Surgery, Gastroenterology and Oncology

|
|
Background: anastomotic leakage stays one adverse post-operative complication for gastrointestinal surgeons either regarding its prevention or its early diagnosis. Anastomotic leakage may lead to prolonged hospital stay, increased morbidity and mortality from ensuing sepsis. Purpose: to evaluate the value of using bilirubin concentration in serum and the peritoneal drain fluid as predictive biomarkers for anastomotic leakage.
Material and Methods: this prospective cohort study was conducted at the department of Surgery, Kasralainy School of Medicine, Cairo University on 200 patients with colorectal, ileo-colic, intestinal and gastrointestinal anastomoses in the peroid from July 2021 to June 2022.
Results: the overall incidence of anastomotic leakage was 9.5% (19/200). In patients with leakage, a significant rise in serum bilirubin, drain fluid bilirubin level, and drain to serum ratio were observed. Receiver operating characteristic analysis of serum bilirubin showed sensitivity for anastomotic leakage ranging from 10.5% to 57.9%, and specificity ranging from 90.1% to 100%. Receiver operating characteristic analysis of drain fluid bilirubin level showed a sensitivity for anastomotic leakage ranging from 80%to100%, and specificity ranging from 97.6% to 100%. Higher risk of leakage was associated with co-existing morbidities, emergent procedures, and hand sewing with p-value 0.045, 0.003 and 0.012 respectively.
Conclusion: serum bilirubin at the first 5 postoperative days can be used as a good positive test to diagnose anastomotic leakage in patients with non-specific postoperative clinical symptoms. The drain fluid-to-serum bilirubin ratio and drain fluid bilirubin level are predictive biomarkers of anastomotic leakage.
INTRODUCTION
Anastomotic Leakage (AL) has been a longstanding post-operative complication in gastrointestinal intestinal surgery for decades (1,2).
Early diagnosis of anastomotic leakage is universally needed as the first step towards early management aiming to prevent adverse complications up to mortality from sepsis (3). Noting that each hour of delay in administration of antibiotics from the onset of septic shock is associated with 7.5% decrease in survival (4). Predictive biomarkers to detect AL are subject of research and due to the ensuing morbidity and the high rate of mortality, these biomarkers are urgently required (3). The nonspecific postoperative clinical signs and inflammatory markers may lead to unneeded interventions misleading the clinician from the problem itself (postoperative pulmonary complications, urinary tract infections or venous thrombo-embolism) or the reverse referring the elevated markers for the above-mentioned causes delaying the diagnosis of AL (3,5,6).
