Surgery, Gastroenterology and Oncology

|
|
Highlights:
A randomized controlled study (RCT) that discusses the impact of biliopancreatic limb length, gastric pouch length, and total small bowel length on weight loss and nutritional parameters after One-anastomosis gastric bypass (OAGB).
Longer BPL lengths (200 cm) in OAGB are associated with greater %TWL and %EWL compared to shorter limb lengths (150 cm).
Patients with longer BPL lengths (170 cm and 200 cm) exhibit significantly higher rates of postoperative nutritional deficiencies, particularly in serum albumin, calcium, iron, and ferritin levels.
While a 200 cm BPL may offer enhanced weight loss, the increased risk of malnutrition suggests that a shorter BPL (150 cm) may provide a better balance between weight loss and nutritional safety.
ABSTRACT
Background: One-anastomosis gastric bypass (OAGB) is an established metabolic and bariatric surgical (MBS) procedure that integrates restrictive and malabsorptive mechanisms. The length of the biliopancreatic limb (BPL) plays a critical role in determining both the efficacy and nutritional safety of the operation. Objectives: To compare outcomes of OAGB with BPL lengths of 150 cm, 170 cm, and 200 cm from the duodenojejunal junction, with additional evaluation of impact of gastric pouch length and total small bowel length (SBL) on postoperative weight and nutritional parameters.
Methods: In this randomized controlled trial, 60 patients were assigned to one of three equal groups based on BPL length. Gastric pouch length and SBL were measured intraoperatively. Primary outcomes included percentage of total weight loss (%TWL), percentage of excess weight loss (%EWL), and the incidence of nutritional deficiencies in albumin, calcium, iron, ferritin, and total protein. Remission of type 2 diabetes mellitus (T2DM) and hypertension (HTN) was also assessed over a 12-month follow-up. Setting: University Hospital
Results: Patients in the 200 cm BPL group demonstrated significantly greater %TWL and %EWL compared to those with a 150 cm BPL (p < 0.05). However, longer BPL lengths (170 cm and 200 cm) were associated with significantly higher rates of postoperative deficiencies in albumin, calcium, iron, and ferritin (p < 0.05). There were no significant differences in T2DM or HTN remission across the groups. Gastric pouch length and SBL showed no correlation with weight loss or nutritional outcomes.
Conclusion: A 150 cm BPL in OAGB offers a favorable balance between effective weight loss and reduced nutritional complications. Although a 200 cm limb enhances weight loss, it is associated with increased nutritional risk. Routine measurement of small bowel length may be useful, but further randomized trials are needed to determine its clinical relevance.
Introduction
In both developed and developing countries, the rising prevalence of obesity has become a major public health crisis, with escalating treatment costs closely linked to its growing burden (1). This insidious condition significantly reduces life expectancy and is associated with a high incidence of comorbidities, particularly among younger populations (2). Obesity is now recognized as an independent risk factor for mortality, with an estimated 2.8 million obesity-related deaths occurring annually worldwide (3). Common comorbidities include type 2 diabetes mellitus (T2DM), stroke, hyperlipidemia, asthma, cardiovascular disease, hypertension (HTN), musculoskeletal disorders affecting weight-bearing joints, obstructive sleep apnea, depression, and several types of malignancies (4).
Among the most commonly performed metabolic and bariatric surgeries (MBS) are sleeve gastrectomy (SG), one-anastomosis gastric bypass (OAGB), and Roux-en-Y gastric bypass (RYGB) (5). SG has gained popularity due to its technical simplicity and favorable early outcomes (1). However, concerns have emerged regarding its modest long-term weight loss and a higher incidence of postoperative gastroesophageal reflux disease (GERD) (6). In contrast, OAGB has rapidly gained traction and is now the third most performed bariatric procedure worldwide, increasingly recognized as a standard option (5). Several studies have reported that OAGB yields superior long-term outcomes in terms of weight loss and resolution of comorbidities when compared to both SG and RYGB (7).
Despite its effectiveness, OAGB, a hypoabsorptive non-resectional MBS procedure (8), carries a significant risk of micronutrient deficiencies, particularly in vitamin B12, thiamine, fat-soluble vitamins, iron, and folate, which can lead to long-term nutritional complications (9). One key variable influencing this risk is the length of the biliopancreatic limb (BPL). To date, there is no consensus on the optimal BPL length, and ongoing research continues to investigate various configurations in an effort to maximize weight loss while minimizing obesity-related complications and nutritional deficiencies (10).
This prospective study compares weight loss and nutritional outcomes across three standardized OAGB limb lengths (150 cm, 170 cm, and 200 cm), aiming to inform surgical decision-making and enhance long-term safety.
METHODS
Study Design and Setting
This was a single-center, prospective, randomized clinical trial conducted at the Bariatric surgery department of a tertiary hospital, between May 2023 and June 2024. The study adhered to CONSORT reporting standards.
Participants Sixty patients aged 18-60 years with a BMI ?35 kg/m² and at least one significant obesity-related comorbidity (e.g., T2DM or hypertension), who failed conservative treatment for ? 6 months, were recruited. Exclusion criteria included prior abdominal or MBS procedure, known nutritional deficiencies, pregnancy or lactation, significant cardiopulmonary disease, systemic illness, active substance abuse, psychological instability, or a small bowel length (SBL) <6 meters, discovered intraoperatively. Baseline assessments included sex, age, BMI, weight, comorbidities, and laboratory values (albumin, calcium, ferritin, iron, and HbA1c).
Randomization and Allocation
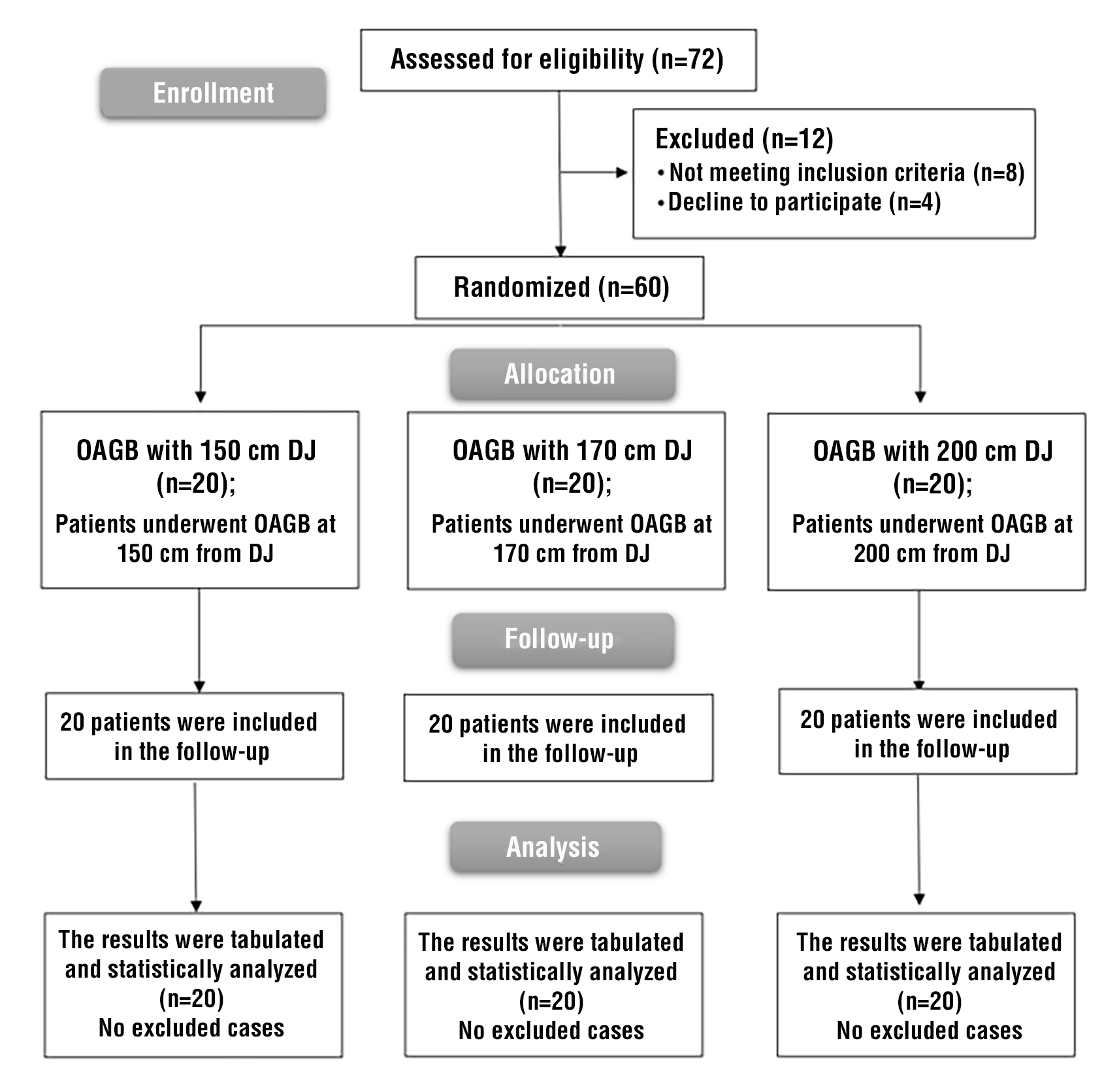
Participants were randomized in a 1:1:1 ratio using a computer-generated sequence to one of three study groups based on biliopancreatic limb (BPL) length: 150 cm (Group I), 170 cm (Group II), or 200 cm (Group III), measured from the duodenojejunal (DJ) flexure. Allocation was concealed using sequentially numbered, coded assignments held by the surgical team. Patients remained blinded to their group assignment. Randomization was stratified by common channel length. Patient enrollment and allocation are depicted in the CONSORT flow diagram (fig. 1).
