Surgery, Gastroenterology and Oncology

|
|
Introduction: One frequently diagnosed malignancy is colorectal cancer, and this study aimed to determine the incidence of colorectal cancer in seven important areas of Najaf, Iraq.
Methods: Data were collected from the statistical records of the Middle Euphrates Cancer Center (MECC) from 2016 to 2021 for some areas of Najaf province. The age of the subjects ranged from 30 to 76 years. The total number of colon cancer cases in this period were recorded for the districts of middle Al-Madina, Al-Kufa, Al-Razawi, Al-Mishkhab, Al-Haydariya, Al-Mundhirah, and Al-Hirah. There were 194 total cases during this period.
Results: We found that 22% of the cases were in 2021 for the seven regions. The data were processed using SPSS version 20 and a Chi-square test. Correlation was not significant because the p-value was greater than 0.05, but the percent change was positive (+64.28). That is, there is an increase in the incidence over time.
Conclusion: There are many factors that may underlie the increased incidence of colon cancer, e.g., food, air, and soil pollution as well as genetic factors. Therefore, aspects of health awareness in terms of food and periodic examination must be activated—especially since Iraq has suffered from many wars in previous years.
Introduction
Alarming cancer statistics include estimates of 18.1 million new cases and 9.6 million cancer-related deaths worldwide (1). A main cause of cancer mortality (9.2%) and one of the most frequently diagnosed malignancies (6.1% incidence) is colorectal cancer (CRC). Adenomas are the origin of the majority of colorectal malignancies (2). With a median age at diagnosis of 70 years, sporadic colon cancer is considered an old-age disease that affects slightly more males than females (3). More than 90% of colorectal cancer cases are sporadic, meaning that the patients are not related to someone who has had colon cancer (4). Although the evidence for a link between rectal cancer risk and ionizing radiation exposure is limited, there is strong evidence this relationship in colon cancer (5).
In Western and Japanese cohort studies, lifestyle factors like smoking, drinking alcohol, eating red meat, and body mass index (BMI) have also been associated with an increased risk of colorectal cancer. There is evidence that the prognosis for colon cancer varies by anatomical subsite including time patterns of incidence, lifestyle, environmental risk factors, presence of hereditary disease, and carcinogenic pathways (i.e., proximal vs. distal location) (6). The pathophysiology of sporadic proximal and distal colon cancers is further supported by genomic research with proximal colon cancer most likely being connected to microsatellite instability (MSI) and distal colon cancer to chromo-somal instability (CIN) (7).
A 19-year follow-up research including 1.1 million Swedish males looked at the relationship between physical job activity and colon cancer. The estimated relative risk (RR) of colon cancer in males who work in sedentary occupations is 1.3 (1.2-1.5, 90% confidence interval) with the transverse colon including flexures having the highest risk (RR = 1.6) and the sigmoid having the lowest risk (RR = 1.2) (8).