Many studies and reviews have studied many markers for early identification of anastomotic leakage. However, few were prospective with sufficient sample size (1,2,7-9). In addition, the majority of these studies focuses only on colorectal anastomoses (1,2,7,10,11) making use of its conclusions on other anastomoses like gastrojejunostomies, jejunojejunostomies or ileocolic anastomoses not applicable. Also, many studies lack standardized AL definition and grading (12).
Our study estimates bilirubin level in serum and the drain fluid (DF) are biomarkers for early diagnosis of bowel leakage.
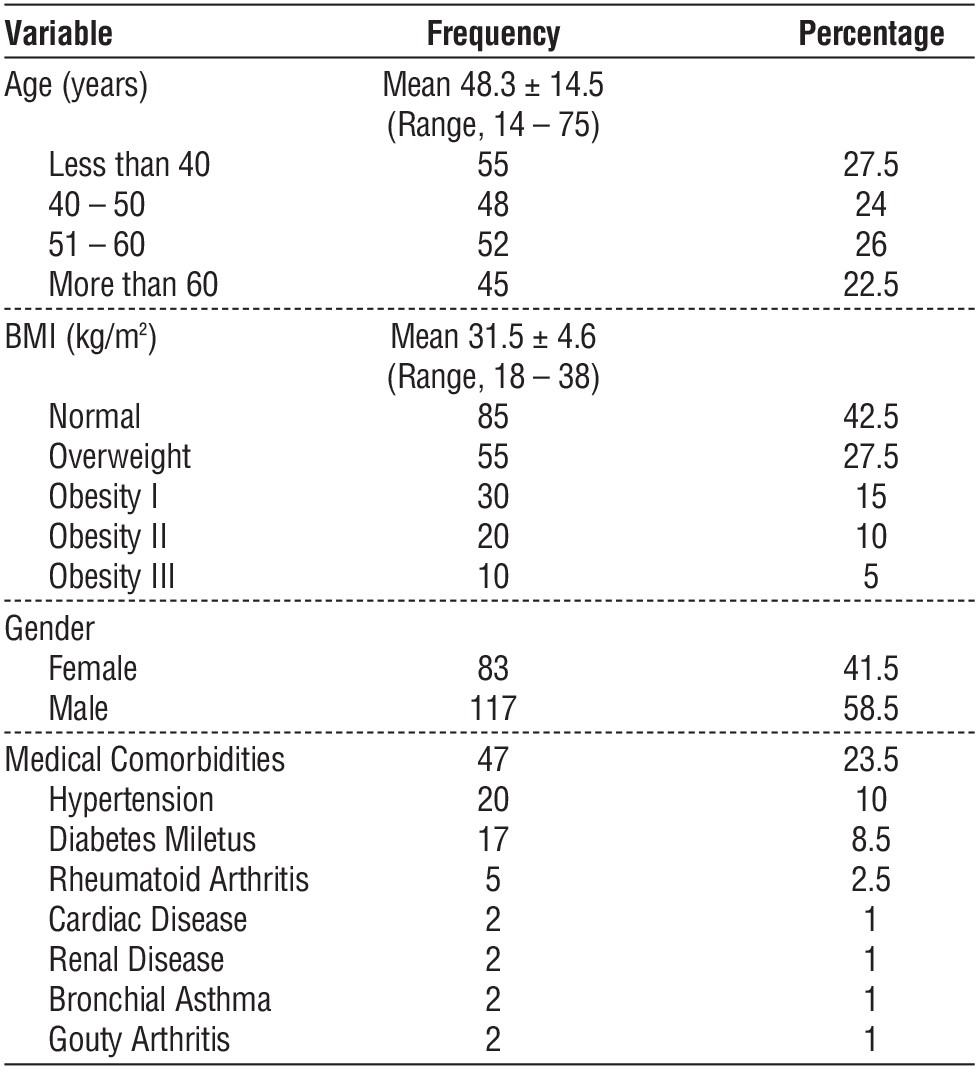
Table 1 - Baseline demographic data (n = 200)
MATERIALS AND METHODS
Study Design
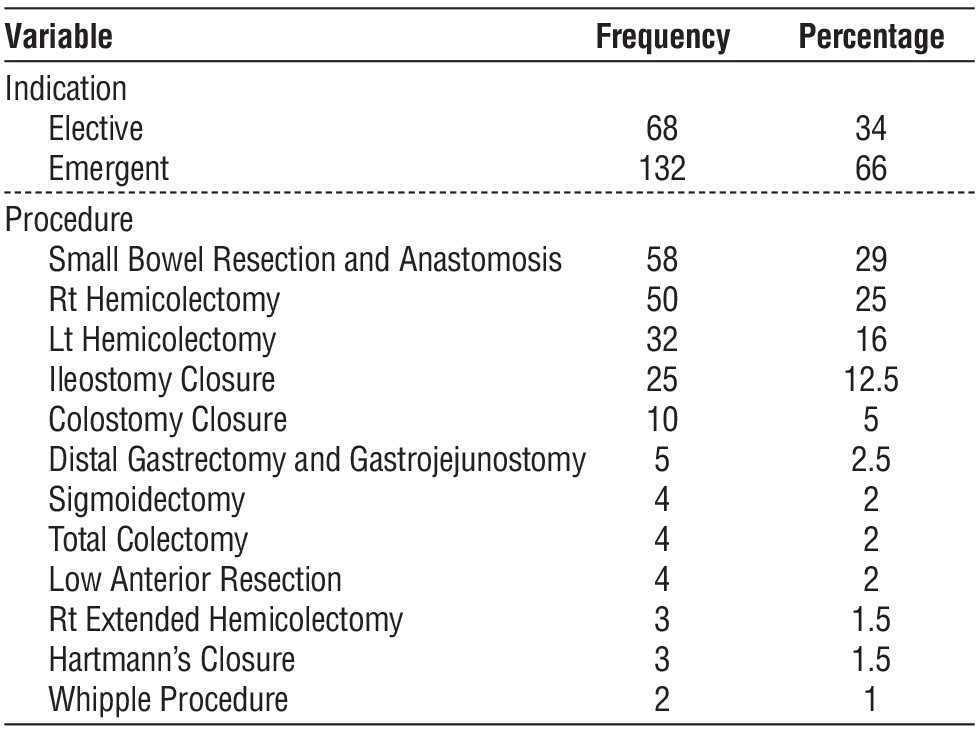
This cohort prospective study was conducted on 200 patients with colorectal and intestinal anastomoses in the general surgery, colorectal and emergency departments at the Department of Surgery, at Kasralainy School of Medicine, Cairo University, a tertiary health care hospital, in the period from July 2021 to June 2022 as illustrated in tables 1 and 2.
Table 2 - Surgical data (indication, Type of procedure, mode of anastomosis)(n = 200)
Inclusion Criteria
Resection and anastomosis (emergency & elective) for any part of the gastrointestinal tract (stomach, small and large bowel).
Exclusion Criteria
The following cases were excluded (patients receiving neoadjuvent chemotherapy, those having a protective proximal stoma, those with preoperative jaundice, subclinical hyperbilirubinemia or liver failure, those having bogota bag bridging an open-abdomen wound, those receiving or planned to receive immediate postoperative total parental nutrition, patients with lesions requiring concomitant liver resection, and traumatic cases requiring bowel resection).
All patients received an intra-abdominal tube drain which was placed near, but not touching, the anastomosis. And the drain was left for al least 5 days.
Type of the drain: Nelaton drain (EUCEREP, Roald Dahllaan 33, 5629MC-Eindhoven, The Netherlands).
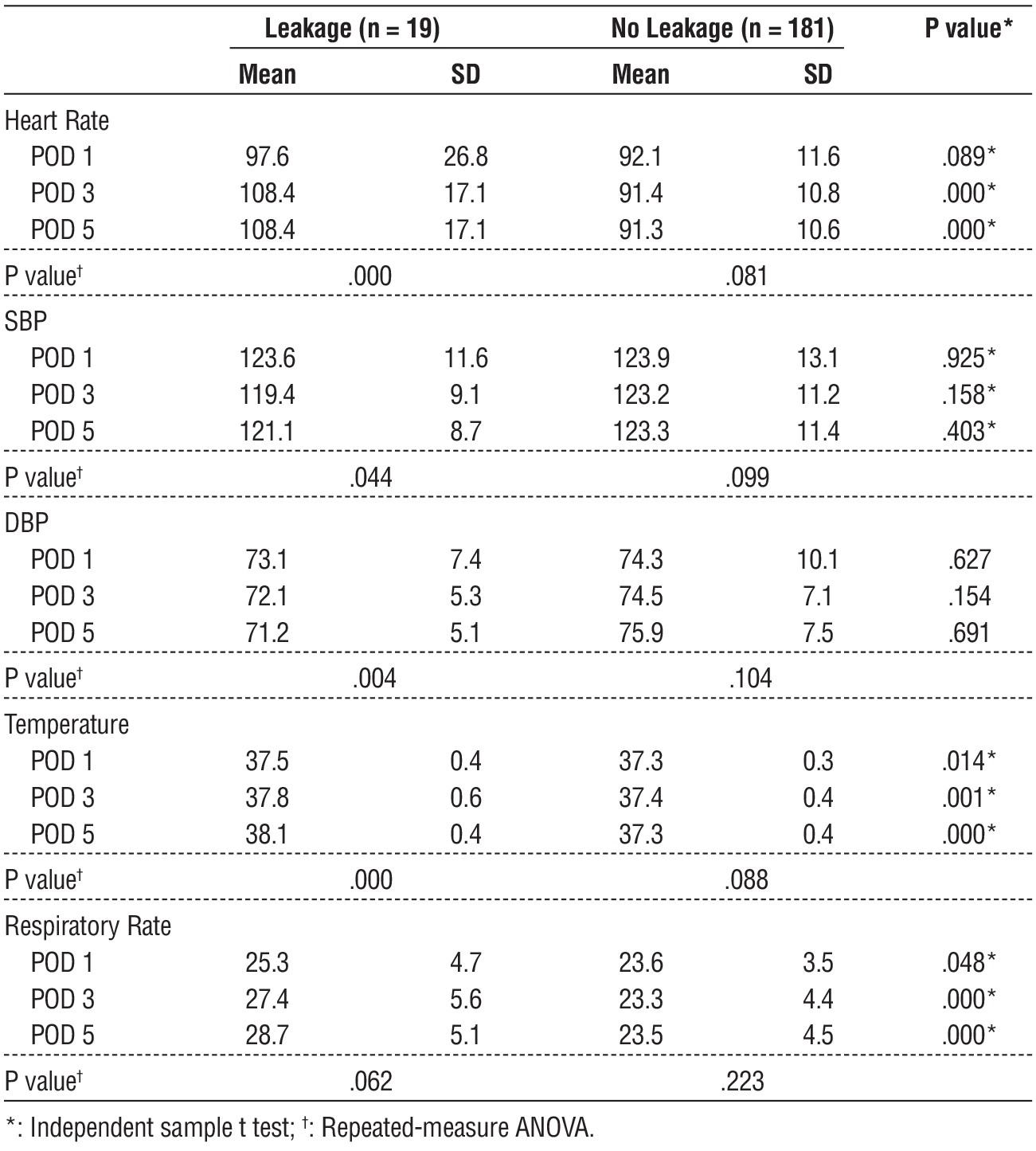
Demographic data, postoperative vital signs (temperature, pulse rate, blood pressure and respiratory rate) were recorded (tables 1 and 3).
Table 3 - Comparing vital measurements in leakage and no leakage patients
Daily general and local examination was performed, suspected cases of leakage underwent post-contrast abdomino-pelvic computed tomography scan.
Leakage was defined a connection between intra-luminal and extraluminal spaces through a defect in a site of anastomosis and was classified into three grades according to the management plan needed, grade A requiring no interventions, grade B requiring interventions but not re-explorations, and grade C requiring re-explorations (13).
The drain fluid was sampled once a day with intervals of 24 hours until the 5th postoperative day at least, under complete aseptic conditions and the collecting bag is then exchanged with a new one. Serum total bilirubin was measured at the same time.