Figure 1 - CONSORT flow diagram showing patient screening, eligibility assessment, randomization into the three OAGB groups (150 cm, 170 cm, 200 cm BPL from the DJ), follow-up, and analysis.
Surgical Technique
All procedures were performed by a single surgeon using a standardized laparoscopic OAGB technique. Pneumoperitoneum was established via Veress needle entry at the left hypochondrium, and five trocars were placed. The gastric pouch was fashioned over a 36 Fr bougie using sequential 60-mm linear staplers. Staple lines were oversewn with 3/0 PDS.
Small bowel length was measured from the ligament of Treitz to the ileocecal valve using marked graspers (5 cm intervals) in a hand-over-hand fashion. The planned BPL was identified and marked, and the jejunum was held without tension to ensure accurate counting and reduce risk of injury. A posterior gastrojejunal anastomosis was constructed with a 45-mm linear stapler, and the enterotomy was closed with barbed suture. Leak testing was performed in all cases. No drain, nasogastric tube, or Peterson’s defect closure was performed.
Postoperative Protocol
Patients began a clear liquid diet a few hours postoperatively and were discharged on postoperative day one if stable. No contrast study was performed. Dietary progression followed a structured plan: two weeks of liquid diet, followed by a soft diet, then transition to high-protein, calorie-restricted regimens with multi-vitamin supplementation. A dietitian supervised staged food reintroduction.
Follow-Up
Patients were reviewed monthly for the first three months, then every six months, and annually thereafter. Additional visits were scheduled based on patient symptoms. Clinical assessment included weight, BMI, and evaluation of comorbidities. Nutritional labs (albumin, calcium, iron studies) were repeated at follow-up intervals.
Primary Outcomes
Primary endpoints were percentage of total weight loss (%TWL) and excess weight loss (%EWL) at one year. %EWL was calculated using the formula: %EWL = ((Initial weight ? Follow-up weight) ÷ (Initial weight ? Ideal weight)) × 100, where ideal weight corresponds to BMI 25 kg/m2. Associations with gastric pouch length and total small bowel length were explored.
Nutritional Assessment
Serum albumin, calcium, and iron profile were measured during follow-up. Malnutrition was defined by biological indicators, with severe hypoalbuminemia classified as <3.0 g/dL (11).
Secondary Outcomes
Remission of obesity-associated metabolic disorders was assessed. T2DM remission was defined as fasting glucose ?126 mg/dL and HbA1c ?6.5% without medication. Hypertension remission was defined as BP <135/85 mmHg off antihypertensives (12).
Ethical Considerations
All patients included in this study provided informed consent. The study received approval from the University Research Ethical Committee and was registered retrospectively in a publicly accessible clinical trial registry.
Sample Size Calculation
The study was designed with an effectiveness rate of 0.80 and an alpha error of 0.05 to account for any symptomatic occurrences between follow-ups. A confidence interval of 95% was applied. The average %EWL across groups categorized by different lengths (150 cm, 170 cm, and 200 cm) was consistent with existing literature, yielding respective TWLs of 21.8 kg, 36.55 kg, and 43.74 kg. To adequately power the comparative study of OAGB at these varying lengths and to address potential nutritional deficiencies, a total sample size of 54 was calculated, incorporating a 10% buffer for follow-up attrition (20 participants per group).
Statistical Analysis
Statistical analyses were conducted using SPSS v26 (IBM Inc., Armonk, NY, USA). The normality of the data distribution was assessed using the Shapiro-Wilk test and histograms. For parametric data, ANOVA (F) with post hoc (Tukey) tests were employed, presenting results as means and standard deviations (SD). Non-parametric comparisons were made using the Kruskal-Walli’s test in conjunction with the Mann-Whitney U test, with results summarized as medians and interquartile ranges (IQR). For categorical variables, the Chi-square test was utilized, with results expressed as frequency and percentage. A two-tailed P value of 0.05 or lower was considered statistically significant.
RESULTS
Patient Flow and Baseline Characteristics
A total of 72 patients were screened for eligibility; 8 did not meet the inclusion criteria and 4 declined to participate. Consequently, 60 patients were randomly allocated into three groups of 20 each. Comprehensive statistical analyses were conducted for all patients who completed follow-up assessments (fig. 1).
