Surgery, Gastroenterology and Oncology

|
|
Background: HCV chronic infection is a leading cause of end-stage liver disease and liver transplantation. The aim of our study was to assess the benefits of novel anti-HCV therapeutic approaches in obtaining viral clearance, in reducing liver inflammation, in regression of fibrosis, and improvement of liver-related morbidity and mortality.
Material and methods: We performed an observational, prospective, non-interventional study in 260 patients with HCV chronic infection and advanced liver fibrosis (F3 and Child class A liver cirrhosis), treated with direct-acting antivirals (Ombitasvir/Ritonavir/Paritaprevir + Dasabuvir, Ledipasvir/ Sofosbuvir). Liver fibrosis grade was assessed by non-invasive methods. HCV-RNA was determined in all patients at baseline and at 3 months after the end of treatment. The parameters used for follow-up and comparison were liver stiffness, liver function tests, abdominal ultrasound, and endoscopy.
Results: We identified 95 patients with F3 fibrosis and 165 patients with F4 fibrosis, of which 188 were treated with Ombitasvir/Ritonavir/Paritaprevir + Dasabuvir, and 72 were treated with Ledipasvir/ Sofosbuvir. We obtained an SVR rate of 99.4% in the first group and 94.4% in the 2D-treated group. We observed an improvement of the biochemical profile. We also remarked a decrease of liver stiffness 12 months post-SVR, especially in the patient population with fibrosis grade F3. Multivariate analysis identified the following factors associated with non-regression of fibrosis at 12 months after achieving SVR: diabetes mellitus, esophageal varices, serum albumin below 3 gr/dL and AST/ALT ratio < 0.8.
Conclusions: DAAs proved their efficacy in achieving viral clearance, with SVR rates > 95%. DAA therapy reduces liver inflammation, improves the biochemical profile, and reduces liver fibrosis grade, especially in patients with F3 fibrosis at the time of treatment initiation.
INTRODUCTION
HCV chronic hepatitis represents a major public health issue worldwide, affecting approximately 71 million people (1). The evolution of the disease is slowly progressive, characterized by persistent inflammation, and up to 20% of patients progress to liver cirrhosis in 20-30 years after the moment of infection (2). Therefore, HCV is a major cause of end-stage liver disease and a leading indication for liver transplantation. The development of new therapeutical options has made it possible to eliminate the virus in patients with advanced disease, to reduce the need for transplantation and to prolong survival.
Studies have shown the benefits of new antiviral agents not only in obtaining viral clearance, but also in reducing liver inflammation, in the regression of fibrosis, and in the decrease of complications associated to extrahepatic manifestations and of the need for liver transplantation (3). However, recent articles suggest that viral clearance in patients with liver cirrhosis reduces, but does not totally eliminate, the risk of developing hepatocellular carcinoma (4).
Regarding the regression of liver fibrosis after treatment, current data suggests the significant
benefits in reducing fibrosis grade after removing viral aggression. Treatment with direct-acting antivirals (DAA) improves liver-related morbidity and mortality (5).
The aim of our study was to assess the benefits of novel anti-HCV therapeutic approaches not only in obtaining viral clearance, but also in reducing liver inflammation, regression of fibrosis, and improvement of liver-related morbidity and mortality.
Material and methods
We selected 260 patients treated in the Department of Internal Medicine, Fundeni Clinical Institute. Eligible patients were represented by adult patients, with ages ranging from 30 to 80 years, with HCV chronic infection, with positive viremia (HCV-RNA > 10 IU/mL), with advanced liver fibrosis (F3) and Child class A liver cirrhosis, naive/experimented to previous antiviral therapies, with diagnosis established on clinical, imagistic and laboratory criteria, who received treatment with direct-acting antivirals.
At the time of study initiation, the direct-acting antiviral treatment regimens approved in Romania were: the 3D-Ombitasvir/Ritonavir/Paritaprevir and Dasabuvir regimen, and the fixed-dose combinations Sofosbuvir/Ledipasvir, Grazoprevir/Elbasvir, with or without association of Ribavirin.
A thorough anamnesis was taken in all patients (history of infection, previous antiviral therapies and adherence to treatment, previous endoscopic investigations, use of oral contraceptives in fertile women, chronic concomitant medication).
