Surgery, Gastroenterology and Oncology
|
|
Current Management of Ocular Surface Squamous Neoplasia: A Systematic Review
Andi Muhammad Maksum Abdul Baqi, Halimah Pagarra, Suliati P. Amir, Andi Pratiwi
Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
ABSTRACT
Background: Ocular Surface Squamous Neoplasia (OSSN) represents a range of conditions from epithelial dysplasia to invasive carcinoma. Recent advancements in OSSN management have incorporated topical pharmacological agents as alternatives or complements to surgical interventions. This systematic review summarizes the current documentation on the efficacy, safety, and recurrence rates associated with various OSSN therapeutic modalities.
Methods: A systematic literature search was conducted across PubMed, ScienceDirect, SpringerLink, and Google Scholar to locate primary studies published between 2019 and 2024 investigating OSSN therapies. Eighteen out of the 292 initially identified articles were selected. The data extracted included therapy type, clinical outcome, and adverse effects.
Results: Topical administration of interferon alfa-2b (IFNa2b) had a high efficacy, low toxicity, and low recurrence rate. The combination of IFNa2b and 5-fluorouracil (5-FU) achieved complete tumor resolution without recurrence for up to 16 months. Mitomycin-C and 5-FU were effective; however, these options were associated with higher local toxicities than those produced by IFNa2b or combination of IFNa2b and 5-FU. Surgical excision was identified as crucial for extensive or invasive lesions, with recurrence contingent on margin status and adjuvant therapy. An individualized therapeutic approach based on lesion characteristics and patient condition was strongly emphasized.
Conclusions: Current OSSN management favors safe, effective, non-surgical therapies. Topical IFNa2b was identified as a preferred modality due to its optimal efficacy and safety profile. Combination therapies and long-term surveillance are critical for minimizing recurrence, while the tailoring of treatment strategies to specific tumor characteristics and patient conditions is essential for achieving superior outcomes.
INTRODUCTION
Ocular Surface Squamous Neoplasia (OSSN) is a neoplasm of the ocular surface originating from the squamous epithelium of the conjunctiva, limbus, and cornea. The term encompasses a spectrum of lesions ranging from mild dysplasia and Conjunctival Intraepithelial Neoplasia (CIN) to invasive Squamous Cell Carcinoma (SCC) (1). OSSN is the most common epithelial tumor of the ocular surface and timely diagnosis and treatment is required to prevent a serious negative impact on visual function. Although the disease predominantly affects older adults, males, and people with prolonged exposure to ultraviolet radiation, OSSN has been observed in younger patients, particularly immunocompromised individuals, such as HIV/AIDS patients or organ transplant recipients (2).
The incidence of OSSN varies globally depending on geographic factors, environmental exposure, and genetic predisposition. The condition has a high prevalence in developing countries, where it is often associated with intense ultraviolet (UV) radiation exposure, limited access to eye care services, and delayed diagnosis (1). In addition to UV exposure, infection with human papillomavirus (HPV), particularly types 16 and 18, and mutations in the tumor suppressor gene p53 have been identified as significant carcinogenic factors. Furthermore, immunosuppression due to HIV infection or iatrogenic causes accelerates the progression of OSSN lesions toward more aggressive and invasive forms (3).
OSSN can present with highly variable clinical manifestations, ranging from flat lesions resembling pterygium to prominent, vascularized nodular tumors. Accurate diagnosis often requires histopathological confirmation via biopsy; however, imaging modalities such as Anterior Segment Optical Coherence Tomography (AS-OCT) are increasingly utilized as non-invasive diagnostic tools to delineate lesion margins and assess lesion depth (4).