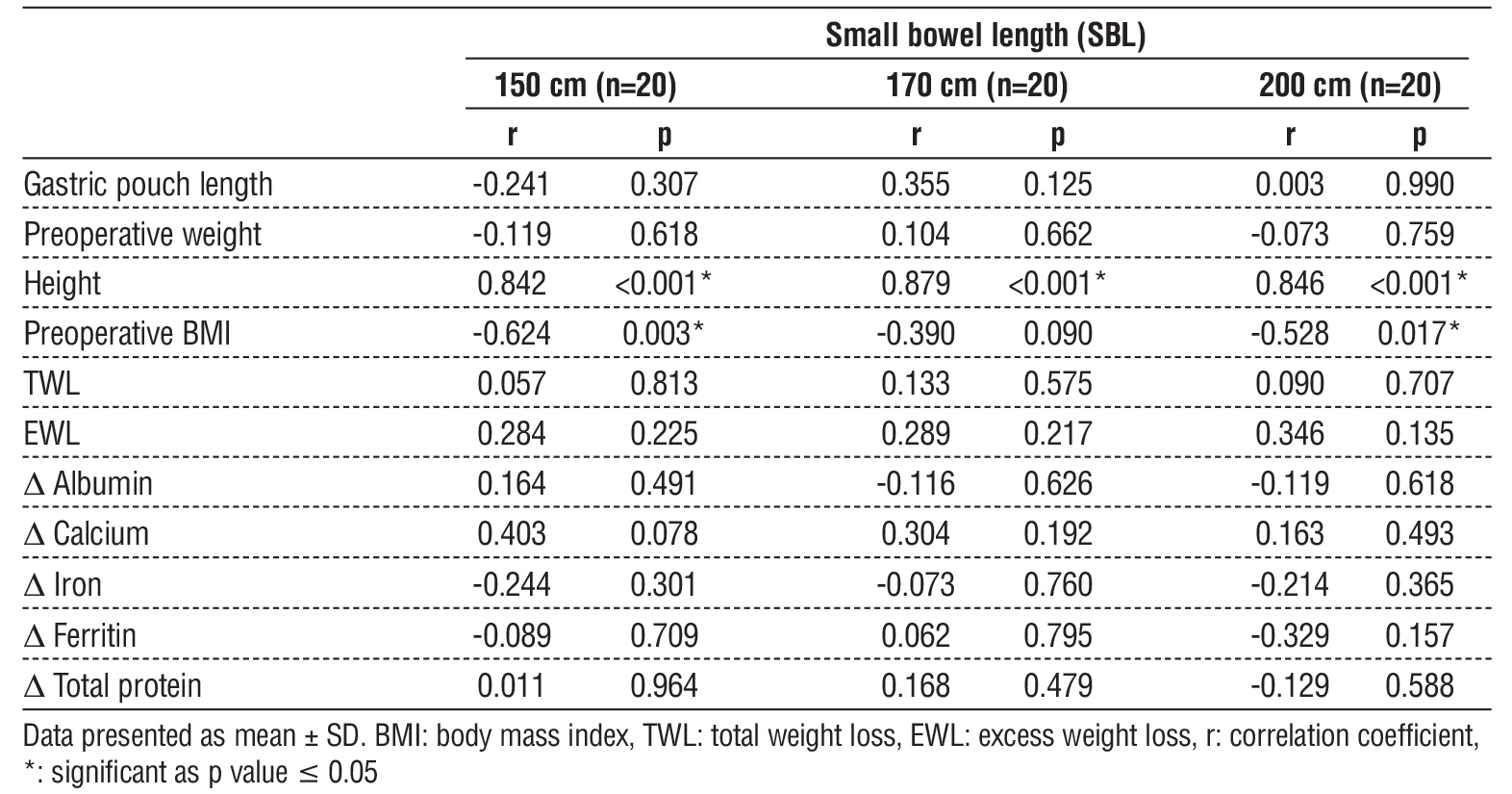
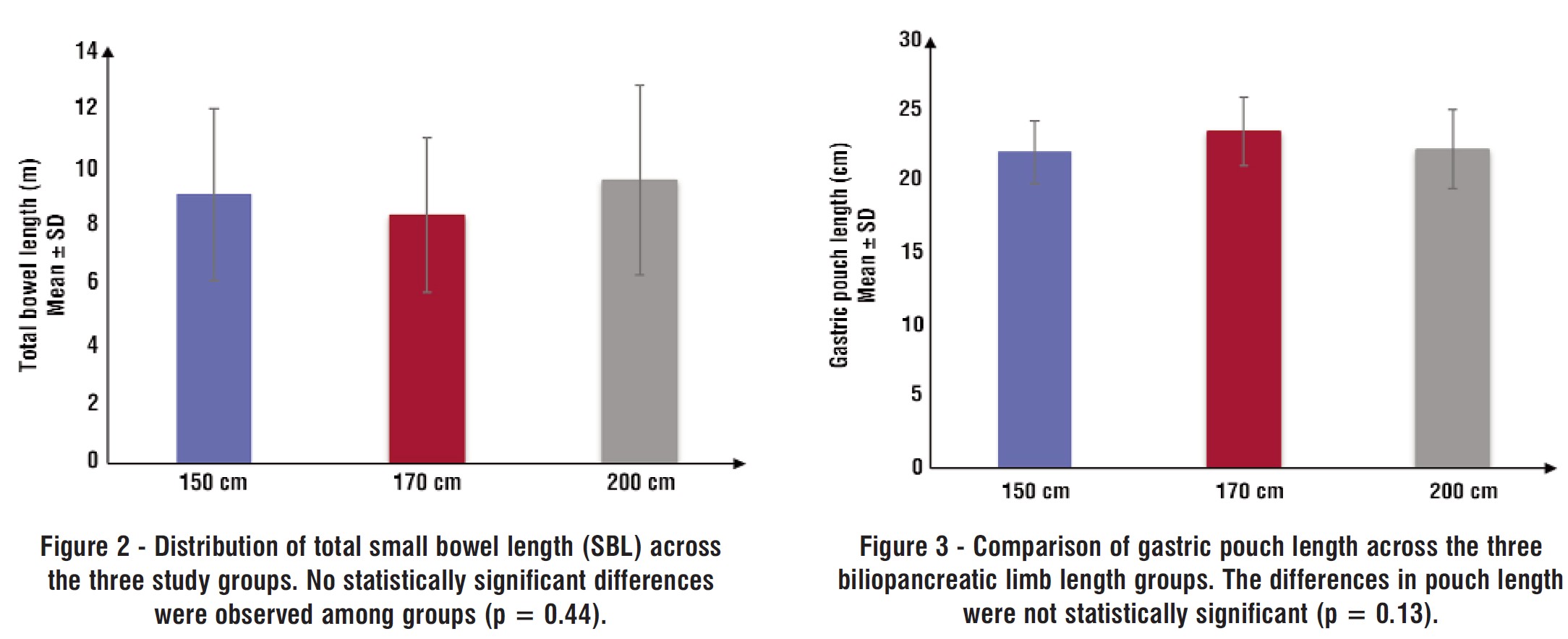
Baseline characteristics, including age, sex, preoperative weight, height, BMI, and the presence of comorbidities such as T2DM and HTN, were comparable across groups with no statistically significant differences (table 1). Total small bowel length and gastric pouch length also did not differ significantly between groups (p = 0.44 and p = 0.13, respectively) (table 2) (fig. 2, fig. 3). A significant positive correlation was observed between patient height and total small bowel length (p < 0.001) (table 3).
Table 1 - Demographic data of the studied groups
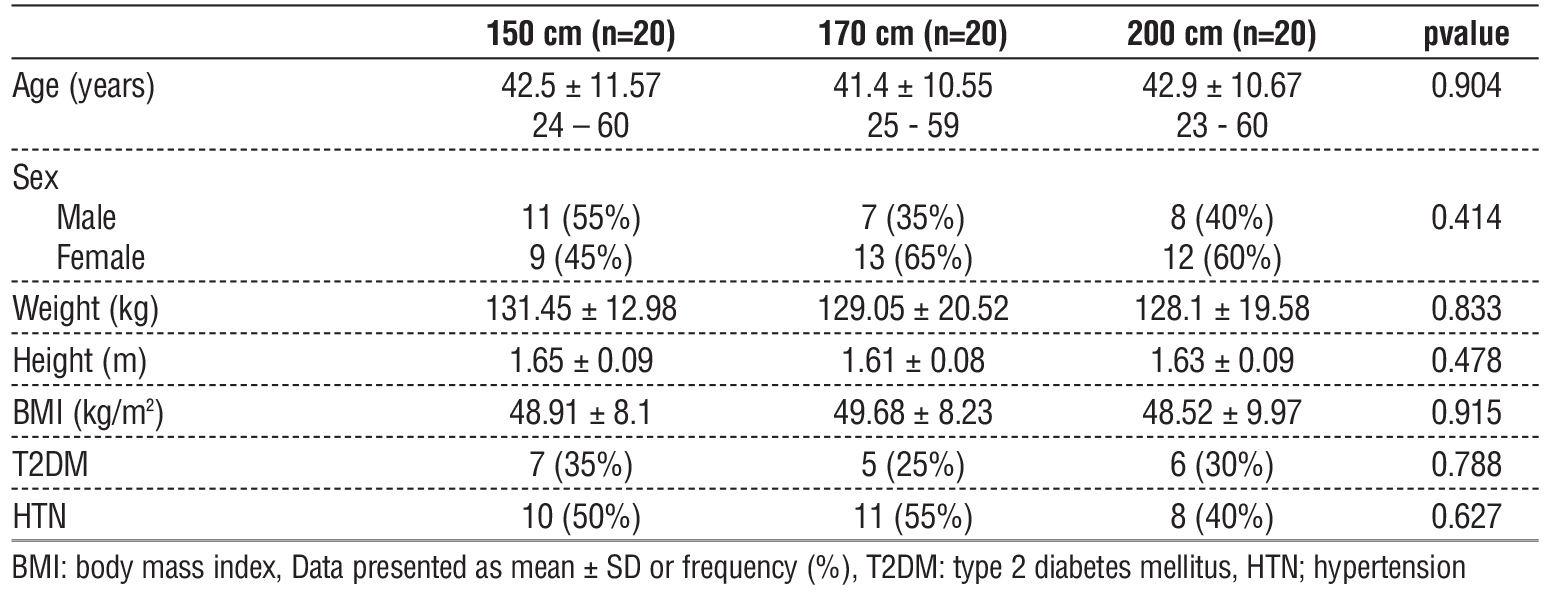
Table 2 - Small bowel length and gastric pouch length of the studied groups

Table 3 - Correlation of small bowel length with weight loss and nutritional deficiencies
Perioperative Events and Complications
One case of small bowel serosal tear occurred during intraoperative measurement, which was repaired with interrupted 3/0 Vicryl sutures; no sub-sequent complications occurred. There was no mortality during the study period.