Several epidemiological studies have shown a link between solar UVB radiation exposure and lowered risk of malignancies including colon cancer (9). Colon cancer has been the subject of numerous international investigations: Western and Northern Europe have a slightly higher incidence than Southern and Eastern Europe. Australia, Europe, and North America are other high-risk regions. There is less risk in Central and South America, Asia, and Africa (10). According to a study, patients with stage II colon cancer who also had blockage, perforation, emergency admission, T4 stage, and less than 12 lymph nodes removed might be considered for adjuvant treatment (11).
According to the above studies and the increase in cancerous diseases that have been observed in Iraq—especially in recent years—we decided to study the statistics on colon disease and to seek the assistance of the Middle Euphrates Center for Cancerous Tumors to obtain the required data. The location of the tumor in the gut and the extent of its internal dissemination determines the signs and symptoms of colorectal cancer (metastasis), constipation, melena, bloating, fullness, cramps, weight loss, and fatigue (12).
More than 75-95% of colon cancer instances involve individuals with little to no hereditary predisposition. Incidence factors include consuming excessive fat, drinking alcohol, eating red meat or processed meat, being obese, smoking, and not exercising. Males and the elderly are also at an increased risk. About 10% of infections are related to insufficient activity, and alcohol abusers are more likely to become infected. Five glasses of water per day were found to lower the risk of adenomas and colorectal cancer (13).
In light of the increase in cancerous diseases, including colon cancer, we decided to collect the number of cases of this disease available in the oncology center’s records and study them statistically to determine whether they decreased or increased over time.
Methods
All cases were diagnosed in the city, and no cases were recorded outside the center. The data obtained were inclusive of all sub-regions in the governorate. The area is managerially divided into seven regions. The population of any region in Najaf city depends on (2016 -2021) statistics. The data of colon cancer patients were obtained in cooperation with the staff of the Middle Euphrates Cancer Center (MECC) where the data were collected from 2016 to 2021.
Statistical analysis
Statistical software (SPSS version 20) was used to analyze the data and perform a Chi-squared test. The goal was to evaluate an association between the city and year with the number of cases recorded.
Results
Table 1 compares the number of new cases from 2016 to 2021 and the total population for each region. The year 2021 had the most new infections (n=43), and 2016 had the least (n=24). Table 1 also shows that the percentage of cases in the Al-Manazihira region was the highest of the seven regions studied (50%) in 2016. The Al-Hira region had the most cases in 2017 and 2018, and the Al-Haidariya region was the highest (at a rate of 25%) in 2019 and 2020. The Razavi region had the highest percentage in 2021.
Table 1 - The cross Tabulation between districts of Al Najaf city and years
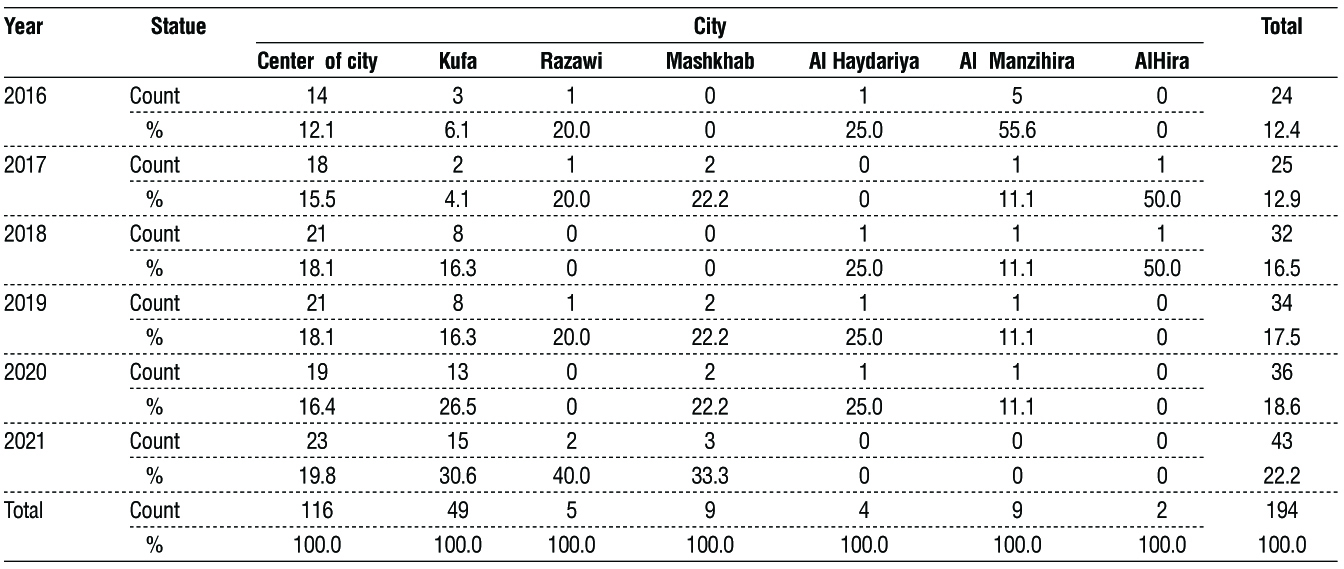
Table 2 shows the results of cross tabulation between the districts and the years; it shows the counts and percentages of the patients in each city according to year. The results indicate that the city center has the largest number of patients in all years; Kufa is the second-most, and the Al-Haidariya and Al-Hira districts have the smallest numbers of the patients in all years (4 and 2, respectively). This is clear in table 2. The most cases were seen in 2021.
Table 2 - The result of Chi-square test of the association between the city and the year