The management of OSSN has evolved considerably over the past decades. Traditionally, surgical excision using the “no-touch” technique combined with adjuvant cryotherapy has been the primary treatment modality. However, the subclinical margins and high postoperative recurrence rates observed with this approach have prompted the exploration of non-surgical alternatives (2). Topical pharmacologic therapies such as interferon alfa-2b (IFN-?2b), mitomycin C (MMC), and 5-fluorouracil (5-FU) have demonstrated high efficacies in tumor resolution, albeit with varying toxicity profiles (5). IFN-?2b can induce tumor regression with minimal side effects; therefore, this treatment it an ideal first-line therapy, especially for patients with small lesions or a high risk of surgical complications (6,7).
A global consensus on the optimal management algorithm for OSSN has yet to be established, although various therapeutic options are available. Recent studies have compared the efficacy of monotherapy to that of combination therapy, analyzed the advantages of primary versus adjuvant treatment, and investigated the ideal duration of therapy to prevent long-term recurrence. This literature review was conducted to summarize the scientific evidence on OSSN management published during the past five years, focusing on therapeutic efficacy, adverse effects, recurrence rates, and clinical considerations in modality selection. This knowledge is intended to assist clinicians in the formulation of individualized treatment strategies based on current evidence and patient-specific characteristics.
MATERIALS AND METHODS
This study is a systematic literature review evaluating recent studies on the management of OSSN. The research was conducted based on the principles of evidence-based medicine, adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework (8-10), and is registered in the Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251058042.
Literature Search Strategy
A systematic literature search was conducted using four electronic databases: PubMed, ScienceDirect, SpringerLink, and Google Scholar. Specific search terms were employed, using the following combination of key phrases: "Ocular Surface Squamous Neoplasia" AND (management OR treatment OR therapy).
Each database was searched independently, and the results were screened according to predefined inclusion and exclusion criteria. In addition, the reference lists of selected articles were reviewed to identify other relevant studies. The final database search was conducted on 9 February 2024.
Inclusion criteria