Five patients developed intraluminal postoperative bleeding, diagnosed based on clinical signs including tachycardia, orthostatic hypotension, oliguria, and a significant drop in hemoglobin. Pelvi-abdominal ultrasound (PAUS) showed no peritoneal collections suggesting luminal bleeding. All cases presented later with melena. They were successfully managed with transfusions of packed red blood cells and plasma. The bleeding occurred in two patients from the 150 cm group, one from the 170 cm group, and two from the 200 cm group.
Five patients experienced persistent epigastric pain and underwent upper endoscopy, which revealed stomal ulceration. All cases were managed conservatively with medical therapy. This occurred in two patients, each from the 150 cm and 170 cm groups, and one from the 200 cm group.
Weight Loss Outcomes
Postoperative weight differed significantly between groups (p = 0.041). Patients in the 200 cm group had significantly lower postoperative weight compared to the 150 cm group (p = 0.032), while no significant differences were found between the 150 cm and 170 cm or the 170 cm and 200 cm groups (table 4).
Table 4 - One-year postoperative weight and BMI, TWL (%), EWL (%) of the studied groups
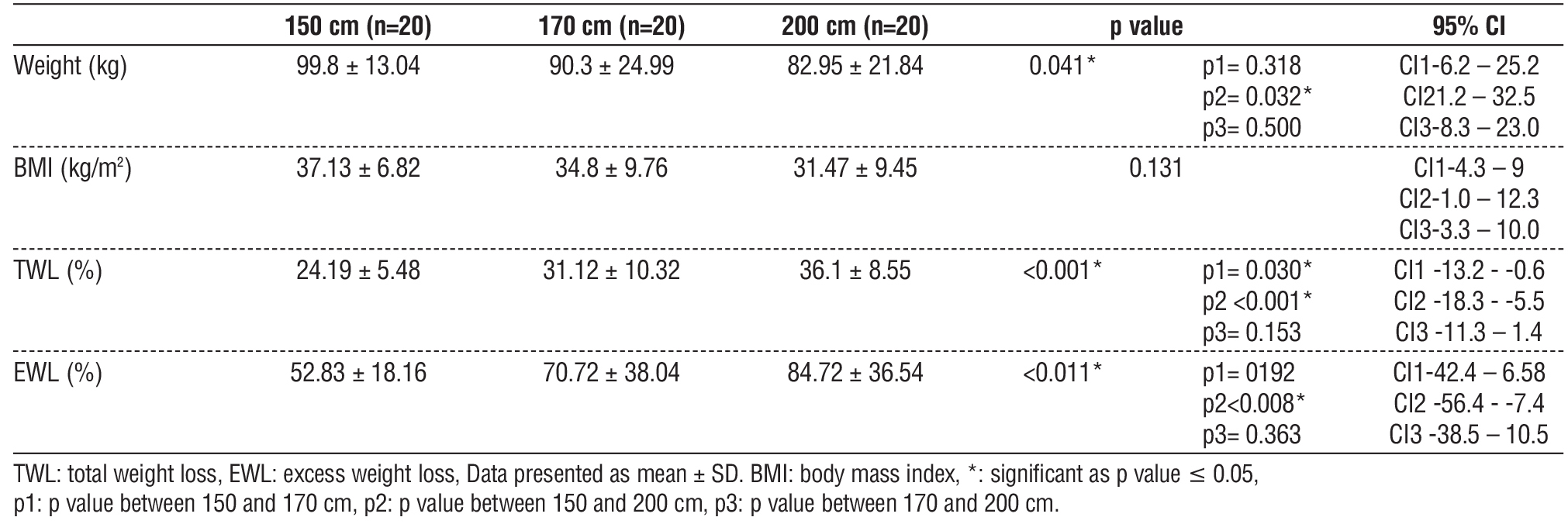
The percentage of total weight loss (%TWL) differed significantly across groups (p < 0.001). Patients in the 150 cm group had significantly lower %TWL compared to the 170 cm (p = 0.030) and 200 cm (p < 0.001) groups. There was no significant difference in %TWL between the 170 cm and 200 cm groups. Excess weight loss (%EWL) also varied significantly (p = 0.011), with the 150 cm group showing significantly lower %EWL than the 200 cm group (p = 0.008). No significant differences were observed between the other pairwise comparisons (table 4).
Correlation Analyses
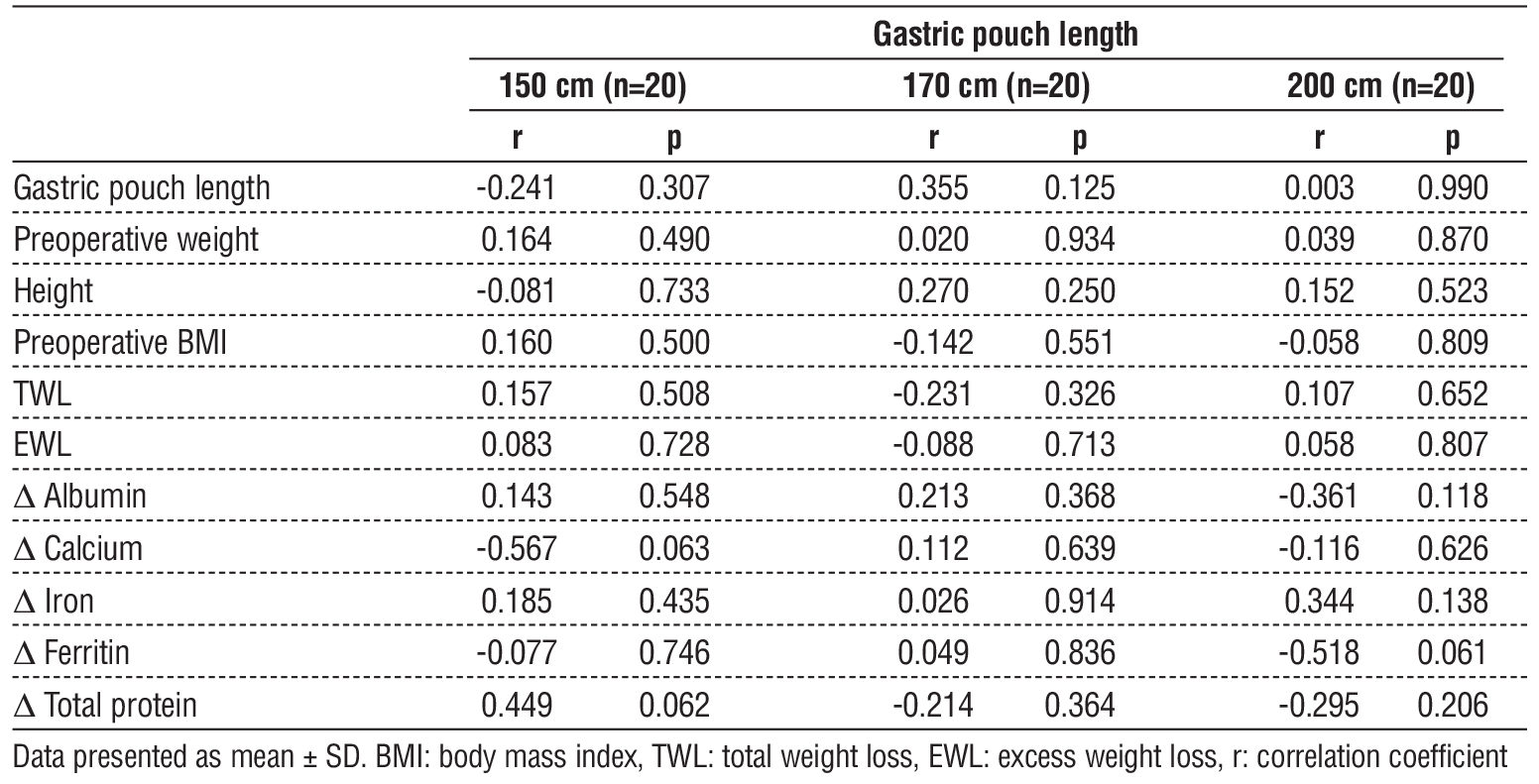
Total small bowel length showed no significant correlation with gastric pouch length, preoperative weight, %TWL, %EWL, or changes in albumin, calcium, iron, ferritin, or total protein across the three groups (table 3). Similarly, gastric pouch length was not significantly correlated with preoperative weight, height, BMI, %TWL, %EWL, or nutritional parameters (table 5).
