine artery embolization versus laparoscopic occlusion of uterine arteries for leiomyomas: long-term results of a randomized comparative trial. J Vasc Interv Radiol. 2009;20(10):1303-10. quiz 1311.
33. Dubuisson J, Popescu S, Dubuisson JB, Petignat P. Preventive Uterine Artery Occlusion: Benefits of the Laparoscopic Posterior Approach. J Minim Invasive Gynecol. 2016;23(3):296
34. Cunningham E, Barreda L, Ngo M, Terasaki K, Munro M. Uterine artery embolization versus occlusion for uterine leiomyomas: a pilot randomized clinical trial. J Minim Invasive Gynecol. 2008;15(3):301-7.
301-7.
35. Saiqun G. Clinical Analysis of Uterine Artery Embolization in Treating 62 Cases with Adenomyosis. Medicine. 2007.
36. Kim MD, Kim S, Kim NK, Lee MH, Ahn EH, Kim HJ, et al. Long-term results of uterine artery embolization for symptomatic adenomyosis. AJR Am J Roentgenol. 2007;188(1):176-81.
37. Yang Y-p, Wang W, Feng G-s. The clinical curative effect of super selective uterine artery embolization to ease the dysmenorrhea of adenomyosis. Chinese Journal of Practical Gynecology and Obstetrics, 28 (2012):530-532.
38. Park KH, Kim JY, Shin JS, Kwon JY, Koo JS, Jeong KA, et al. Treatment outcomes of uterine artery embolization and laparoscopic uterine artery ligation for uterine myoma. Yonsei Med J. 2003;44(4): 694-702.
39. Cappelli F, Mosconi C, Facchini C, Rizzo L, Galletti S, Morotti M, et al. Uterine artery embolization for the treatment of symptomatic uterine fibroids of different sizes: A single center experience. J Pers Med. 2023;13(6):906.
40. Hald K, Kløw N, Qvigstad E, Istre O. Laparoscopic occlusion compared with embolization of uterine vessels: a randomized controlled trial. Obstet Gynecol. 2007;109(1):20-7.
41. Ibrahim S, Mansor A. Tranexamic Acid Effect on Doppler Indices of the Uterine Artery in Patients with Menorrhagia Related to Copper IUCD (Cu 380) Insertion. Med. J. Cairo Univ. 2019;87(7):4803-4808.
42. Huo Z, Chen C, Liu P, Ma B, Duan H, Jiang B, et al. Analysis of related factors on effects of uterine artery embolization in the treatment of dysmenorrhea of adenomyosis and the construction and validation of prediction model. Zhonghua Fu Chan Ke Za Zhi. 2016;51(9):650-656. Chinese
43. Hu S, Guo W, Chen SY, Wu Z, Zhuang W, Yang J. Factors associated with dys-menorrhoea and menorrhagia improvement in patients with adenomyosis after uterine artery embolisation. J Obstet Gynaecol. 2024;44(1):2372645.
44. American College of Obstetricians and Gynecologists. Management of acute abnormal uterine bleeding in nonpregnant reproductive-aged women. Obstet Gynecol. 2013;121(4):891-6.
45. Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011; 113(1):3-13.
46. Hammad MF, Alwaraky MS, Maaly MA, Kamel MA, Hamza H. Role of uterine artery embolization in management of abnormal uterine bleeding: A prospective study. Tumori. 2020;106(5):369-74.
47. Ahmedkhalaf-Awad I, Abdellah M. The role of uterine artery embolization in management of abnormal uterine bleeding. SVU Med J. 2021;4(2):65-74.
48. Taeima M, Elkader Y. Role of transcatheter embolization of uterine artery in management of intractable abnormal uterine bleeding. Zagazig Med J. 2013;19(2):115-20.
49. Hatimota P, Gautam H, Kathar KK, Baruah D. Successful embolization of pseudoaneurysm of uterine artery: a case report. Int J Reprod Contracept Obstet Gynecol. 2024;13(11):3398-3401.