The degree of liver fibrosis was assessed by non-invasive methods. Complete biochemical tests were performed: electrolytes, renal function tests (urea, creatinin, uric acid), coagulation tests (PT, aPTT, INR), liver function tests, serum albumin. AFP levels were determined before antiviral treatment in all patients, with an upper limit of normal of 10 ng/mL. Basal plasma glucose and glycated hemoglobin (HbA1c%) were determined in all patients with a medical history of diabetes mellitus.
Elastography (Fibroscan) was performed in all patients for assessing liver stiffness. We used the following cut-offs to differentiate between Metavir fibrosis stages: 5.5 kPa, 7.1 kPa, 9.5 kPa and 14.5 kPa for F1, F2, F3 and F4, respectively. The results of the biochemical scores used for assessing liver fibrosis were determined by using the following formulas:
- APRI=(AST level/AST upper limit of normal) x 100/platelet count;
- FIB4=[age (years) x AST level (IU/L)/platelet count (109/L) x (U/L).
The cut-off values for APRI were 0.5-1.5 for F2/F3 and > 1.5 for F4, while for FIB4 they were 1.45-3.25 for F2/F3 and > 3.25 for F4.
HCV-RNA was determined using COBAS AmpliPrep/COBAS TaqMan HCV (Roche). Fibromax results were obtained with the help of Biopredictive. All elastography tests were performed on the same machine (FibroScan 502, ECHOSENS PARIS), in the Department of Internal Medicine, Fundeni Clinical Institute, with the M probe calibrated at all times, according to the requirements of the manufacturer. All patients signed an informed consent form before being included in the study, and the study was approved by the Ethics Committee of Fundeni Clinical Institute.
The following exclusion criteria were used: patients in whom a correct follow-up was not possible due to refusal to cooperate, patients with hepatocellular carcinoma diagnosed by contrast-enhanced abdominal CT/MRI before DAA initiation, patients with other chronic liver diseases (HBV coinfection, autoimmune hepatitis, primary biliary cholangitis, Wilson disease, etc), patients with extrahepatic cancers (without the approval of an onco-hematologist), patients with Child-Pugh class B and C HCV liver cirrhosis.
We designed our study as a prospective, observational, non-interventional study. Data was collected by standard medical procedures. We did not identify, in our study group, patients from high-risk groups, patients with aberrant sexual behaviour or incarcerated patients.
Clinico-biological and imagistic evaluations were performed in all patients before therapy, at end of treatment (EOT) and at 12 weeks after EOT (SVR).
Abdominal ultrasound was performed before therapy, at SVR and after 1 year in patients with advanced liver fibrosis (F3). In accordance with international guidelines, ultrasound was repeated every 3-6 months in order to screen for the occurrence of hepatocellular carcinoma.
HCV-RNA was determined in all patients before antiviral therapy and 12 weeks after EOT.
Upper digestive endoscopy was performed in all patients at baseline, and at 12 months and 24 months after EOT.
The parameters used for montoring and for comparison at 3 months – 6 months – 1 year were represented by: liver stiffness, total bilirubin, aminotransferases, serum albumin, complete blood count – with platelet count, and INR.
The antiviral treatment regimens consisted in:
- Ombitasvir+Ritonavir+Paritaprevir (12,5 mg/75 mg/50 mg) 2 tb/day plus Dasabuvir 250 mg twice a day, 12 weeks;
- Ledipasvir/Sofosbuvir (90 mg/400 mg) once a day, 12 weeks.
Statistical analysis
Continuous variables between groups were compared by the Mann-Whitney test and categorical variables by the Fisher exact test. A p value < 0.05 was considered significant. Univariate analysis identified predictors of fibrosis, which were then included in multivariate analysis using Cox’s logistic regression model. Statistical analyses were performed using the statistical software GraphPadPrism 9 (GraphPad software, California, USA).
Interactions between chronic medication and DAAs were checked for each patient, with the help of www.hep-druginteractions.org
RESULTS
The non-invasive markers for assessing liver stiffness used in our study are illustrated in table 1, accompanied by their cut-off values.