Total bilirubin was measured by using the third generation Bilirubin Total assay.
Post-operative basic labs (CBC, CRP, albumin, AST, ALT) were recorded on POD 1,3,5.
The Primary outcomes are to measure sensitivity and specificity of bilirubin level in serum and in drain fluid for detection of bowel anastomosis leakage.
Statistical Analysis
The collected data was revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). Data was presented and suitable analysis was done according to the type of data obtained for each parameter.
Kolmogorov–Smirnov test was used to evaluate normal distribution of continuous data. Mean, Standard deviation (± SD), and range was used for numerical data, while frequency and percentage were used for non-numerical data.
Independent sample t test was used to assess the statistical significance of the difference between two study group means. Mann Whitney Test (U test) was used to assess the statistical significance of the difference of a non-parametric variable between two study groups. Correlation analysis (using Spearman / Pearson's method): to assess the strength of association between two quantitative variables. The correlation coefficient denoted symbolically "r" defines the strength and direction of the linear relationship between two variables. Chi-Square test was used to examine the relationship between two qualitative variables. The ROC Curve (receiver operating characteristic) provides a useful way to evaluate the Sensitivity and specificity for quantitative Diagnostic measures that categorize cases into one of two groups. ANOVA with repeated measures was used for normally distributed quantitative variables, to compare between more than two periods.
For all above mentioned statistical tests done, the threshold of significance is fixed at 5% level (P-value):
P value of > 0.05 indicates non-significant results,
P value of < 0.05 indicates significant results and P value of < 0.01 indicates highly significant results
RESULTS
Patients complicated with anastomotic leakage had significantly higher leucocytic count, CRP levels, and lower albumin levels (Independent sample t test, P < .05) as illustrated in table 4.
Table 6 compares bilirubin measurements between patients presented with leakage and patients who did not. A statistically significant difference was found between the two groups regarding drain fluid bilirubin (POD 1-5), serum bilirubin (POD 4-5), and drain fluid-to-serum bilirubin ratio (POD 1-5). Patients complicated with anastomotic leakage had significantly higher drain fluid bilirubin and drain to serum bilirubin ratio (Independent sample t test, P < .05). In patients with leakage, a significant rise in serum bilirubin (POD 4-5), drain fluid bilirubin, and drain-to-serum ratio were observed from POD 1 to POD 5 (Repeated measure ANOVA, P < .05).