50. Ho S, Ong C, Tan B. A case of uterine artery pseudoaneurysms. Singapore Med J. 2002;43(4):202-4.
51. Subramaniam S, Nadarajan C, Aziz M. Role of Uterine Artery Embolization in Pseudoaneurysm of Uterine Artery: A Rare Cause of Secondary Postpartum Hemorrhage. Cureus. 2018;10(2):e2220.
52. Wicaksana A, Agung Setiawan. Unilateral Uterine Artery Embolization Therapy For Secondary Postpartum Hemorrhage In Pseudoaneurysma Of The Sinistra Uterinary Artery Post-Cesarean Section. Asian J Heal Res. 2022;1(2): 57-63.
53. CQ Wu, Nayeemuddin M, Rattray D. Uterine artery pseudoaneurysm with an anastomotic feeding vessel requiring repeat embolisation. BMJ Case Rep. 2018;2018:bcr2018224656.
54. Roeckner JT, Louis-Jacques AF, Zwiebel BR, Louis JM. Uterine artery pseudoaneurysm and embolisation during pregnancy. BMJ Case Rep. 2020;13(5):e234058.
55. Popovic M, Puchner S, Berzaczy D, Lammer J, Bucek RA. Uterine artery embolization for the treatment of adenomyosis: a review. J Vasc Interv Radiol. 2011;22(7):901–9; quiz 909.
56. Jha RC, Takahama J, Imaoka I, Korangy SJ, Spies JB, Cooper C, et al. Adenomyosis: MRI of the uterus treated with uterine artery embolization. AJR Am J Roentgenol. 2003;181(3):851-6.
57. de Bruijn AM, Smink M, Lohle PN, Huirne JAF, Twisk JWR, Wong C, et al. Uterine artery embolization for the treatment of adenomyosis: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017; 28(12):1629-1642.e1.
58. Bratby MJ, Walker WJ. Uterine artery embolisation for symptomatic adenomyosis--mid-term results. Eur J Radiol. 2009;70(1):128-32.
59. Kitamura Y, Allison SJ, Jha RC, Spies JB, Flick PA, Ascher SM. MRI of adenomyosis: changes with uterine artery embolization. AJR Am J Roentgenol. 2006;186(3):855-64.
60. Siskin GP, Tublin ME, Stainken BF, Dowling K, Dolen EG. Uterine artery embolization for the treatment of adenomyosis: clinical response and evaluation with MR imaging. AJR Am J Roentgenol. 2001;177(2):297-302.
61. Singh T, Richa, Swamy AN, Kumar S. Uterine Artery Embolisation for Acquired Uterine Arteriovenous Malformation - A Case Report. J Radiol Clin Imaging. 2020;3(4):110-115.
62. Sagili H, Krishnan N, Keepanasseril A, Priya S, Devaraj S. Uterine artery embolization for uterine arterio-venous malformation. Int J Reprod Contracept Obstet Gynecol. 2021;10(7):2902-2904
63. Markoff G, Quagliarello J, Rosen R, Beckman E. Uterine arterio-venous malformation successfully embolized with isobutyl 2-cyanoacrylate. Am J Obstet Gynecol. 1986;155(3):659-60.
64. Chan C, Chu F, Pun T. Treating a recurrent uterine arteriovenous malformation with uterine artery embolization: a case report. J Reprod Med. 2003;48(11):905-7.
65. Rubod C, Mubiayi N, Robert Y, Vinatier D. Uterine arteriovenous malformation: a rare cause of recurrent metrorrhagia. Gynecol Obstet Fertil. 2005;33(7-8):511-3.
66. Ruiz Labarta FJ, Pintado Recarte MP, Leyte MG, Bravo Arribas C, Álvarez Luque A, Cuñarro López Y, et al. Uterine Artery Embolization of Uterine Arteriovenous Malformation: A Systematic Review. J Pers Med. 2022;12(7):1098.
67. El Agwany AS, Elshafei M. Extensive uterine arteriovenous malformation with hemodynamic instability: embolization for whole myometrium affection. Eur J Obstet Gynecol Reprod Biol. 2018;222: 188-91.
68. Soeda S, Kyozuka H, Suzuki S, Yasuda S, Nomura Y, Fujimori K. Uterine artery embolization for uterine arteriovenous malformation is associated with placental abnormalities in the subsequent pregnancy: two cases report. Fukushima J Med Sci. 2014;60(1):86-90.