Table 1 - Assessment of fibrosis grade

We identified a total of 260 patients with advanced liver disease, of which 95 with F3 and 165 with F4 on FibroMax.
According to the national protocol approved by the National Health Insurance Company, SVR is defined as undetectable HCV-RNA, 12 weeks after the end of treatment (mandatory HCV-RNA determination between days 169-199, calculated from the first day of administration of antiviral medicaton).
Treatment failure is defined as detectable HCV-RNA, regardless of the level of detection, 12 weeks after the end of treatment.
An SVR rate of over 90% was achieved in our study group, regardless of the therapeutic regimen used. The response rates were 99.4% in patients treated with Ombitasvir/Ritonavir/Paritaprevir and Dasabuvir (187/ 188 pts) and 94.4% in the group treated with Sofosbuvir/Ledipasvir (68/72 pts) (table 2).
Table 2 - SVR rates by treatment regimen

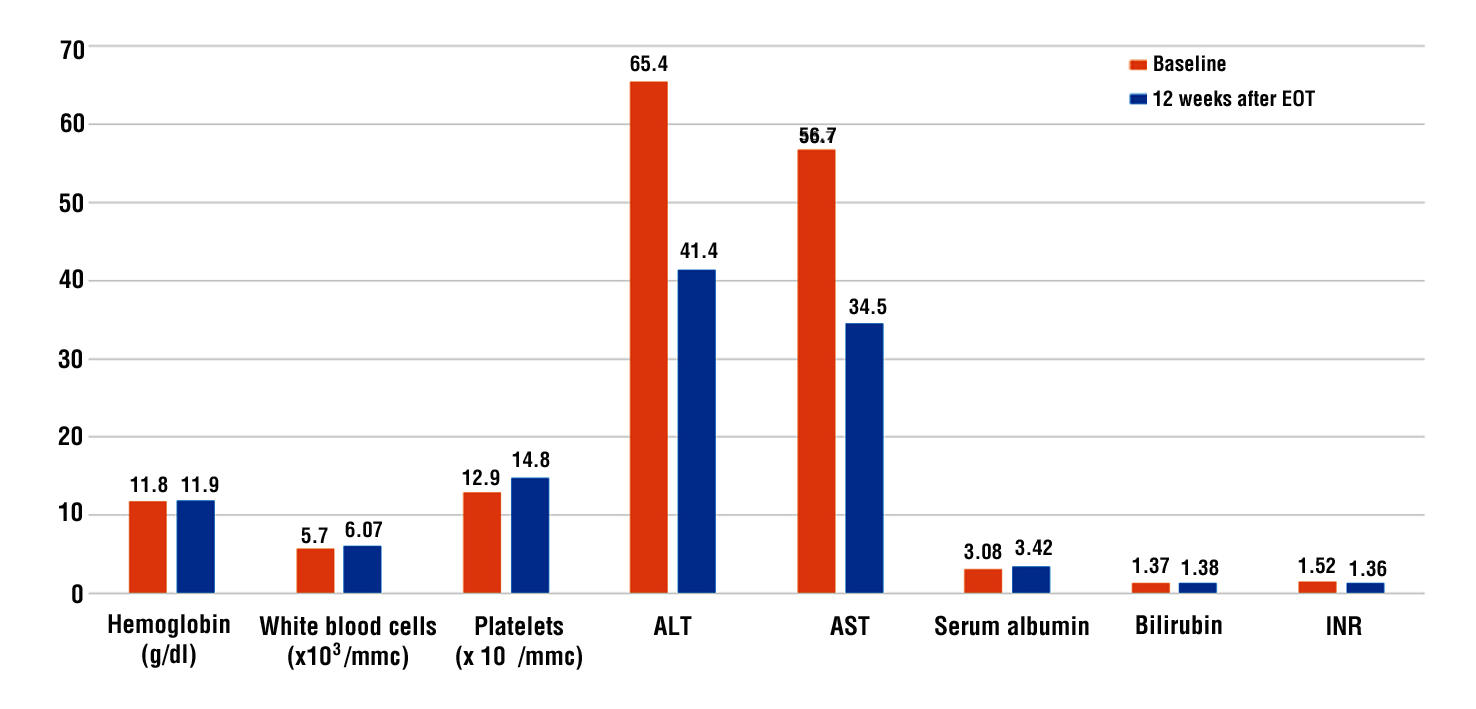
In our study group, serum albumin levels were 3.08±0.36 g/dL at the end of treatment vs 3.42±0.38 at 12 weeks after end of treatment (p < 0.002). Total serum bilirubin remained at a constant level (1.37±0.26 at EOT vs 1.38±0.34 mg/dL at SVR), without notable differences. INR values were 1.52±0.8 at baseline and 1.36±0.21 at 12 weeks after end of treatment (p <0.03).