The inclusion criteria for this review comprised studies that discussed the management of OSSN through surgical, topical, or combined therapies; were published within the last five years (2019-2024); written in English; available in full-text format; and classified as primary research, including clinical trials, observational studies, and case reports.
Exclusion criteria
The exclusion criteria encompassed articles written in languages other than English and studies that were not available in full text; irrelevant to OSSN management; or classified as narrative reviews, editorials, commentaries, conference abstracts, or experimental studies conducted on animals or in vitro.
Study Selection and Data Extraction
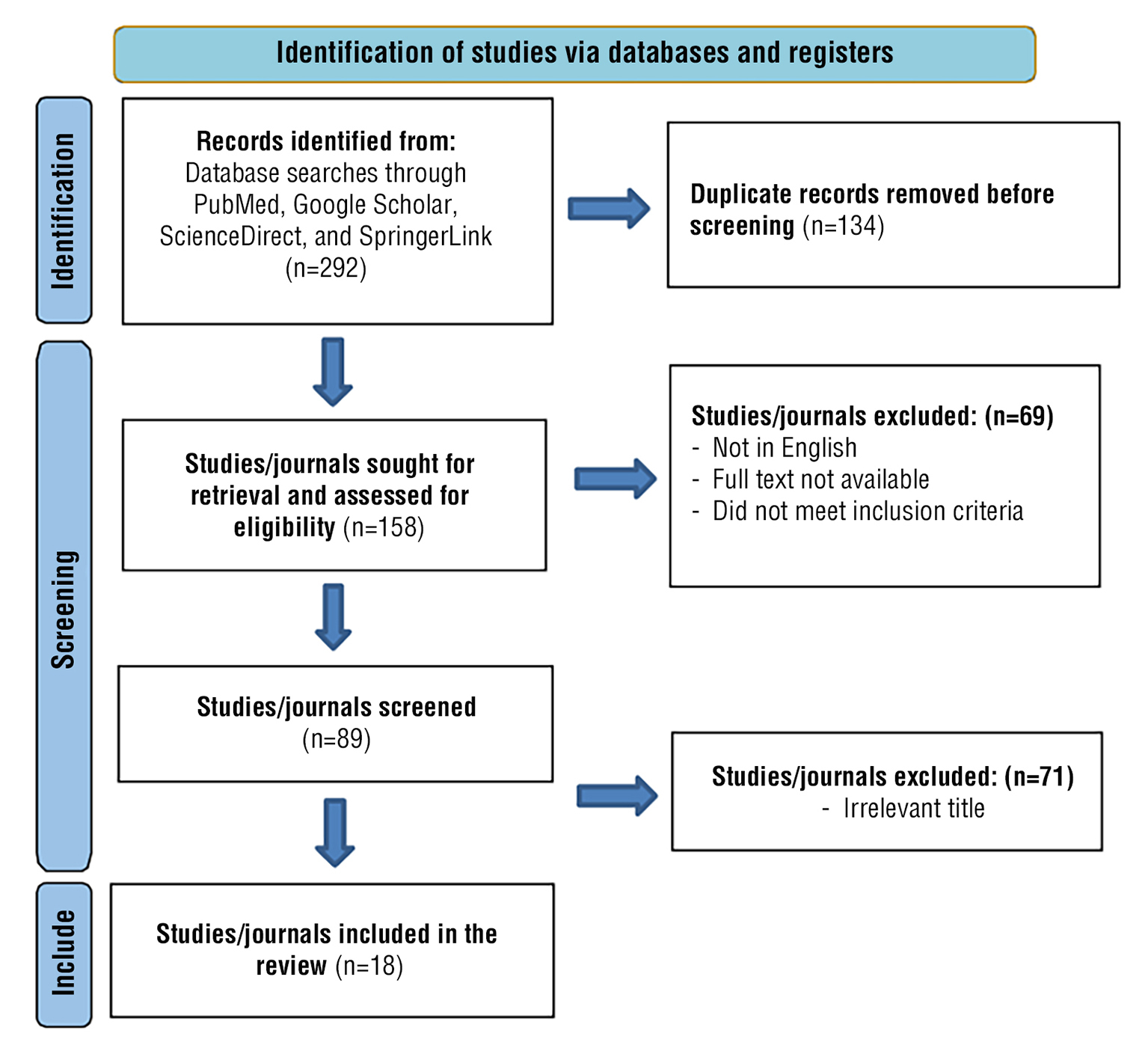
A total of 292 initial articles were identified across the four databases. After removing duplicates (n=134), 158 studies were screened based on title and abstract. From this process, 89 full-text articles were assessed for eligibility, and 18 met the inclusion criteria for further analysis. The article selection process is illustrated in the PRISMA flow diagram (fig. 1).
Figure 1 - PRISMA diagram for systematic review search
Data from the selected studies were manually retrieved using a structured extraction form. The extracted information included author names, year of publication, study location, study design, sample size, type of therapy administered (topical, surgical, or combination), level of evidence (according to the 2011 Oxford Centre for Evidence-Based Medicine), clinical outcome (resolution rate, duration of therapy, and recurrence), and reported adverse effects.
Data Extraction and Synthesis
Two reviewers independently carried out the extraction process, and the other authors verified the accuracy of the retrieved information. Any differences were resolved by consensus among all four authors. In accordance with PRISMA 2020 guidelines, the data were synthesized integratively and summarized in both tables and narrative text.
RESULTS
A total of 18 studies met the inclusion criteria after screening 292 initial records. Design spanned retrospective cross-sectional studies, cohort analyses, case series, and systematic reviews. Therapeutic approaches included surgical excision (often with adjuvant cryotherapy), topical pharmacotherapy (interferon alfa-2b [IFN?2b], mitomycin-C [MMC], 5-fluorouracil [5-FU]), combined regimens (particularly IFN?2b plus 5-FU), and novel procedural options such as laser.
Topical IFN?2b demonstrated high tumor control rates of up to 95% with recurrence between 0-7% during mean treatment durations of 3-6 months.