69. Imankulova B, Terzic M, Ukybassova T, Bapayeva G, Lesbekov T, Mustafinova G, et al. Repeated pulmonary embolism with cardiac arrest after uterine artery embolization for uterine arteriovenous malformation: A case report and literature review. Taiwan J Obstet Gynecol. 2018;57(6):890-3.
70. Yang MJ, Jeng M. Combination of transarterial embolization of uterine arteries and conservative surgical treatment for pregnancy in a cesarean section scar. J Reprod Med. 2003;48(3):213–6.
71. Zhou Q, Young D, Vingan H. Uterine artery embolization for cervical ectopic pregnancy. Radiol Case Rep. 2015;10(1):72–5.
72. Li Z, Xu W, Hu B, Li M, Zhou J, Ni C. Uterine artery embolization in association with methotrexate infusion for the treatment of tubal ectopic pregnancy. J Interv Med. 2019;1(3):182-187.
73. Krissi H, Hiersch L, Stolovitch N, Nitke S, Wiznitzer A, Peled Y. Outcome and future fertility in women treated with uterine artery embolization and methotrexate for non-tubal ectopic pregnancy. Eur J Obstet Gynecol Reprod Biol. 2014;182:172–6.
74. Marchand GJ, Masoud AT, Coriell C, Ulibarri H, Parise J, Arroyo A, et al. Treatment of cesarean scar ectopic pregnancy in China with uterine artery embo-lization: A systematic review and meta-analysis. J Clin Med. 2022;11(24):7393.
75. Saito S, Tanabe K, Sato A, Akaishi M, Hayashi C, Yokomizo R, et al. Live birth after a Cesarean Scar Pregnancy Treated with Methotrexate Administration, Uterine Artery Embolization, Hysteroscopic Removal of Conceptus, and Laparoscopic Repair of Uterine Scar: Case report. Japanese Journal of Gynecologic and Obstetric Endoscopy. 2012; 30(1):240-246.
76. Lisowski A, Drelichowski S, S?oka-Sutkowska A, Wi?niewski D, Malinowski J. Intravascular embolization of the uterine arteries in the treatment of early post-partum haemorrhage. Ginekol Pol. 2011;82(2):146-9. Polish
77. Pelage JP, Limot O. Current indications for uterine artery embolization to treat postpartum hemorrhage. Gynecol Obstet Fertil. 2008; 36(7-8):714-20.
78. Myers TT. Uterine Artery Embolization for Postpartum Hemorrhage. J Radiol Nurs. 2016;35(2):142-5.
79. Aoki M, Tokue H, Miyazaki M, Shibuya K, Hirasawa S, Oshima K. Primary postpartum hemorrhage: outcome of uterine artery embolization. Br J Radiol. 2018;91(1087):20180132.
80. Farouk O, Elbasuony W, Elbohouty A. Uterine artery embolization versus surgical management in primary atonic postpartum hemorrhage. Egypt J Radiol Nucl Med. 2016;47(2):817-23.
81. Rossetti D, Vitale SG, Gulino FA, Biondi A, Cignini P, Rapisarda AMC, et al. Pelvic arterial embolization for postpartum hemorrhage: long term results of a single center experience in 29,091 deliveries. Clin Exp Obstet Gynecol. 2016;43(5):733-6.
82. Kim MJ, Kim IJ, Kim S, Park IY. Postpartum hemorrhage with uterine artery embolization: risk of complications of uterine artery embolization. Minim Invasive Ther Allied Technol. 2022;31(2):276-283.
83. Koganemaru M, Nonoshita M, Iwamoto R, Kuhara A, Nabeta M, Kusumoto M, et al. Endovascular management of intractable postpartum hemorrhage caused by vaginal laceration. Cardiovasc Intervent Radiol. 2016;39(8):1159-64.
84. Chen T-H, Chen C-H, Hong Y-C, Chen M. Puerperal pelvic hematoma successfully treated by primary transcatheter arterial embolization. Taiwan J Obstet Gynecol. 2009;48(2):200–2.