Table 4 - Comparing laboratory measurements in leakage and no leakage patients
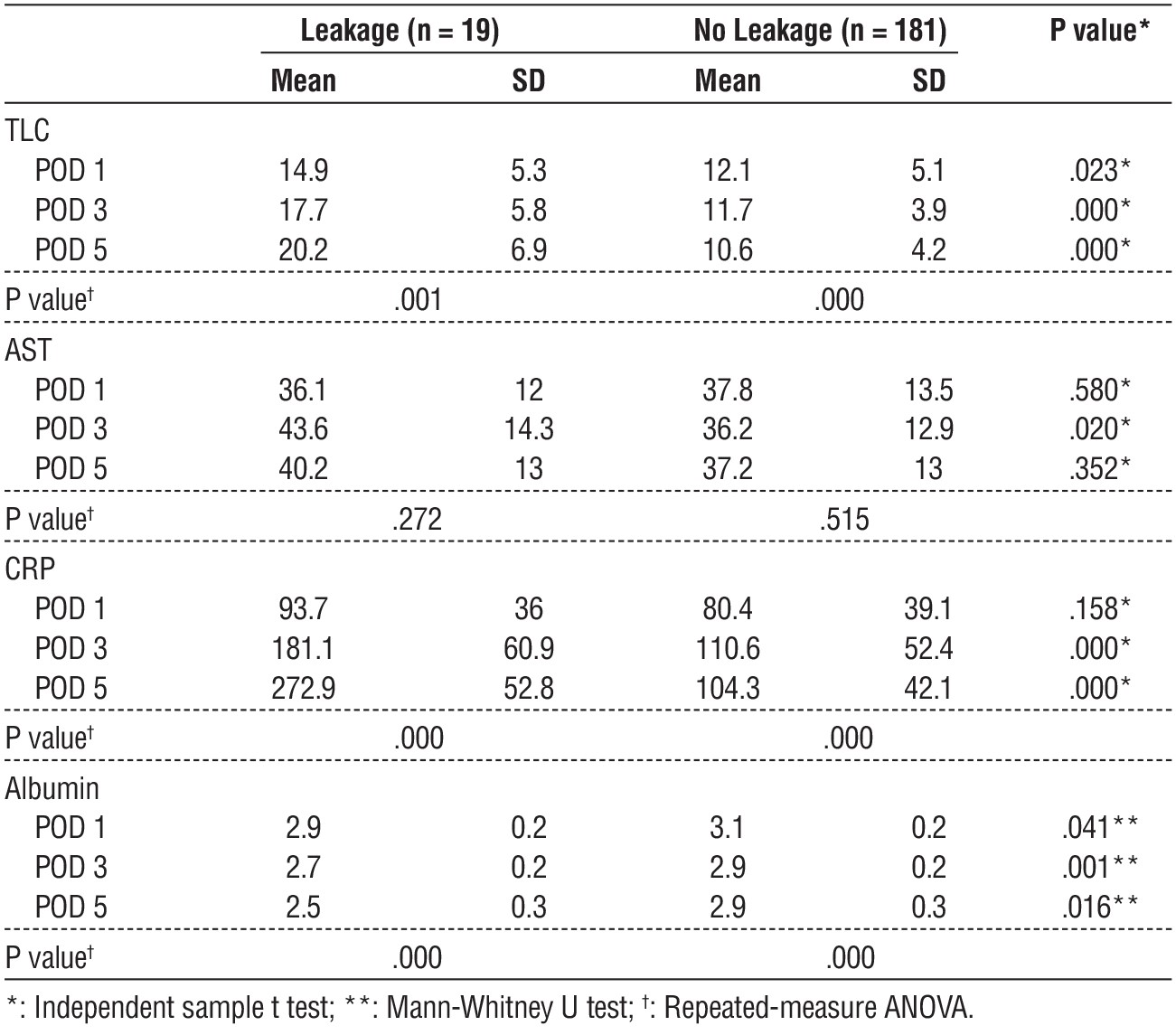
Table 5 - Serum and drain fluid bilirubin (n = 200)
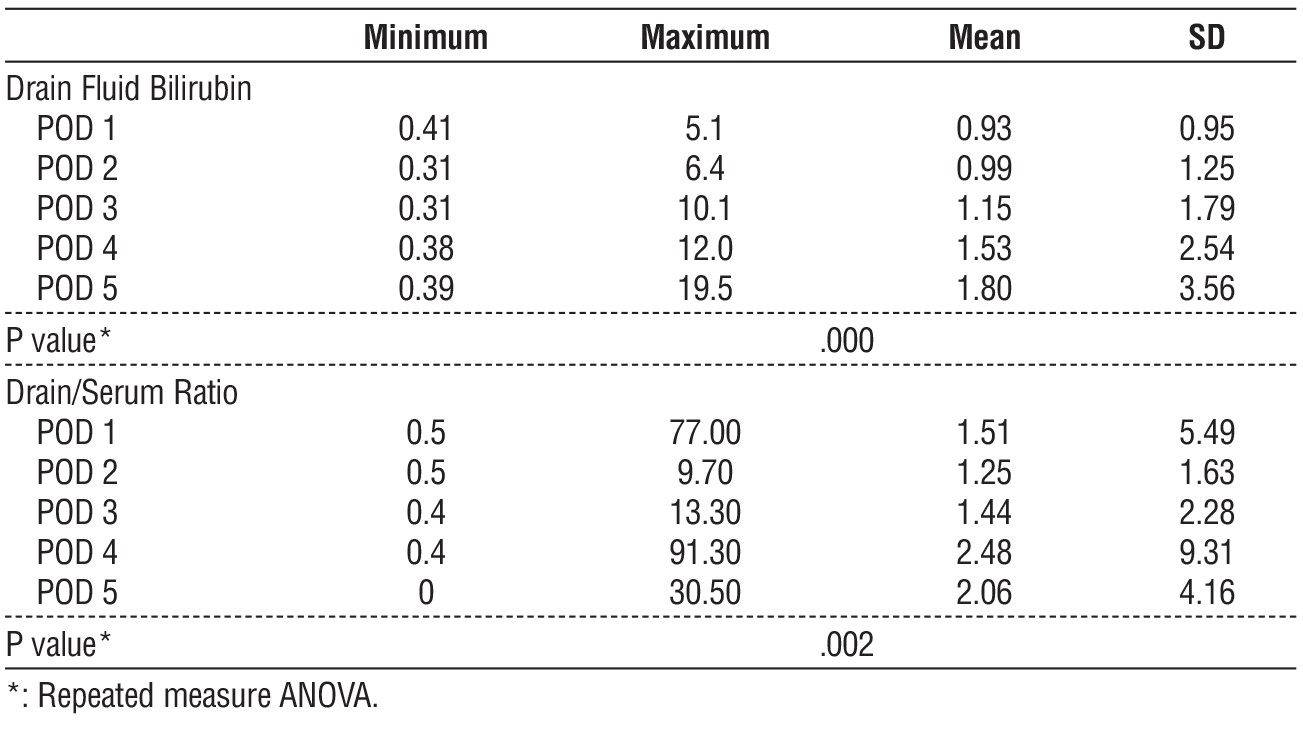
Table 6 - Comparing serum and drain fluid bilirubin in leakage and no leakage patients
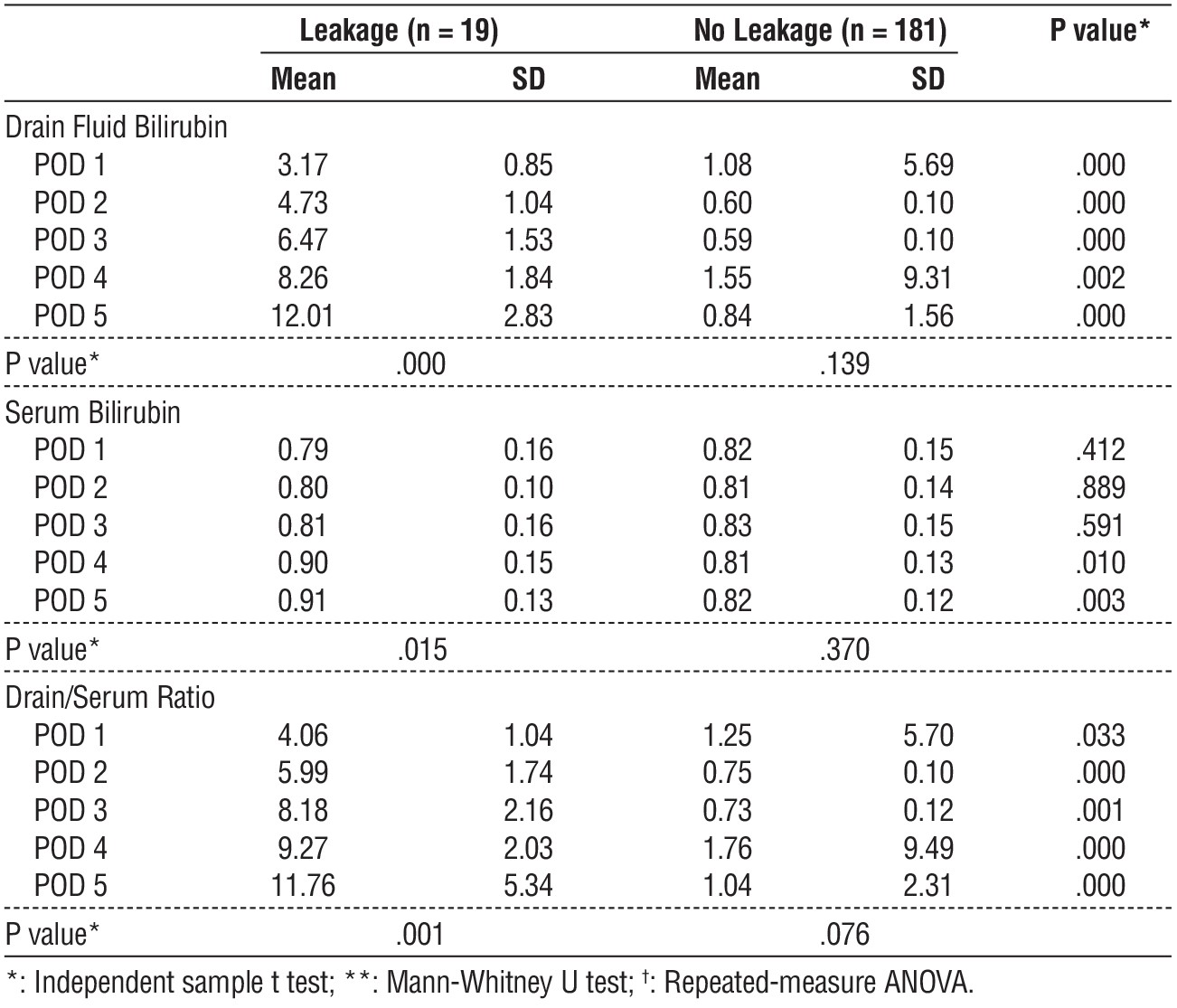