The IFN?2b+5-FU combination achieved complete resolution with no recurrences during follow-up of up to 16 months. Surgical excision with negative margins and adjuvant therapy produced recurrence rates as low as 1.5%, while recurrence rose to 17–20% with positive or indeterminate margins. MMC and 5-FU were effective but consistently associated with higher ocular surface toxicity compared with IFN?2b.
In addition to these conventional strategies, newer reports highlighted rapid remission of extensive corneal surface neoplasia with topical interferon therapy (24), as well as successful management of recurrent or nodulo-ulcerative variants using combined surgical and adjuvant approaches (25,26).
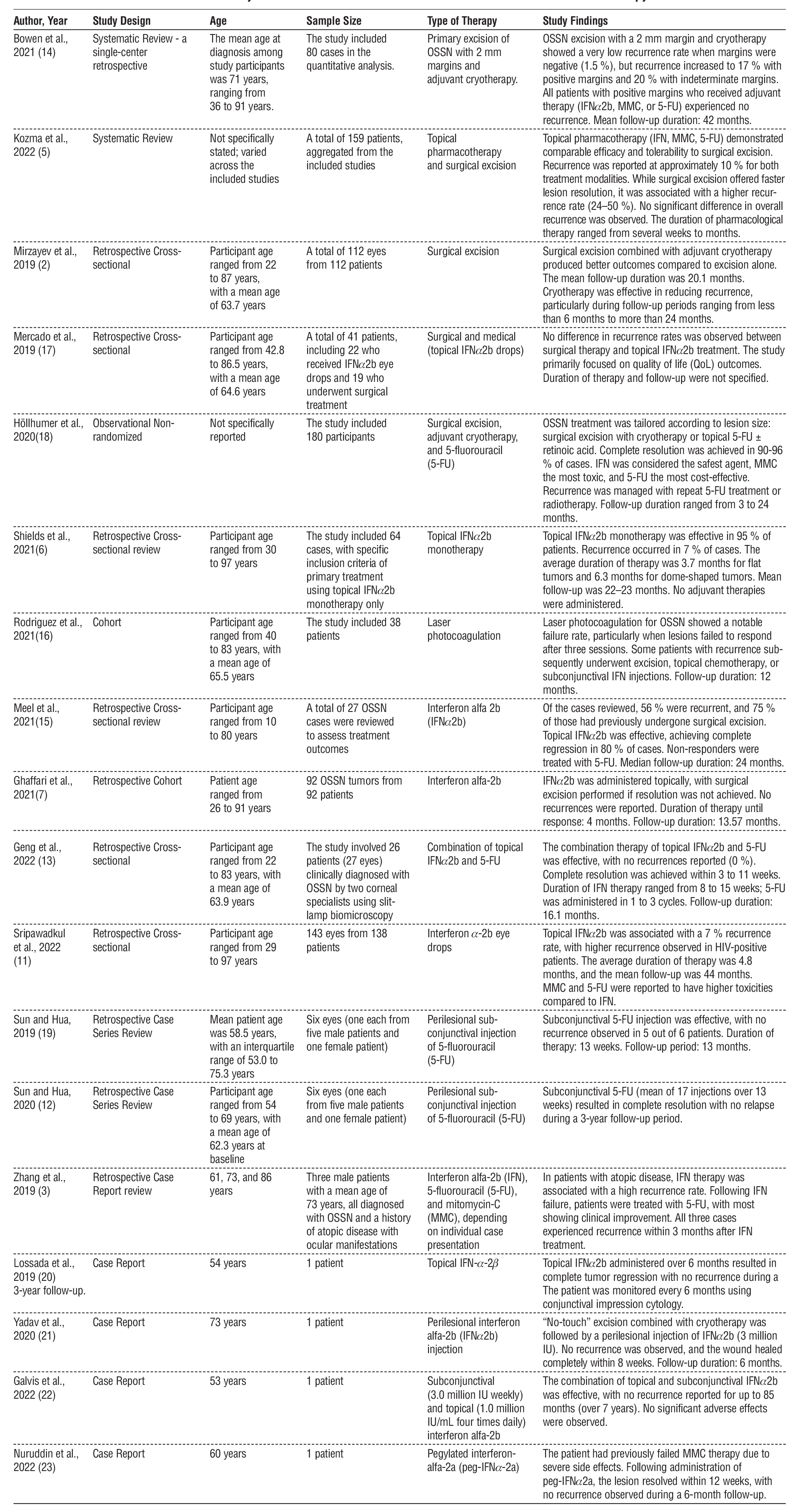
The characteristics of the studies included in this systematic review are presented in table 1.