Both ALT and AST decreased signficantly from the moment of treatment initiation to end of treatment, with normalization of AST levels 12 weeks after the end of antiviral therapy (ALT from 65.4±41.3 IU/L at EOT to 41.4±16.9 IU/L at SVR, p < 0.001; AST from 56.7±36.4 IU/mL at EOT to 34.2±0.38 at SVR, p < 0.001).
We did not observe a significant impact on hemoglobin levels, which remained unchanged. However, complete blood count showed a significant improvement of the mean platelet count in our patients – from 129±11.7 x 103/mm3 at baseline to 148±22.6 x 103/mm3 at 12 weeks after end of treatment, p ± 0.042 (table 3, fig. 1).
Table 3 - Evolution of the main biochemical and immunological characteristics

Figure 1 - Evolution of the main biochemical and immunological characteristics
In our study, we observed a decrease of liver stiffness at 12 months after SVR, especially in patients with F3 fibrosis, with a significant improvent of the APRI, FIB4 and Fibrotest scores (table 4).
Table 4 - Evolution of Fibrotest, APRI and FIB4 at baseline and at 12 weeks after end of therapy

With regards to the evolution of esophageal varices after antiviral therapy, we remarked a regression of varices grade of 77% after 24 months and a progression of 7.5% (fig. 2).
Figure 2 - Evolution of esophageal varices according to the achievement of sustained virological response
Multivariate analysis revealed that the factors associated with non-regression of fibrosis after therapy are the presence of diabetes mellitus, the presence of esophageal varices, serum albumin below 3 g/dL, thrombocytopenia < 100.000/mmc, and AST/ALT ratio < 0.8 (table 5).
Table 5 - Association of clinico-biological parameters with lack of fibrosis regression at more than 12 months after SVR

DISCUSSIONS
Direct-acting antivirals represent the new standard-of-care in chronic hepatitis C virus infection, being associated with high rates of sustained virological response at 12 weeks after end of treatment, and with a positive impact on reduction of fibrosis.
Regression of liver fibrosis remains one of the hot topics for experts in the field of liver disease. HCV elimination following treatment with direct-acting antivirals does not eradicate the risk of hepatocellular carcinoma, especially in patients with advanced fibrosis and liver cirrhosis. This is not at all surprising, because treatment does not immediately determine the regression of the underlying pathogenic mechanism, although achieving SVR may reduce the progression/ stimulate regression of liver fibrosis. Therefore, advanced liver fibrosis prior to antiviral therapy represents one of the most important predictive factors for the occurrence of HCC after treatment with DAAs.
There is consistent evidence regarding the role of measuring liver rigidity by non-invasive markers, in order to assess the risk of developing hepatocellular carcinoma.
The virological response rates in our study are similar to those published in the literature. No significant differences were observed between age groups. Kanda et al report similar efficacy rates in patients ³ 75 years old, compared to those with age below 75 years (6). The same theory is also demonstrated by Tada et al, with an SVR rate of 97.5% in seniors over 75 years old, compared to 98.8% in those with age below 75 years (7). In the study of Ogawa et al, SVR was achieved in 99.2% of patients under 65 years old, 98% of patients with ages between 66-74 years, and 99.6% of patients ³ 75 years (8).
The following factors for unfavorable treatment response were identified: male gender, cirrhotic status, low serum albumin levels (≤ 3 g/dL), elevated serum bilirubin levels, and thrombocytopenia (<100,000/mmc).
In our study group we identified 5 patients with therapeutic failure, 4 of them of male gender. All five patients presented cirrhosis, and all were naive to previous DAA therapy.