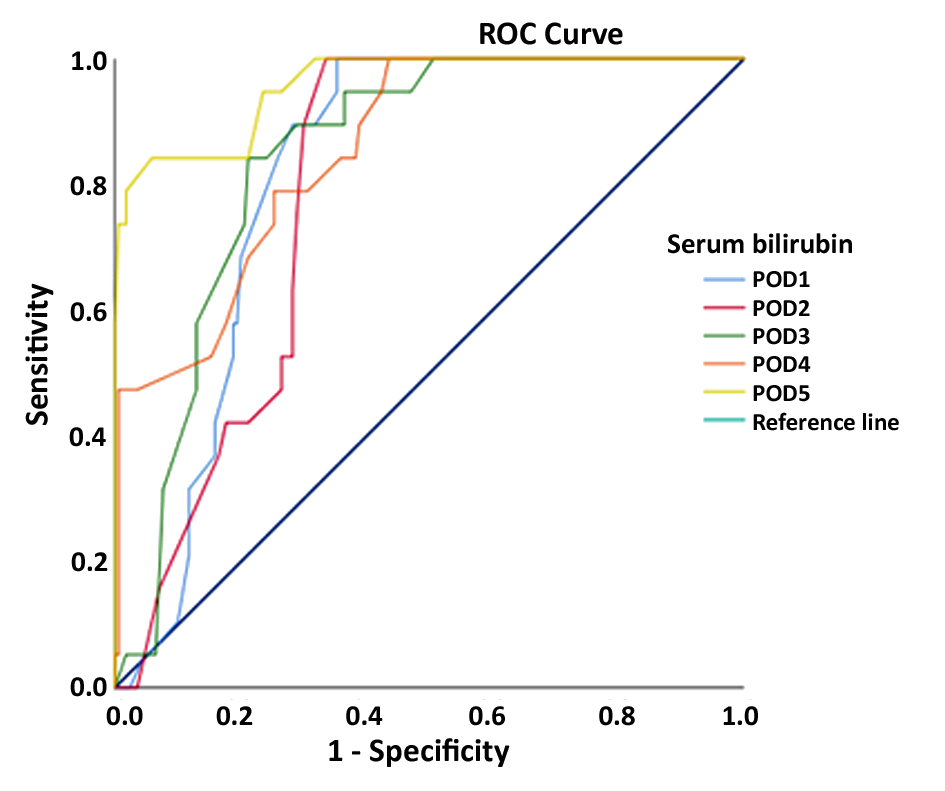
Table 7 showed that a receiver operating characteristic (ROC) analysis was carried out to demonstrate the leakage predictive value of serum bilirubin. Serum bilirubin was found to be a good predictive test on POD 1 to 5, with a sensitivity ranging from 10.5% to 57.9%, and specificity ranging from 90.1% to 100%.