Table 1 - Summary of Recent Clinical Research Results on the Effectiveness of OSSN Therapy
DISCUSSION
A deeper understanding of the biological behavior of tumors and the emergence of safer and more effective non-surgical therapies have resulted in considerable advancements in the management of OSSN through effective surgical and/or topical pharmacologic approaches. Traditional surgical interventions, such as excision using the “no-touch” technique combined with adjuvant cryotherapy, have long been the standard of care, particularly for large or invasive lesions (2). However, the limitations of surgery in addressing subclinical tumor margins have driven the adoption of topical therapies as both alternative and adjuvant treatments.
Interferon alfa-2b (IFN?2b), an immunomodulatory agent, is increasingly employed as a first-line therapy for OSSN due to its favorable toxicity profile and high efficacy in reducing recurrence rates (6). Topical IFN?2b monotherapy has been shown to achieve a tumor control rate of up to 95 %, with no significant differences in efficacy based on tumor configuration. Sripawadkul et al. (2022) corroborated these findings by reporting a post-treatment OSSN recurrence rate of 7 %, with a cumulative recurrence rate of 3.1 % after five years (11).
Compared to other chemotherapeutic agents such as mitomycin C (MMC) and 5-fluorouracil (5-FU), IFN?2b has a milder side effect profile. While MMC has shown resolution rates of up to 100 %, it is frequently associated with severe local complications, including epithelial toxicity, hyperemia, toxic keratitis, punctal stenosis, and even limbal stem cell deficiency (12). As a result, MMC is often reserved for refractory OSSN cases or used as an adjuvant therapy following surgery under strict supervision.
Meanwhile, 5-FU has been proven effective in the treatment of OSSN, both topically and via perilesional injection. Geng et al. (2022) reported that the combination of topical IFN?2b and 5-FU resulted in high tumor resolution rates with no recurrence observed during the follow-up period of 16.1 months. This combination was well-tolerated, caused no significant irritation, more cost-effective, and did not require the special storage conditions necessary for IFN?2b or MMC; therefore, this option is an attractive therapeutic alternative, particularly in developing countries (13).
Topical IFN?2b remains a cornerstone in the medical management of OSSN, consistently demonstrating high resolution rates with minimal side effects compared to MMC or 5-FU. Recent studies confirm its broader applicability, including rapid remission in extensive lesions (24). The combination of IFN?2b and 5-FU has further strengthened medical therapy options, achieving complete resolution without recurrence during medium-term follow-up, and proving particularly relevant in resource-limited settings.
Bowen et al. (2021) used surgical excision with a 2 mm margin combined with adjuvant cryotherapy to yield favorable outcomes, with a recurrence rate of 1.5 % in patients with negative margins, compared to 17–20 % in those with positive or unclear margins (14). These findings highlight the importance of strict margin control and underscore the critical role of adjuvant therapy in preventing tumor recurrence. A study by Kozma et al. (2022) supported these observations by reporting that topical therapy exhibited a recurrence rate comparable to surgical excision - approximately 10 % - but with a lower risk of complications (5).