The results shows that no significant association between the city and the year in terms of the number of patients (p-value = 0.116, which is higher than the α=.05; table 3).
Figure 1 also presents a clustered bar chart for the number of patients over time and for the seven regions studied. The incidence rate (IR) per 10,000 was highest in the Al-Manazihira area and lowest in Al-Hira area. Incidence is a measure of disease that allows us to determine a person's probability of being diagnosed with a disease during a given period of time. Therefore, incidence is the number of newly diagnosed cases of a disease. An incidence rate is the number of new cases of a disease divided by the number of persons at risk for the disease. If, over the course of one year, five women are diagnosed with colon cancer, out of a total female study population of 200 (who do not have colon cancer at the beginning of the study period), then we would say the incidence of colon cancer in this population was 0.025 (or 2,500 per 100,000 women-years of study).
Table 3 - Incedent Rate (IR) (per 10,000) of colon cancer by age catgorices and the Percentage change(p.c)in Najaf Governorate (2016-2021)

Figure 1 - Clustered Bar chart of the number of patients according to year and city

Discussion
These findings are provisional and may change. Therefore, care must be taken when interpreting the data. Updated findings will be released to help organizations using vital statistics consider the most recent year available. We noticed an increase in the number of cases over time. In 2016 there were 24 cases, and 43 cases in 2021. This is an indicator that must be considered to determine whether the increasing incidence is related to the increase in population or the presence of other risk factors.
The cases of colon cancer patients were classified according to the seven regions of Najaf Governorate and the population of each region. The most cases of colon cancer were in the city center (n116), and the least in the Al-Hira region (n=2). Analysis considered the subject age (30-79 years) and location of residence based on the records of the National Cancer Center in Najaf. We then calculated the incidence rate for the number of colon cancer cases diagnosed in Najaf/Iraq. The incidence rates can be calculated by race, sex, age, etc. The highest incidence rates were in the Al-Manathira area (4.42) and the lowest in Al-Hira (1.02). The most important point in Table 4 is that the percentage change (15) was calculated to determine any decrease or increase in the number of colon cancer cases. The value was 64.28, which is positive and indicates an increase in the number of new and previous cases of colon cancer. However, this was not statistically significant (p-value = 0.116) at the 95% confidence interval.
Conclusion
Data was collected from the Middle Euphrates Cancer Center in Najaf to estimate the incidence colorectal cancer for the years 2016 to 2021. There was an increase in the number of cases in light of the available data, and action should be taken in many aspects such as increasing health guidelines and addressing deficiencies in the nature of food and lifestyle. There will be more studies that describe cases as a function of time and region leading to more accurate and comprehensive results.
Acknowlegment
We extend our thanks to all the employees of the Middle Euphrates Cancer Center, especially the director of the center, the working doctors and the calculator unit, for their assistance in completing the research.
Conflict of interest
There are no conflicts of interest to declare.
Funding disclosure: support by ourselves.
Ethical Approval
The study protocol was approved by local ethics committee.
Reference
1.Feng RM, Zong YN, Cao SM, Xu RH. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun (Lond). 2019;39(1):22.
2.Sawicki T, Ruszkowska M, Danielewicz A, Nied?wiedzka E,Ar?ukowicz T, Przyby?owicz KE. A review of colorectal cancer in terms of epidemiology, risk factors, development, symptoms and diagnosis. Cancers (Basel). 2021;13(9):2025.
3.Labianca R, Nordlinger B, Beretta GD, Brouquet A, Cervantes A; ESMO Guidelines Working Group. Primary colon cancer: ESMO Clinical Practice Guidelines for diagnosis, adjuvant treatment and follow-up. Ann Oncol. 2010;21 Suppl 5:v70-7.
4.Farrar WD, Sawhney MS, Nelson DB, Lederle FA, Bond JH. Colorectal cancers found after a complete colonoscopy. Clin Gastroenterol Hepatol. 2006;4(10):1259-64.
5.Sugiyama H, Misumi M, Brenner A, Grant EJ, Sakata R, Sadakane A, et al. Radiation risk of incident colorectal cancer by anatomical site among atomic bomb survivors: 1958–2009. Int J Cancer. 2020; 146(3):635-645.
6.Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 2019;16(12):713-732.
7.Iacopetta B. Are there two sides to colorectal cancer? Int J Cancer. 2002;101(5):403-8.
8.Gerhardsson M, Norell SE, Kiviranta H, Pedersen NL, Ahlbom A. Sedentary jobs and colon cancer. Am J Epidemiol. 1986;123(5):775-80.
9.Spina C, Tangpricha V, Yao M, Zhou W, Wolfe MM, Maehr H, et al. Colon cancer and solar ultraviolet B radiation and prevention and treatment of colon cancer in mice with vitamin D and its Gemini analogs. J Steroid Biochem Mol Biol. 2005;97(1-2):111-20.
10. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74-108.
11. Feng Q, Chang W, Mao Y, He G, Zheng P, Tang W, et al. Tumor-
associated macrophages as prognostic and predictive biomarkers for postoperative adjuvant chemotherapy in patients with stage II colon cancer. Clin Cancer Res. 2019;25(13):3896-3907.
12. Elliot JW. II. The operative relief of gangrene of intestine due to occlusion of the mesenteric vessels. Ann Surg. 1895;21(1):9-23.
13. Zelber-Sagi S, Ivancovsky-Wajcman D, Fliss Isakov N, Webb M, Orenstein D, Shibolet O, et al., High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J Hepatol. 2018;68(6):1239-1246.
14. Altekruse SF, Henley SJ, Cucinelli JE, McGlynn KA. Changing hepatocellular carcinoma incidence and liver cancer mortality rates in the United States. Am J Gastroenterol. 2014;109(4):542-53.
15. Chien LH, Tseng TJ, Chen CH, Jiang HF, Tsai FY, Liu TW, et al. Comparison of annual percentage change in breast cancer incidence rate between Taiwan and the United States—A smoothed Lexis diagram approach. Cancer Med. 2017;6(7):1762-1775.
Full Text Sources:
Abstract:
Views: 3277

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.