Table 5 - Correlation of gastric pouch length with weight loss and nutritional deficiencies
Nutritional Parameters
There were no significant intergroup differences in preoperative levels of albumin, calcium, iron, ferritin, or total protein. Postoperatively, albumin and calcium levels showed significant differences among groups (p = 0.005 and p = 0.007, respectively). Deficiencies in albumin and calcium were significantly more common in the 170 cm and 200 cm groups compared to the 150 cm group (p < 0.05 for both), with no significant differences between the 170 cm and 200 cm groups (table 6).
Table 6 - Albumin (g/dL), Calcium (mg/dL) preoperative and one-year postoperative of the studied groups
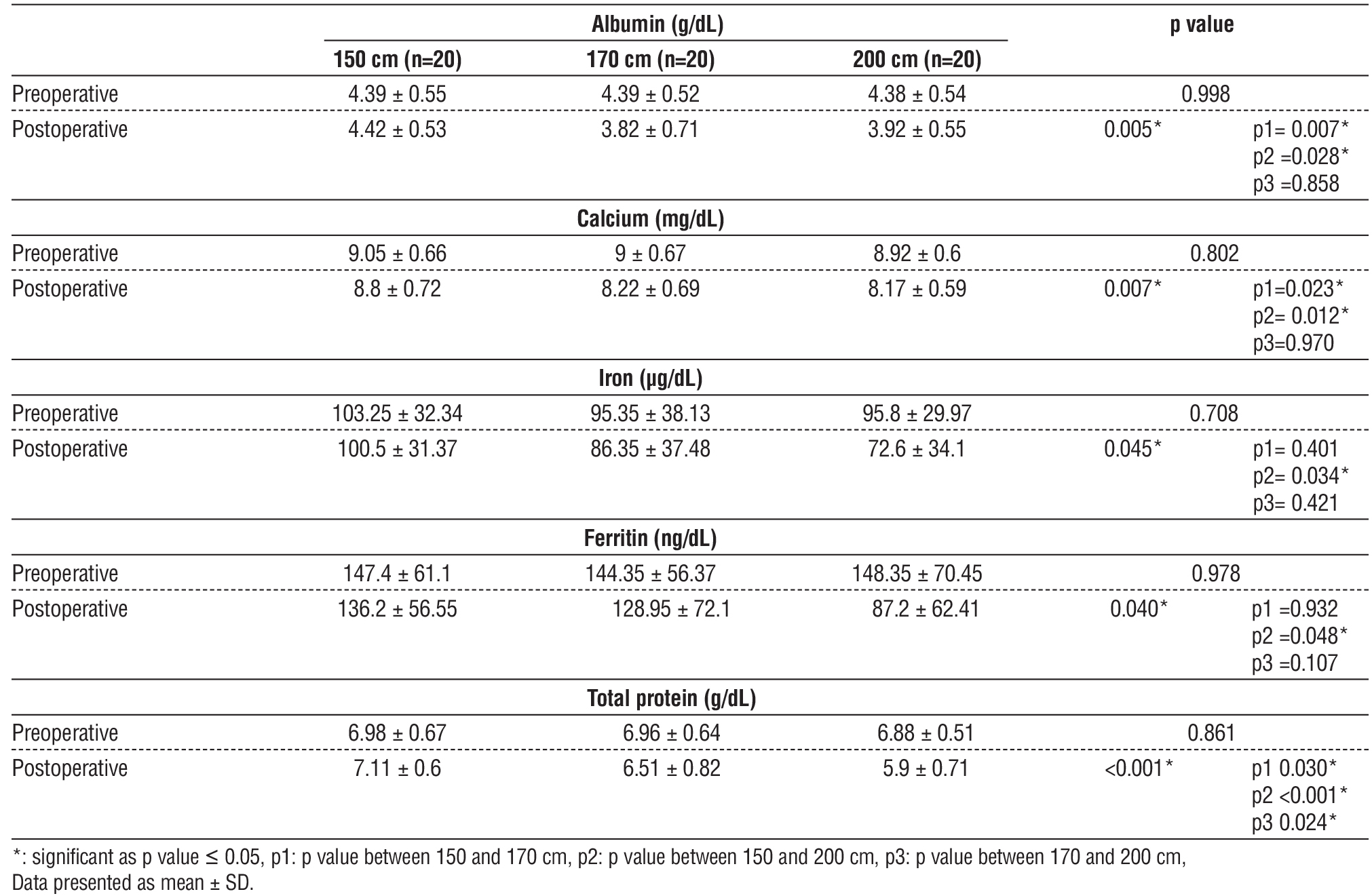
Total protein levels also differed significantly postoperatively (p < 0.001). The 200 cm group had significantly lower total protein compared to both the 150 cm (p < 0.001) and 170 cm (p = 0.024) groups. Additionally, a significant difference was found between the 170 cm and 150 cm groups (p = 0.030).
Iron and ferritin deficiencies were also significantly more prevalent in the 200 cm group (p = 0.045 and
p = 0.040, respectively) compared to the 150 cm group (p < 0.05) (table 6).
Remission of Obesity-Related Comorbidities
At one-year follow-up, no significant differences were observed between groups in the remission rates of T2DM (p = 0.567) and HTN (p = 0.790) (table 7).
Table 7 - Comorbidities resolution of the studied groups

DISCUSSION
Mechanisms and Rationale for Limb Length Variation in OAGB
Procedures combining restriction with hypo-absorption, such as OAGB, are hypothesized to produce superior long-term outcomes compared to purely restrictive surgeries. OAGB achieves this dual mechanism by bypassing a segment of jejunum, which contributes to enhanced weight loss and metabolic improvements but also introduces the risk of nutritional deficiencies (13,14). Since Rutledge’s original description of OAGB (13), multiple bilio-pancreatic limb (BPL) lengths have been explored, including 130 cm to 400 cm (14-39). However, most of these studies are retrospective (8,13,37,38,40), and only a minority count the total small bowel length (SBL) (13,21,34), limiting interpretability.