Despite these advances, surgical excision continues to hold a crucial role for large or invasive lesions, especially where margin control can be achieved. The stark difference between recurrence rates in negative versus positive/indeterminate margins highlights the importance of meticulous technique. In addition, newer reports of nodulo-ulcerative and recurrent variants (25,26) emphasize the importance of individualized, multimodal approaches that combine surgical and pharmacologic strategies.
In recurrent cases, combination therapy has proven to be more effective than monotherapies. Meel et al. (2021) reported that 56 % of the OSSN cases in their study were recurrences, and most of these involved prior surgical excisions. The administration of primary immunotherapy with IFN?2b followed by topical chemotherapy in cases of incomplete regression prevented the need for re-excision and provided long-term tumor control (15).
HIV-positive patients demonstrated higher recurrence with IFN?2b therapy, suggesting the need for closer follow-up and potential use of combination regimens. Patients with atopic disease showed early recurrence after IFN therapy, requiring alternative strategies such as 5-FU or MMC. Emerging insights into the genetic and epigenetic landscape of OSSN may explain inter-individual variability in treatment response and recurrence, suggesting a potential role for molecular stratification in future therapeutic algorithms (27).
Other alternative therapies explored by Rodriguez et al. (2021), such as laser photocoagulation, perilesional bevacizumab, and cidofovir, remain in the exploratory phase and cannot yet be recommended as standard treatments due to limited long-term clinical evidence (16). However, in cases of large or refractory OSSN, viable options may include radiotherapy modalities such as plaque brachytherapy and proton beam therapy (16).
Overall, the choice of OSSN therapy largely depends on tumor size and location, degree of invasion, patient immune status, availability of medical facilities, and patient preferences. IFN?2b appears to offer the most balanced profile in terms of efficacy and safety, while MMC and 5-FU remain strong alternatives under specific clinical circumstances. Long-term follow-up is crucial for the early detection of recurrence and the assessment of ensuing outcomes associated with each therapeutic modality (11).
Clinicians should consider topical IFN?2b as first-line therapy for limited lesions, escalate to IFN?2b+5-FU for suboptimal responders or cost-sensitive contexts, reserve MMC for refractory disease with careful toxicity monitoring, and employ surgery for invasive cases with adjuvant support. Long-term follow-up remains essential to monitor recurrence and late complications. Collectively, these contemporary studies (24,25,26,28) emphasize that the therapeutic landscape of OSSN is rapidly evolving, and clinicians should integrate both clinical evidence and emerging molecular data to optimize patient outcomes.
Limitations
The limitations of this study include the restricted temporal scope (2019-2024), which may have resulted in the exclusion of some essential foundational research or long-term follow-up data for understanding evolving therapeutic trends and the sustained efficacy of established treatments. In addition, considerable heterogeneity was observed among the included studies regarding patient demographics, lesion characteristics, specific treatment protocols (e.g., dosage, duration, surgical techniques), and outcome-reporting methodologies. This heterogeneity precluded a robust meta-analysis and limited both the direct comparability and generalizability of the synthesized results. In addition, the predominance of observational or retrospective study designs, along with a paucity of head-to-head randomized comparative trials, caused an increase in the inherent risks of selection bias and confounding, thereby weakening the evidence supporting definitive therapeutic recommendations. Finally, the potential for publication bias and the varied and often limited follow-up durations reported in several studies restrict the thorough assessment of long-term recurrence rates and sustained safety profiles that are key considerations for a condition such as OSSN, which is known for its potential for late relapse.
CONCLUSIONS
This review indicated that the management of OSSN has undergone considerable advancements over the past five years, with topical therapies such as interferon alfa-2b (IFN?2b) proving to be an effective and safe primary treatment option. Furthermore, the combination of IFN?2b with agents such as 5-fluorouracil (5-FU) has shown promising clinical outcomes with low recurrence rates. Although surgical therapy remains an important option, particularly in invasive cases, strict margin control and the use of adjuvants are required to reduce the risk of relapse. The clinical relevance of these findings highlights the importance of an individualized therapeutic approach based on lesion characteristics and patient conditions, as well as the necessity for long-term follow-up to prevent recurrence and complications.