Table 7 - Receiver operating characteristic (ROC) analysis of serum bilirubin values
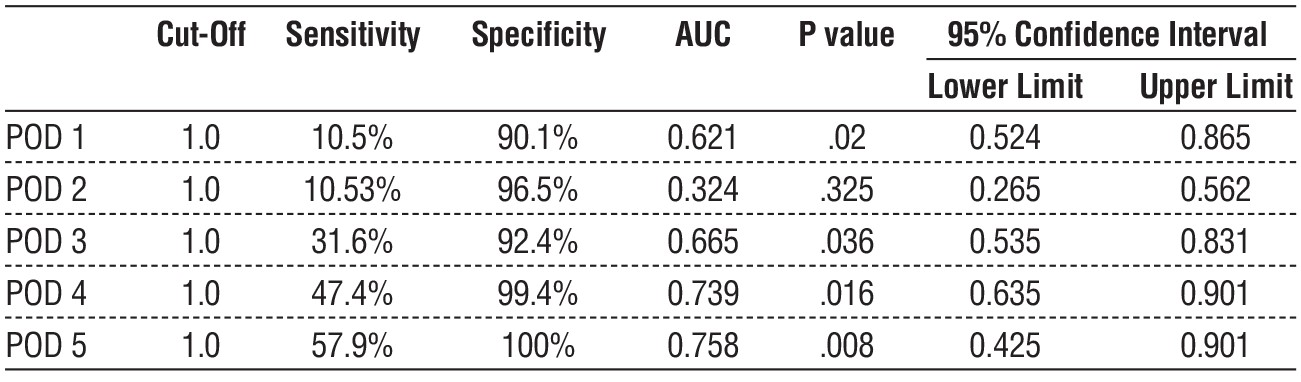
Table 8 - Correlation analysis of leakage risk factors (n = 200)
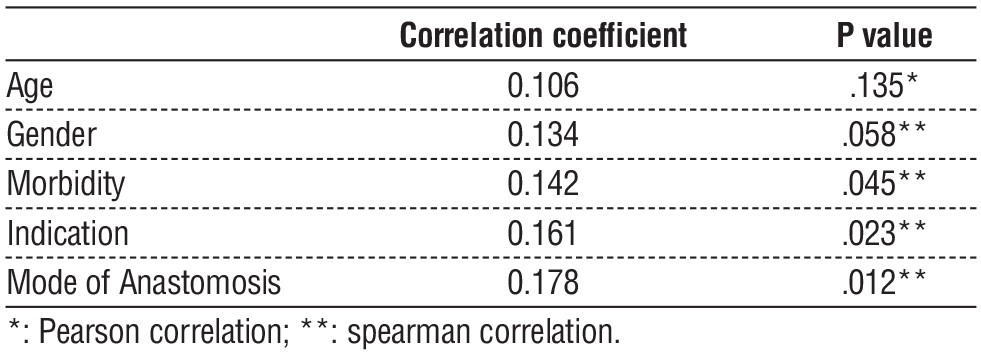
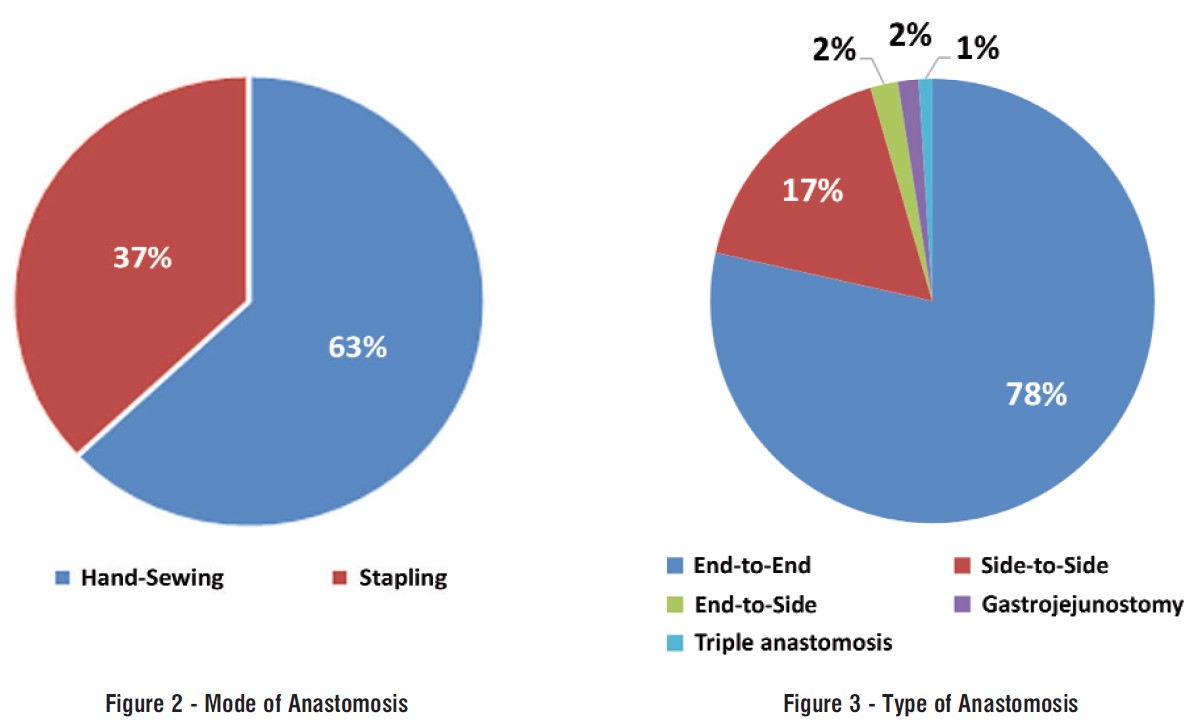
Table 8 and fig. 1 showed that a correlation analysis between anastomotic leakage and different risk factors identified in our cohort. A statistically significant correlation was found between leakage as a dependent variable and morbidity, indication, and method of anastomosis (figs. 2 and 3) as independent variables. Therefore, higher risk of anastomotic leakage was associated with medical comorbidities, emergent procedures, and hand sewing.