With regards to the evolution of clinico-biological parameters, in populational studies, serum ALT levels correlated with a progressive increase in the risk of death of all causes, and especially liver-related death. Persistently normal ALT levels are observed in 20-30% of patients with HCV chronic hepatitis, and this is associated with lower grades of fibrosis on liver biopsy. Moreover, the disease has a slower progression compared to patients with elevated ALT. In cross-sectional studies performed on liver biopsies, AST/ALT ratio was identified as a predictive factor. A study performed in Taiwan showed that ALT level presented a cummulative risk factor for hepatocellular carcinoma of 1.7% for serum levels ≤ 15 IU/L. This increased to 4.2% for ALT levels between 15-45 IU/L and to 13.8% for ALT levels ≥ 45 IU/L (9). Consequently, monitoring of ALT levels is recommended in the management of patients with HCV chronic hepatitis.
A study that aimed to identify factors associated with therapeutical success and post-therapy evolution identified the following negative prognostic factors: association of obesity, association of diabetes mellitus, persistently elevated aminotransferase levels, cirrhotic status and alcohol intake (10).
Weight loss and physical activity are factors known to reduce the level of steatosis, obesity and insulin resistance, decrease serum ALT levels and reduce fibrosis, despite the persistence of positive HCV-RNA. The intensity and type of physical exercise are essential for obtaining benefits. High-intensity aerobic training has been shown to improve liver enzymes and the psychological status of patients, and contributes to the improvement of quality of life in overweight and obese patients. Results similar to ours were also obtained in previous studies. The results support the theory that normalization of the values of biological parameters after DAA treatment is associated with restoration of immune response activity (10,11).
The reactivated immune response may achieve residual viral clearance in the weeks following therapy. Dendritic cells are involved in coordinating the innate and acquired immune response to viral infection via growth receptors. A study which examined the level of soluble CD163 released from activated hepatic macrophages in chronic viral infection and post-therapy histological activity showed that serum levels rapidly decreased after achieving eradication, which was also accompanied by the reduction of fibrosis and of inflammatory histology (12).
Another study demonstrated the reduction or normalization of immune activity markers (aminotransferases, CD163) after achieving response to DAAs. AST levels correlated with CD163 levels (13).
Exhaustion and loss of T lymphocyte effector function at the hepatic and peripheral level occur in chronic HCV infection. Viral eradication following DAA therapy leads to a rapid increase of CD8+ T lymphocytes, which suggests the restoration of immune response (14).
With regards to the impact of DAAs on recovery of liver function, recent studies report that successful treatment leads to improvement in over 2/3 of cases: decrease of aminotransferase levels, progressive increase of serum albumin levels and decrease of bilirubin (15), aspects that we also observed in our study.
Improvement of thrombocytopenia, as an indirect marker of portal hypertension, in patients who achieved SVR suggests the possibility of liver fibrosis regression over time in patients with HCV chronic
hepatitis who achieve viral eradication.
The availability of DAA therapy, which is extremely potent and has an excellent safety profile, has transformed the population of HCV patients with advanced liver fibrosis into a group which is no longer considered as „difficult to treat”.
Our study is consistent with previous real-life studies that investigated treatment with OBT/PTV/DSV and SOF/LDV in patients with HCV chronic infection and showed SVR rates of 86-100%. The SVR rate in our patient group was higher compared to the Spanish study of Chamorro-de-Vega, in which 93.8% of cirrhotic patients achieved SVR (16).
Due to the fact that in Romania, it was mandatory to determine fibrosis stage (by non-invasive biochemical markers and non-invasive imaging - Fibroscan) before initiating DAA therapy, it was easy to monitor the evolution of fibrosis at 12 months after obtaining SVR.
Many studies have shown a decrease of liver stiffness after DAA therapy, assessed by APRI, FIB4, Fibrotest and Fibroscan, which led to a reduction of portal hypertension. Besides the fact that these tests are non-invasive, they can be repeated as frequently as necessary and can assess the evolution of liver fibrosis over time. Moreover, their sensitivity and specificity rates are high enough to allow them to be used in long-term monitoring and in assessment of patient prognosis.