Limitations of the Tailored Approach
Tailoring BPL length based on BMI, diabetes status, or diet introduces confounding variables that undermine comparative rigor (14). As observed by Charalampos et al. (26), long BPLs (e.g., 200 cm) may paradoxically yield better weight loss outcomes than even longer ones (e.g., 300 cm), likely due to such confounders (38). This study circumvents those limitations by applying randomization and standardi-zation under a single surgeon to ensure unbiased comparison.
Weight Loss Outcomes and Efficacy
Weight loss remains a primary goal in bariatric surgery. Salman et al.’s meta-analysis (8) found superior total weight loss (TWL) with 200-cm BPLs, although excess weight loss (EWL) differences were not statistically significant (8,14). Similarly, Ahuja et al. (16) and Jedamzik et al. (39) reported variable outcomes depending on limb length. In our study, %TWL was significantly lower in the 150-cm group compared to the 200-cm group (24% vs. 36%, p = 0.001), with EWL also significantly lower at 150 cm. These findings reinforce the relationship between extended BPLs and enhanced weight loss.
Nutritional Deficiencies: Albumin and Total Protein
The balance between weight loss and malnutrition is delicate. In our cohort, hypoalbuminemia and total protein deficiency were more common at 170 and 200 cm. This is consistent with findings by Pizza et al. (29), Ahuja et al. (16) and Jedamzik et al. (39), all of whom observed a higher risk of protein malnutrition at longer limb lengths. Alarmingly, Khalaj et al. (26) reported that some cases required reoperation, with one resulting in mortality. Omar et al. (24) also noted higher albumin and multivitamin deficiencies in the 200-cm group. These findings underscore the risk of protein-energy malnutrition (PEM) with extended BPLs.
Calcium and Bone Health Implications
Our results further showed significant calcium deficiency at 170 and 200 cm, despite no baseline differences. Although we did not assess vitamin D, PTH, or bone mineral density (BMD), the literature supports their evaluation (19,41). OAGB bypasses duodenal and proximal jejunal absorption sites, increasing the risk of secondary hyperparathyroidism and skeletal fragility (42). Ahuja et al. (16) documented vitamin D3 deficiency reaching 40% at 250 cm, reinforcing the need for careful monitoring of bone health in longer BPLs.
Gastric Pouch Length: A Neglected Variable
While extensively studied in RYGB (43,44) the influence of gastric pouch length in OAGB is largely unexamined. In our study, no correlation was found between pouch length and weight loss or nutritional status, though all pouches exceeded 15 cm. The MGB-OAGB International Club's consensus supports a minimum pouch length above 15 cm (45). Notably, Wickremasinghe et al. (46) used shorter pouches (as little as 8 cm), which may compromise outcomes by increasing the risk of esophageal biliary reflux, a condition poorly assessed by pH monitoring alone (47,48).
Total Small Bowel Length: Measurement and Implications
Accurate small bowel length (SBL) measurement adds precision to OAGB, although its clinical impact remains controversial. Our data showed no correlation between SBL and outcomes. Literature reports wide variability in SBL (3.5-15 m) (21,27). Despite this, most expert panels, including the MGB-OAGB International Club (45), do not mandate routine SBL counting. However, ensuring a common channel (CC) ? 4 m is recommended to avoid PEM. This is particularly important given the differences in anatomy and function between OAGB and procedures like SADI-S/OADS which requires a CC of 3 m. As SADI-S/OADS has wider gastric sleeve, preservation of the pylorus and proximal duodenum (27,49).
Obesity-Related Comorbidities and Metabolic Resolution
Remission rates for T2DM and HTN did not differ significantly across BPL lengths in our study, consistent with previous findings by Ahuja et al. (16), Salman et al. (8), and Boyle et al. (38). Thus, a shorter BPL limb may suffice for metabolic benefits while minimizing nutritional risks.
Iron and Ferritin Deficiencies
Iron and ferritin deficiencies were significantly more prevalent in the 200-cm group. OAGB patients are known to face higher rates of anemia than those undergoing RYGB (40). Ahuja et al. (16) and Jedamzik et al. (39) agree with our findings, highlighting the susceptibility of women in particular. This again supports limiting BPL length to mitigate hypoabsorptive risks.
Strengths and Limitations
This study is distinguished by several notable strengths. Foremost is its randomized controlled trial (RCT) design, which addresses many of the methodological weaknesses present in prior observational and retrospective studies comparing different BPL lengths in OAGB. Randomization was conducted with rigorous allocation concealment, and all procedures were performed by a single high-volume surgeon using a standardized technique. This uniformity in operative strategy minimizes inter-operator variability, particularly with respect to critical surgical elements such as small bowel measurement, gastric pouch construction, anastomotic technique, and perioperative care. As such, the outcomes observed are more likely attributable to the variable under investigation, BPL length, rather than confounding surgical factors.
Another significant strength lies in the prospective documentation of both anatomical (e.g., small bowel length and gastric pouch length) and clinical outcomes (e.g., weight loss, nutritional status, and metabolic remission). The inclusion of total small bowel length measurements, which are often omitted in comparable studies, adds valuable anatomical context to the observed clinical outcomes. Moreover, this study is among the first to examine the potential relationship between gastric pouch length and postoperative outcomes in OAGB patients, an area that remains underexplored despite its possible implications for reflux, weight loss, and malabsorption.
Nonetheless, the study has important limitations. The sample size, although powered to detect differences in weight loss and nutritional parameters, remains relatively modest and may not capture rare adverse events or long-term trends. A larger cohort would enhance the reliability of subgroup analyses, especially for secondary endpoints such as individual nutrient deficiencies. The single-center nature of the study, while aiding procedural consistency, may also limit the generalizability of the findings to other institutions with different patient populations, dietary habits, or surgical practices.
Additionally, the study's follow-up period is restricted to one year. While early postoperative outcomes are important, the durability of weight loss and the long-term nutritional sequelae of extended BPLs, particularly the development of protein-energy malnutrition, bone disease, and trace element deficiencies, typically manifest beyond the first postoperative year. The study also lacks systematic assessment of micronutrients such as vitamin D, vitamin B12, folate, vitamin A, and parathyroid hormone (PTH), which are critically relevant in MBS patients and known to be affected by variations in absorptive length. Similarly, routine postoperative upper endoscopy, which could have yielded insights into the incidence of biliary reflux or stomal complications, was not incorporated.
Future Directions
Future research should aim to expand upon this work through large-scale, multicenter randomized trials with extended follow-up (? 3-5 years), incorporating standardized assessments of a broader range of micronutrient and hormonal markers, bone mineral density, and quality of life indices. Such studies should also integrate postoperative imaging and endoscopy protocols to better understand anatomical and functional consequences of varying pouch lengths and limb configurations. Comparative studies between fixed BPL lengths and tailored approaches based on total small bowel length or patient phenotype (e.g., BMI, diabetes status, dietary pattern) are especially needed to clarify whether personalized limb lengths offer meaningful advantages over standardized configurations without increasing risk.
Importantly, future studies should assess the cost-effectiveness and clinical utility of routine small bowel length measurement in OAGB. While this study demonstrates the feasibility of accurate bowel measurement without extending operative time or altering surgical setup, the clinical significance of such measurements -particularly when a minimum 4-meter common channel is preserved-remains contentious. Investigating whether counting SBL improves nutritional risk stratification, enhances patient counseling, or influences decision-making regarding surgical reversals would be a valuable addition to the field.
CONCLUSION
This randomized clinical trial provides evidence that shorter BPL lengths, specifically 150 cm from the DJ flexure, in OAGB are associated with comparable, and in some cases superior, postoperative weight loss outcomes and a significantly lower incidence of nutritional deficiencies compared to extended BPL lengths of 170 cm and 200 cm. Although no significant differences were observed in the remission rates of obesity-related comorbidities such as T2DM and HTN across groups, the increasing prevalence of hypoalbuminemia, iron, calcium, and total protein deficiencies in patients with longer BPLs underscores the critical need for cautious limb selection during surgical planning.