Figure 1 - ROC analysis of serum bilirubin
DISCUSSION
In the present study we found that the overall incidence of anastomotic leakage was 9.5% (19 cases) as illustrated in table 2.
In emergent procedures, the incidence of leakage was 12.9%, whereas the incidence of leakage in elective procedure was 2.9%. A statistically significant difference was found between emergent and elective procedure regarding rate of leakage (Chi-square test, P = .000).
The mean time of leakage diagnosis (by CT scan and/or re-exploration) was 6.1 ± 1.6 days. In emergent procedures, the mean leakage time was 5.9 ± 1.5 days. No statistically significant difference was found between emergent and elective procedures regarding time of leakage (Independent sample t test, P = .067).
Also, our results were in line with Parthasarathy et al. who reported that the incidence of anastomotic leakage was 3.9% (687/17 518). Although the overall incidence of leakage is lower than our study, when analyzing its results, we found that most of the cases were elective cases. when looking for emergent cases, we found that AL represented 9.5% (11/116), 7.9 % (19/240), 8% (11/137) when the primary indication of surgery was bleeding, malignant neoplasm and perforation of intestine respectively (14).
Bakker et al. reported that incidence of anastomotic leakage was 7.5% (1176/15667). The study also revealed that a statistically significant difference was found between emergent and elective procedure regarding rate of leakage (Chi-square test, P < .001) (15).
Comparison of bilirubin measu-rements between patients presented with and without leakage showed that there was a statistically significant difference between the two groups regarding drain fluid bilirubin (POD 1-5), serum bilirubin (POD 4-5), and drain fluid to serum ratio (POD 1-5). Patients complicated with anastomotic leakage had significantly higher drain fluid bili-rubin and drain-to-serum bilirubin ratio (Independent sample t test, P < .05). In patients with leakage, a significant rise in serum bilirubin (POD 4-5), drain fluid bilirubin, and drain to serum ratio were observed from POD 1 to POD 5 (Repeated measure ANOVA, P < .05). On the other hand, patients without leakage did not demonstrate significant changes in serum bilirubin, drain fluid bilirubin, and drain-to-serum ratio from POD 1 to POD 5 (Repeated measure ANOVA, P > .05).
Our results were supported by Aziz et al. This was prospective controlled study of 10 AL patients vs 20 controls (no leak group) following laparoscopic total colectomy with ileorectal anastomosis for familial adenomatous polyposis who revealed that there was a significant difference between the AL and no-AL groups regarding serum bilirubin (p=0.008), heart rate (p=0.001) and respiratory rate (p=0.017) (8). Similar to our study, all patients with AL were candidates for re-laparotomies (Grade 3 AL). In contrast to our results and many other studies (2,3,5-7,11,14) inflammatory markers (TLC, CRP, Albumin) and temperature were not statistically different in both groups (8).
Also, in agreement with our results Paasch et al. 100 patients, who underwent different types of colectomies with colorectal or colocolic anastomoses were included in prospective clinical trial. During the first four postoperative days (POD) the concentration of bilirubin in the DF was measured and revealed a significant increase than those of the control group on the 1st POD (p = 0.031) and on the 3rd POD (p = 0.041)(2). Similar to our study, all the six patients with AL were re-explored (Grade 3 AL)(3).
Five hundreds and forty-six patients underwent laparoscopic-assisted radical right hemicolectomy in Peking Union Medical College Hospital from 2010 to 2016 and were analyzed in a retrospective clinical trial. Increased concentration of amylase and bilirubin in the DF of four patients, who suffered from AL (9). Among 546 patients, 8(1.5%) cases developed anastomotic leakage with mean age of (54.3±10.3) years. Amylase and bilirubin in DF of 4 patients increased significantly. All the 8 AL patients were having grade 3 AL and underwent secondary ileostomies during the re-exploration (9).
This is the first study to assess the drain-to-serum bilirubin ratio in bowel anastomotic leakage (tables 9 and 5). This quotient is important to avoid the effect of individual normal variations in serum bilirubin (3).
Table 9 - Receiver operating characteristic (ROC) analysis of drain fluid-to-serum bilirubin ratio
In the present study receiver operating characteristic (ROC) analysis was carried out to demonstrate the leakage predictive value of serum bilirubin. Serum bilirubin was found to be a good predictive test on POD 1 to 5, with a sensitivity ranging from 10.5% to 57.9%, and specificity ranging from 90.1% to 100% (table 7 and fig. 1).
Regarding drain bilirubin, ROC analysis showed that drain bilirubin was found to be an excellent predictive test on POD 1 to 5, with a sensitivity ranging from 80% to 100%, and specificity ranging from 97.6% to 100% (table 10). In the current study we found that at 1st and 5th POD drain bilirubin have the best diagnostic accuracy. At second and the third POD drain bilirubin has perfect diagnostic accuracy (AUC = 1). Also, at 4th POD drain bilirubin has diagnostic accuracy (AUC = 0.989). To our knowledge there were no studies in literature have performed ROC curve analysis for these markers.