Acknowledgements
The researchers would like to express their sincere gratitude to the Faculty of Medicine at Hasanuddin University in Makassar, Indonesia, for their generous support of this research.
Author’s Contributions
A.M.B: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, validation, visualization, Writing – original draft, Writing – review & editing. H.P: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, software, validation, visualization, writing - original draft. S.P.A: conceptualization, data curation, formal analysis, investigation, methodology, resources, supervision, validation, visualization, writing – original draft, writing – review & editing. A.P: conceptualization, data curation, formal analysis, investigation, methodology, resources, writing – original draft, writing – review & editing.
Competing Interests
No competing interests were reported.
Funding
Self-funding
Ethics Approval
This research did not involve human subjects;
therefore, it was exempt from ethical clearance.
Data Availability Statement
All reviewed papers can be obtained from journals.
REFERENCES
1. Hossain RR, Oh JA, McLintock C, Murphy C, McKelvie J. Ocular Surface Squamous Neoplasia: A 12-Month Prospective Evaluation of Incidence in Waikato, New Zealand. Vision (Basel). 2022;6(3):50.
2. Mirzayev I, Gündüz AK, Özalp Ateæ FS, Özcan G, Iæ?k MU. Factors affecting recurrence after surgical treatment in cases with ocular surface squamous neoplasia. Int J Ophthalmol. 2019;12(9):1426-1431.
3. Zhang L, Mercado C, Galor A, Holland EJ, Wang G, Karp CL. Challenging Treatment of Ocular Surface Squamous Neoplasia in Patients with Atopic Disease. Ocul Immunol Inflamm. 2019;27(2):288-293.
4. Baækan C, K?l?carslan A. How Can We Diagnose Ocular Surface Squamous Neoplasia With Optical Coherence Tomography? Cureus. 2023;15(3):e36320.
5. Kozma K, Réka Dömötör Z, Csutak A, Szabó L, Hegyi P, Er?ss B, et al. Topical pharmacotherapy for ocular surface squamous neoplasia: systematic review and meta-analysis. Sci Rep. 2022;12(1):14221.
6. Shields CL, Constantinescu AB, Paulose SA, Yaghy A, Dalvin LA, Shields JA, et al. Primary treatment of ocular surface squamous neoplasia with topical interferon alpha-2b: Comparative analysis of outcomes based on original tumor configuration. Indian J Ophthalmol. 2021;69(3):563-567.
7. Ghaffari R, Barijani S, Alivand A, Latifi G, Ghassemi H, Zarei-Ghanavati M, et al. Recombinant Interferon Alpha-2b as Primary Treatment for Ocular Surface Squamous Neoplasia. J Curr Ophthalmol. 2021;33(3):260-265.
8. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
9. Oley MH, Oley MC, Sukarno V, Faruk M. Advances in Three-Dimensional Printing for Craniomaxillofacial Trauma Reconstruction: A Systematic Review. J Craniofac Surg. 2024; 35(7):1926-1933.
10. Warsinggih, Aryanti C, Faruk M. Optimum management for complex anal fistula: a network meta-analysis of randomized controlled trials. Surg Open Sci. 2024;18:117-122.
11. Venkateswaran N, Sripawadkul W, Karp CL. The role of imaging technologies for ocular surface tumors. Curr Opin Ophthalmol. 2021;32(4):369-378.
12. Sun Y, Hua R. Long-Term Efficacy and Safety of Subconjunctival /Perilesional 5-Fluorouracil Injections for Ocular Surface Squamous Neoplasia. Drug Des Devel Ther. 2020;14:5659-5665.