These findings support the rationale for favoring a more conservative BPL length to balance efficacy with long-term nutritional safety. Furthermore, while the measurement of total SBL was feasible and reproducible in this study, its routine application during OAGB remains controversial. Additional randomized controlled trials are necessary to determine whether SBL measurement enhances risk stratification or improves clinical outcomes.
Future investigations should prioritize larger, multicenter trials with extended follow-up to validate these findings and determine their generalizability across diverse populations and surgical practices. Longitudinal assessment of micronutrient status, bone health, and quality of life, alongside anatomic evaluations such as endoscopy, will be essential to fully characterize the long-term implications of different BPL configurations. Ultimately, tailoring OAGB to optimize both metabolic outcomes and nutritional safety must remain a central goal in the evolution of bariatric surgical care.
Author’s Contributions
All authors have contributed equally to this manuscript.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding Statement
No funding agency or organization. The used resources are hospital resources applied freely to all types of patients in different departments of the hospital and the hospital management had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the University Research Ethics Committee. The study was registered in a publicly accessible clinical trial registry. All patients included in this study provided informed consent. The study received approval from the Research Ethical Committee REC (approval code: MD-123-2023) and was registered at clinicaltrals.gov with a registration number of NCT06664099.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
1. Zidan MH, Abokhozima A, Gaber MIA, Amgad A, Altabbaa H, El-Masry H, Alokl M, Ali RF, Elmagd AA, Selim A et al: Trends and Practices in Bariatric Surgery in Egypt: Insights on Esophagogastro-duodenoscopy (EGD) Utilization and Surgical Volumes. Obes Surg 2025;35(7):2528-2548.
2. Lin X, Li H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front Endocrinol. 2021;12:706978.
3. WHO - 6 Facts on Obesity (https://www.who.int/news-room/facts-in-pictures/detail/6-facts-on-obesity).
4. AboKhozima A, Zidan MH, Altabbaa H, Selim A, Alokl M, Mourad M, et al. The impact of weight loss after bariatric surgeries on the patient’s body image, quality of life, and self-esteem. Langenbecks Arch Surg. 2025;410(1):24.
5. Angrisani L, Santonicola A, Iovino P, Palma R, Kow L, Prager G, Ramos A, Shikora S, Fiolo F, Harraca JL et al: IFSO Worldwide Survey 2020-2021: Current Trends for Bariatric and Metabolic Procedures. Obes Surg. 2024;34(4):1075-1085.
6. Biter LU, Hart JW, Noordman BJ, Smulders JF, Nienhuijs S, Dunkelgrün M, et al. Long-term effect of sleeve gastrectomy vs Roux-en-Y gastric bypass in people living with severe obesity: a phase III multicentre randomised controlled trial (SleeveBypass). Lancet Reg Health Eur. 2024.38:100836.
7. Gallucci P, Marincola G, Pennestrì F, Procopio PF, Prioli F, Salvi G, et al. One-Anastomosis Gastric Bypass (OABG) vs. Single Anastomosis Duodeno-Ileal Bypass (SADI) as revisional procedure following Sleeve Gastrectomy: results of a multicenter study. Langenbecks Arch Surg. 2024;409(1):128.
8. Salman MA, Salman A, Assal MM, Elsherbiney M, Tourky M, Elewa A, et al. One Anastomosis Gastric Bypass (OAGB) with a 150-cm Biliopancreatic Limb (BPL) Versus a 200-cm BPL, a Systematic Review and Meta-analysis. Obes Surg. 2023;33(6):1846-1856.
9. Aguas-Ayesa M, Yárnoz-Esquíroz P, Olazarán L, Gómez-Ambrosi J, Frühbeck G. Precision nutrition in the context of bariatric surgery. Rev Endocr Metab Disord. 2023;24(5):979-991.
10. Balamurugan G, Sinclair P, Sesby-Banjoh O, Vinod M, Graham Y, Mahawar K. Optimal Bilio-Pancreatic Limb (BPL) Length in One Anastomosis Gastric Bypass (OAGB) Surgery. Curr Obes Rep. 2025; 14(1):14.
11. Perel N, Taha L, Farkash R, Steinmetz Y, Shaheen F, Levi N, et al. Level of Hypoalbuminemia as a Prognostic Factor in Patients admitted to a Tertiary Care Intensive Coronary Care Unit. Cardiol Cardiovasc Med. 2022;6(6):536-541.
12. Omar W, Elhoofy A, Abdelbaky M: Bariatric surgery and its role in the management of metabolic syndrome. Egypt J Surg. 2019;38(2): 257-266.
13. Abdallah E, Emile SH, Zakaria M, Fikry M, Elghandour M, AbdelMawla A, et al. One-anastomosis gastric bypass (OAGB) with fixed bypass of the proximal two meters versus tailored bypass of the proximal one-third of small bowel: short-term outcomes. Surg Endosc. 2022;36(1):328-335.
14. Ibrahim MY, Elshennawy AS, Wassef ATS, Salah A, Hassan AM, Mikhail S. One Anastomosis Gastric Bypass Versus Long Biliopancreatic Limb Roux-en-Y Gastric Bypass. Obes Surg 2022, 32(3):779-785.
15. Omar I, Sam MA, Pegler ME, Pearson EJB, Boyle M, Mahawar K. Effect of One Anastomosis Gastric Bypass on Haematinics, Vitamin D and Parathyroid Hormone Levels: a Comparison Between 150 and 200 cm Bilio-Pancreatic Limbs. Obes Surg. 2021;31(7):2954-2961.
16. Ahuja A, Tantia O, Goyal G, Chaudhuri T, Khanna S, Poddar A, et al. MGB-OAGB: Effect of Biliopancreatic Limb Length on Nutritional Deficiency, Weight Loss, and Comorbidity Resolution. Obes Surg. 2018;28(11):3439-3445.
17. Salman MA, Salman A, Assal MM, Elsherbiney M, Tourky M, Elewa A, et al. One Anastomosis Gastric Bypass (OAGB) with a 150-cm Biliopancreatic Limb (BPL) Versus a 200-cm BPL, a Systematic Review and Meta-analysis. Obes Surg. 2023;33(6):1846-1856.
18. Madhok B, Mahawar K, Hadfield J, Courtney M, Stubbing-Moore A, Koshy S, et al. Haematological indices and haematinic levels after mini gastric bypass: a matched comparison with Roux-en-Y gastric bypass. Clinical obesity. 2018;8(1):43-49.
18. Jedamzik J, Eilenberg M, Felsenreich DM, Krebs M, Ranzenberger-Haider T, Langer FB, et al. Impact of limb length on nutritional status in one-anastomosis gastric bypass: 3-year results. Surg Obes Relat Dis. 2020;16(4):476-484.
20. Noun R, Skaff J, Riachi E, Daher R, Antoun NA, Nasr M. One Thousand Consecutive Mini-Gastric Bypass: Short- and Long-term Outcome. Obes Surg. 2012;22(5):697-703.
21. Slagter N, van der Laan L, de Heide LJM, Jutte EH, Kaijser MA, Damen SL, et al. Effect of tailoring biliopancreatic limb length based on total small bowel length versus standard limb length in one anastomosis gastric bypass: 1-year outcomes of the TAILOR randomized clinical superiority trial. Br J Surg. 2024;111(9): znae219.
22. Slagter N, de Heide LJM, Jutte EH, Kaijser MA, Damen SL, van Beek AP, et al. Outcomes of the One Anastomosis Gastric Bypass with Various Biliopancreatic Limb Lengths: a Retrospective Single-Center Cohort Study. Obes Surg. 2021;31(10):4236-4242.