85. Matsubara S, Sato T, Nakata M. Vaginal artery embolization with a permanent embolic agent for intractable postpartum hemorrhage. J Obstet Gynaecol Res. 2011;37(4):377-8.
86. Yamashita Y, Takahashi M, Ito M, Okamura H. Transcatheter arterial embolization in the management of postpartum hem-orrhage due to genital tract injury. Obstet Gynecol. 1991;77(1):160–3.
87. Lee JM, Park JS, Shim J. The effectiveness of pelvic arterial embolization for intractable postpartum hemorrhage after hysterectomy. J Korean Soc Radiol. 2019;80(1):98
88. Dönmez H, Öztürk MH, Gürgen F, Soylu SO, Hekimoglu B. Intractable postpartum hemorrhage resulting from uterine artery pseudoaneurysm: embolization via the collateral route. Cardiovasc Intervent Radiol. 2007;30(2):310-2.
89. Fernandez MG, de Carvalho SFC, Martins BA, da Silva Mota Santos F, Falcão Paixão Neto FA, de Araujo Medeiros MO, et al. Uterine artery embolization versus hysterectomy in postpartum hemorrhage: a systematic review with meta-analysis. J Endovasc Ther. 2024;15266028241252730.
90. Wang Z, Li X, Pan J, Zhang X, Shi H, Yang N, et al. Uterine Artery Embolization for Management of Primary Postpartum Hemorrhage Associated with Placenta Accreta. Chin Med Sci J. 2016;31(4):228-232.
91. Li X, Wang Z, Chen J, Shi H, Zhang X, Pan J, et al. Uterine artery embolization for the management of secondary postpartum haemorrhage associated with placenta accreta. Clin Radiol. 2012; 67(12):e71-6.
92. Jeon GU, Kim YR, Ahn E, Jung SH. Uterine artery embolization for postpartum hemorrhage with placenta accreta spectrum. Acta Radiol. 2023;64:2321-6.
93. Brustman D, Raupach J, Chovanec V, Ryska P. Uterine artery embolisation in symptomatic patients with placenta accreta spectrum disorders. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2024. Online ahead of print.
94. Malik S, Shams M. Role of uterine artery embolization in the management of cervical cancer. J Cancer Sci Ther. 2012;4:167-169.
95. Yalvac S, Kay?kç?oglu F, Boran N, Tulunay G, Kose MF, Bilgiç S, et al. Embolization of uterine artery in terminal stage cervical cancers. Cancer Invest. 2002;20(5-6):754-8.
96. Bianchi F, de León M, Ballarino B, Ceretti M, Quiroga F, Garcia Balcarce T, et al. Emergency embolization in locally advanced cervical cancer: a case series in a tertiary referral center in Argentina. Obstet Gynecol Int J. 2024;15(2):88-91.
97. Habánová H, Mikula P, Tvrdík T, Dedinská E, Komaromy K, Rusnák I. Emergency uterine artery embolization used for managing profuse intra-abdominal bleeding and uterine rupture in a patient with advanced cervical cancer. Diagnostics (Basel). 2022;12(5):1081.
98. Yang X, Xu G, Wu GN, Li Z, Zhang G. Superselective uterine artery chemoembolization for treatment of locally advanced cervical cancer. Chin J Radiol. 2013;47:735-8.
99. Wang X, Chen J, Liu Y, Li N, Zhang H, Li J. Clinical research of uterine artery chemoembolization combined with radiotherapy for intermediate and advanced cervical cancer. Chin J Clin Oncol. 2013; 36:34-7.
100. Zhou QC, Yu CX, Zhu X, Lu P, Wang Q, Wang D. Clinical effect of uterine artery infusion chemotherapy plus embolization on cervical cancer. Chin J Pract Gynecol Obstet. 2019;46:80-3.
101. Bohîltea R, Dorobat B, Doldur MM, Cioca A, Ducu I, Mihai B, et al. Uterine arteries embolization - a rescue tool for acute vaginal bleeding in late stages of gynecologic malignancies. Clin. Exp. Obstet. Gynecol. 2022;49(6):142.
Full Text Sources:
Abstract:
Views: 835

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.