13. Geng W, Wang JS, Shi BJ, Xie HT, Zhang MC. Topical Chemotherapy for Treating Ocular Surface Squamous Neoplasia with a Combination of Interferon a-2b and 5-Fluorouracil. Ophthalmol Ther. 2022;11(4):1563-1576.
14. Bowen RC, Soto H, Raval V, Bellerive C, Yeaney G, Singh AD. Ocular surface squamous neoplasia: outcomes following primary excision with 2?mm margin and cryotherapy. Eye (Lond). 2021;35(11):3102-3109.
15. Meel R, Dhiman R, Vanathi M, Sen S, Gupta N, Tandon R. Treatment outcome with interferon alpha 2b in ocular surface squamous neoplasia: Recommendation as primary treatment by peripheral ophthalmologists. Oman J Ophthalmol. 2021;14(1):27-32.
16. Rodriguez EEC, Castelo Branco Sancho KF, Mencaroni Kange P, de Nadai Barros J, Sutili Toledo A, Morales M, et al. Novel low-cost approach to the treatment of ocular surface squamous neoplasia using pattern scanning laser photocoagulation. Arq Bras Oftalmol. 2020;83(6):505-510.
17. Mercado CL, Pole C, Wong J, Batlle JF, Roque F, Shaikh N, et al. Surgical versus medical treatment for ocular surface squamous neoplasia: A quality of life comparison. Ocul Surf. 2019;17(1):60-63.
18. H?llhumer R, Williams S, Michelow P. Ocular surface squamous neoplasia: management and outcomes. Eye (Lond). 2021;35(6): 1562-1573.
19. Sun Y, Hua R. Ocular surface squamous neoplasia: angiographic characteristics and response to subconjunctival/perilesional 5-fluorouracil injections. Drug Des Devel Ther. 2019;13:1323-1334.
20. Rocha-de-Lossada C, Alba-Linero C, Borroni D, Rachwani-Anil R, Zamorano-Martín F, Rodríguez-Calvo-de-Mora M. Relapsed ocular squamous surface neoplasia treated with topical interferon alfa-2b. Rom J Ophthalmol. 2020;64(1):62-65.
21. Yadav SP, Patil SS, Deshpande RD. Management of ocular surface squamous neoplasia extending up to a filtering trabeculectomy bleb. Indian J Ophthalmol. 2020;68(11):2540-2542.
22. Galvis V, Moreno NJ, Tello A, Carreño NI. Topical interferon alpha-2b for a giant ocular surface squamous neoplasia: 7 years of follow-up after complete remission. BMJ Case Rep. 2021;14(2):e240994.
23. Nuruddin M, Roy SR, Hoque F. Pegylated interferon-alpha-2a for the treatment of ocular surface squamous neoplasia. Oman J Ophthalmol. 2022;15(1):81-84.
24. Tripathi, M., Markan, A. Rapid remission of extensive corneal surface neoplasia with topical interferon therapy. Eye. 2025;1:1-3.
25. Das S, Gupta N, Kumar A, Saran S, Kumar A. Recurrent ocular surface squamous neoplasia treated with orbital exenteration. Indian Journal of Ophthalmology - Case Reports. 2024;4(1):23-25.
26. Vempuluru SV, Luthra A, Sinha P, Gavara S, Kaliki S. Nodulo-ulcerative ocular surface squamous neoplasia in 27 patients: clinical presentation, management and outcomes. Semin Ophthalmol. Epub 2024 Nov 29.
27. Kounatidou NE, Vitkos E, Palioura S. Ocular surface squamous neoplasia: Update on genetics, epigenetics and opportunities for targeted therapy. Ocul Surf. 2024;35(1):1-14.
28. Tsatsos M, Delimitrou C, Tsinopoulos I, Ziakas N. Update in the diagnosis and management of ocular surface squamous neoplasia (OSSN). J Clin Med. 2025;1s4(5):1699.
Full Text Sources:
Abstract:
Views: 1557

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.