23. Neuberg M, Blanchet MC, Gignoux B, Frering V: Long-Term Outcomes After One-Anastomosis Gastric Bypass (OAGB) in Morbidly Obese Patients. Obes Surg. 2020;30(4):1379-1384.
24. Omar I, Sam MA, Pegler ME, Pearson EJB, Boyle M, Mahawar K. Effect of One Anastomosis Gastric Bypass on Haematinics, Vitamin D and Parathyroid Hormone Levels: a Comparison Between 150 and 200 cm Bilio-Pancreatic Limbs. Obes Surg. 2021;31(7):2954-2961.
25. Khalaj A, Mousapour P, Motamedi MAK, Mahdavi M, Valizadeh M, Hosseinpanah F, et al. Comparing the Efficacy and Safety of Roux-en-Y Gastric Bypass with One-Anastomosis Gastric Bypass with a Biliopancreatic Limb of 200 or 160 cm: 1-Year Results of the Tehran Obesity Treatment Study (TOTS). Obes Surg. 2020;30(9): 3528-3535.
26. Charalampos T, Maria N, Vrakopoulou VGZ, Tania T, Raptis D, George Z, et al. Tailored One Anastomosis Gastric Bypass: 3-Year Outcomes of 94 Patients. Obes Surg. 2019;29(2):542-551.
27. Nabil TM, Khalil AH, Mikhail S, Soliman SS, Aziz M, Antoine H. Conventional Versus Distal Laparoscopic One-Anastomosis Gastric Bypass: a Randomized Controlled Trial with 1-Year Follow-up. Obes Surg. 2019;29(10):3103-3110.
28. Chakhtoura G, Zinzindohoué F, Ghanem Y, Ruseykin I, Dutranoy J-C, Chevallier J-M. Primary Results of Laparoscopic Mini-Gastric Bypass in a French Obesity-Surgery Specialized University Hospital. Obes Surg. 2008;18(9):1130-3.
29. Komaei I, Sarra F, Lazzara C, Ammendola M, Memeo R, Sammarco G, et al. One Anastomosis Gastric Bypass–Mini Gastric Bypass with Tailored Biliopancreatic Limb Length Formula Relative to Small Bowel Length: Preliminary Results. Obes Surg. 2019;29(9):3062-3070.
30. Pizza F, Lucido FS, D'Antonio D, Tolone S, Gambardella C, Dell'Isola C, et al. Biliopancreatic Limb Length in One Anastomosis Gastric Bypass: Which Is the Best? Obes Surg. 2020;30(10):3685-3694.
31. Lee WJ, Wang W, Lee YC, Huang MT, Ser KH, Chen JC. Laparoscopic mini-gastric bypass: experience with tailored bypass limb according to body weight. Obes Surg. 2008;18(3):294-299.
32. Baksi A, Kamtam DNH, Aggarwal S, Ahuja V, Kashyap L, Shende DR: Should Surveillance Endoscopy Be Routine After One Anastomosis Gastric Bypass to Detect Marginal Ulcers: Initial Outcomes in a Tertiary Referral Centre. Obes Surg. 2020;30(12):4974-4980.
33. Ruiz-Tovar J, Llavero C. Metabolic Effect of the Hepatic Branch of the Vagal Nerve in One-Anastomosis Gastric Bypass (OAGB). World J Surg. 2020;44(6):1939-1944.
34. Zaki KM, Moustafa AA, Shafik YS, Helmy MM: Comparative study between total bowel measurement and proximal bowel measurement in laparoscopic one-anastomosis gastric bypass regarding effect on weight loss and nutritional status. The Egyptian Journal of Surgery 2022, 41(1):105-119.
35. Parmar CD, Bryant C, Luque-de-Leon E, Peraglie C, Prasad A, Rheinwalt K, et al. One Anastomosis Gastric Bypass in Morbidly Obese Patients with BMI ³?50 kg/m2: a Systematic Review Comparing It with Roux-En-Y Gastric Bypass and Sleeve Gastrectomy. Obes Surg. 2019;29(9):3039-3046.
36. Parmar CD, Zakeri R, Mahawar K. A Systematic Review of One Anastomosis/Mini Gastric Bypass as a Metabolic Operation for Patients with Body Mass Index £ 35 kg/m2. Obes Surg 2020;30(2): 725-735.
37. Hussain A, El-Hasani S. Short- and Mid-term Outcomes of 527 One Anastomosis Gastric Bypass/Mini-Gastric Bypass (OAGB/MGB) Operations: Retrospective Study. Obes Surg. 2019;29(1):262-267.
38. Boyle M, Mahawar K. One Anastomosis Gastric Bypass Performed with a 150-cm Biliopancreatic Limb Delivers Weight Loss Outcomes Similar to Those with a 200-cm Biliopancreatic Limb at 18 -24 Months. Obes Surg. 2020;30(4):1258-1264.
39. Jedamzik J, Eilenberg M, Felsenreich DM, Krebs M, Ranzenberger-Haider T, Langer FB, Prager G: Impact of limb length on nutritional status in one-anastomosis gastric bypass: 3-year results. Surg Obes Relat Dis 2020, 16(4):476-484.
40. Hussain A, Van den Bossche M, Kerrigan DD, Alhamdani A, Parmar C, Javed S, et al. Retrospective cohort study of 925 OAGB procedures. The UK MGB/OAGB collaborative group. Int J Surg; 2019;69:13-18.
41. Nawar AM, Baumy M, Eid A, Mohamed AT. Effect of laparoscopic mini gastric bypass versus laparoscopic single anastomosis sleeve ileal bypass on serum iron and calcium levels. Egypt J Surg. 2024; 43(2):524-533.
42. Wei JH, Lee WJ, Chong K, Lee YC, Chen SC, Huang PH, et al. High Incidence of Secondary Hyperparathyroidism in Bariatric Patients: Comparing Different Procedures. Obes Surg. 2018;28(3):798-804.
43. Safari S, Ekramnia I, Chehresonboll Y, Ahmadi V, Kermansaravi M. Outcomes and complications after long versus short gastric pouch Roux-en-Y gastric bypass in patients with severe obesity. Sci Rep. 2024;14(1):31012.
44. Ammar M, Ibrahim AI, Aly MA, Eltaia M, Zidan MH. Roux-en-Y Gastric Bypass: Revisiting Gastric Pouch Length Variability in Search of Consensus. Obes Surg. 2025;35(3):1197-1198.
45. Bhasker AG, Prasad A, Shah S, Parmar C, Contributors O-MGBC: MGB-OAGB International Club - Results of a Modified Delphi Consensus on Controversies in OAGB. Obes Surg. 2024;34(12): 4541-4554.
46. Wickremasinghe AC, Leang YJ, Johari Y, Laurie C, Nadebaum D, Yue H, et al. Modified One Anastomosis Gastric Bypass Following Sleeve Gastrectomy for Severe Reflux and Delayed Gastric Emptying: A Prospective Trial with Clinical and Physiological Outcome Measures. Obes Surg. 2024;34(8):2940-2953.
47. Roman S, Gyawali CP, Savarino E, Yadlapati R, Zerbib F, Wu J, et al. Ambulatory reflux monitoring for diagnosis of gastroesophageal reflux disease: Update of the Porto consensus and recommendations from an international consensus group. Neuro-gastroenterol Motil. 2017;29(10):1-15.
48. Zikos TA, Clarke JO: Non-acid Reflux: When It Matters and Approach to Management. Curr Gastroenterol Rep. 2020;22(9):43.
49. Kermansaravi M, Shahmiri SS, Davarpanah Jazi AH, Valizadeh R, Weiner RA, Chiappetta S. Reversal to normal anatomy after one-anastomosis/mini gastric bypass, indications and results: a systematic review and meta-analysis. Surg Obes Relat Dis. 2021; 17(8):1489-1496.
Full Text Sources:
Abstract:
Views: 673

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.