Table 10 - Receiver operating characteristic (ROC) analysis of drain fluid bilirubin values
Although prophylactic peritoneal drainage value to drain post-operative hematomas, infections and to diagnose leakage is debatable after elective GIT surgery (16), it is still up to the discretion of the surgeon especially in emergency surgery (11,17).
Limitations of Study
Limitations of our study includes:
1. The conclusion of the study is not applicable for cases expected to have post-operative hyperbilirubinemia from any other cause apart from leakage and peritoneal absorption of the leaked bilirubin (please refer to the exclusion criteria on the methodology section).
2. Need for drain regarding drain-to-serum bilirubin ratio so it is not applicable for many patients not having peritoneal drains after GIT anastomoses. However, our finding that serum bilirubin is a
predictive biomarker for AL is still applicable in these patients.
3. Need for larger number of patients to conclude the value of this study in all types of GIT anastomoses.
4. The need for a 100% sensitive and 100% specific predictive biomarker is not met yet and further research is needed.
CONCLUSION
The current study showed that serum bilirubin and drain-to-serum ratio, drain fluid bilirubin at the first 5 days postoperatively can be used as cheap, available potential biomarkers for bowel anastomotic leakage. Anastomotic leaks can be detected early providing an opportunity for early management to salvage the anastomosis and to avoid the dreadful sepsis. Serum bilirubin may be used as a good negative test to exclude AL (in the first 5 POD) in patients not having peritoneal drains making this helpful for patients receiving (no tubes) or FAST TRACT GIT surgery.
Conflict of Interest
All author declare that they have no conflict ofinterest.
Funding
Kasralainy hospital resources (part of Cairo University Hospitals) were the source of funding. The hospital administration has had no role in this study starting from the study idea, data collection, data interpretation till manuscript writing and submission.
Ethical Approval
The study was approved by the research ethical committee according to the ethical standards of the Helsinki Declaration of 1975 in June 2022, code number: ms-78-022. All patients gave informed consent.
REFERENCES
1. Gessler B, Eriksson O, Angenete E. Diagnosis, treatment, and consequences of anastomotic leakage in colorectal surgery. Int J Colorectal Dis. 2017;32(4):549-556.
2. Su'a B, Milne T, Jaung R, Jin JZ, Svirskis D, Bissett IP, et al. Detection of anastomotic leakage following elective colonic surgery: results of the prospective biomarkers and anastomotic leakage (BALL) study. J Surg Res. 2022;273:85-92.
3. Paasch C, Rink S, Steinbach M, Kneif S, Peetz D, Klötzler A, et al. Bilirubin, urobilinogen, pancreas elastase and bile acid in drain fluid. The GBUP-study: Analysis of biomarkers for a colorectal
anastomotic leakage. Ann Med Surg (Lond). 2018;35:44-50.
4. Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304-377.
5. Twohig K, Ajith A, Mayampurath A, Hyman N, Shogan BD. Abnormal vital signs after laparoscopic colorectal surgery: more common than you think. Am J Surg. 2021;221(3):654-658.
6. Erb L, Hyman NH, Osler T. Abnormal vital signs are common after bowel resection and do not predict anastomotic leak. J Am Coll Surg. 2014;218(6):1195-9.
7. Komen N, De Bruin RW, Kleinrensink GJ, Jeekel J, Lange JF. Anastomotic leakage, the search for a reliable biomarker. A review of the literature. Colorectal Dis. 2008;10(2):109-15; discussion 115-7.
8. Aziz O, Albeyati A, Derias M, Varsani N, Ashrafian H, Athanasiou T, et al. Anastomotic leaks can be detected within 5 days following ileorectal anastomosis: a case-controlled study in patients with familial adenomatous polyposis. Colorectal Dis. 2017;19(3):251-259.
9. Wu X, Lin G, Qiu H, Xiao Y, Wu B. Anastomotic leakage after laparoscopic-assisted radical right hemicolectomy: reason analysis and management. Zhonghua Wei Chang Wai Ke Za Zhi. 2017;20(6):671-674. Chinese
10. Fouda E, El Nakeeb A, Magdy A, Hammad EA, Othman G, Farid M. Early detection of anastomotic leakage after elective low anterior resection. J Gastrointest Surg. 2011;15(1):137-44.
11. Rama N, Lages MC, Silva CG, Motta Lima P, Campos Gil I, Guarino M, et al. The Usefulness of Inflammatory Biomarkers to Predict Anastomotic Leakage after Colorectal Surgery: Systematic Review and Meta-Analysis. Surg Gastroenterol Oncol. 2022;27:169-81.
12. Wright EC, Connolly P, Vella M, Moug S. Peritoneal fluid biomarkers in the detection of colorectal anastomotic leaks: a systematic review. Int J Colorectal Dis. 2017;32(7):935-945.
13. Rahbari NN, Weitz J, Hohenberger W, Heald RJ, Moran B, Ulrich A, et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery. 2010;147(3):339-51.
14. Parthasarathy M, Greensmith M, Bowers D, Groot-Wassink T. Risk factors for anastomotic leakage after colorectal resection: a retrospective analysis of 17 518 patients. Colorectal Dis. 2017;19(3):288-298.
15. Bakker IS, Grossmann I, Henneman D, Havenga K, Wiggers T. Risk factors for anastomotic leakage and leak-related mortality after colonic cancer surgery in a nationwide audit. Br J Surg. 2014; 101(4):424-32; discussion 432.
16. Messager M, Sabbagh C, Denost Q, Regimbeau JM, Laurent C, Rullier E, et al. Is there still a need for prophylactic intra-abdominal drainage in elective major gastro-intestinal surgery? J Visc Surg. 2015;152(5):305-13.
17. Li Z, Li Z, Zhao L, Cheng Y, Cheng N, Deng Y. Abdominal drainage to prevent intra-peritoneal abscess after appendectomy for complicated appendicitis. Cochrane Database Syst Rev. 2021;8(8): CD010168.
Full Text Sources:
Abstract:
Views: 5550

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.