These non-invasive tests have a major contribution in evaluating therapeutic response to the novel DAAs. The antifibrotic effect of DAAs is easy to monitor and, ideally, even a slight improvement of fibrosis grade can be detected early. These non-invasive tests have become increasingly popular in clinical practice for staging fibrosis grade, practically replacing liver biopsy.
However, the current scoring systems based on serological markers present a higher sensitivity in cases of advanced liver fibrosis and liver cirrhosis, but they frequently lack sensitivity in differentiating between early fibrosis stages (≤ F2). A meta-analysis concluded that an APRI score > 1 presents a sensitivity and specificity of over 70% in predicting advanced liver fibrosis (17). The use of a cut-off value increased specificity, but decreased sensitivity for detecting liver cirrhosis. The lower the score (<0.5), the better the negative predictive value. A value of >1.5 is capable of excluding liver cirrhosis. Intermediate values are not as useful.
APRI alone is not sensitive enough to exclude advanced liver disease. Current evidence suggests that using APRI in combinations (APRI+Fibrotest) increases diagnostic accuracy compared to its use alone (18).
FIB4 evaluates fibrosis grade by using a combination of data that includes patient age, platelet count, ALT and AST. The scoring system produces a score of <1.45 – negative predictive value in over 90% of cases with advanced liver fibrosis, regardless of etiology. A score > 3.25 has a positive predictive value for advanced fibrosis, with a sensitivity of 65% and a specificity of 97% (19).
Patients who continue to have a fibroscan score > 18 kPa after therapy will remain at a high risk of developing complications. FIB4 and APRI scores decreased significantly after DAA therapy.
A recent study in non-cirrhotic patients reported an accelerated decrease of APRI and FIB4 scores starting from week 2 and up to week 12 post-therapy (20). Another study underlined a decrease of elastography parameters at 18 months after SVR, but it is still under debate if this suggests a true regression of fibrosis grade, or if it is just a consequence of the resolution of chronic liver inflammation (21).
Therefore, the observation that FIB4 and APRI scores decrease after treatment can be explained by the reduction of chronic liver inflammation and is reflected biochemically by the decrease of aminotransferases.
CONCLUSIONS
DAAs proved their efficacy in achieving viral clearance, with SVR rates > 95%, regardless of the treatment naive or experienced status of the patient. DAA therapy reduces liver inflammation, improves the biochemical profile, and reduces liver fibrosis grade (quantified by elastography and biochemical scores, such as APRI and FIB4), especially in patients with F3 fibrosis at the time of treatment initiation.
Conflicts of interest
The authors declare no conflicts of interest.
Ethics of approval
For performing this study ethical approval was obtained.
REFERENCES
1. World Health Organization, Hepatitis C, 2020.
2. Tong MJ, el-Farra NS, Reikes AR, Co RL. Clinical outcomes after transfusion-associated hepatitis C. N Engl J Med. 1995;332(22): 1463-6.
3. Nahon P, Bourcier V, Layese R, Audureau E, Cagnot C, Marcellin P, et al. Eradication of hepatitis C virus infection in patients with cirrhosis reduces risk of liver and non-liver complications. Gastroenterology. 2017;152(1):142-156.e2.
4. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):
262-270.
5. Fehily SR, Papaluca T, Thompson AJ. Long-term impact of direct-acting antiviral agent therapy in HCV cirrhosis: critical review. Semin Liver Dis. 2019;39(3):341-353.
6. Kanda T, Lau GKK, Wei L, Moriyama M, Yu ML, Chuang WL, et al. APASL HCV guidelines of virus-eradicated patients by DAA on how to monitor HCC occurrence and HBV reactivation. Hepatol Int. 2019; 13(6):649-661.
7. Tada T, Kumada T, Toyoda H, Kiriyama S, Tanikawa M, Hisanaga Y, et al. Viral eradication reduces all-cause mortality, including non-liver-related disease, in patients with progressive hepatitis C virus-related fibrosis. J Gastroenterol Hepatol. 2017;32(3):687-694.
8. Ogawa E, Furusyo N, Murata M, Toyoda K, Hayashi T, Ura K. Potential risk of HBV reactivation in patients with resolved HBV infection undergoing direct-acting antiviral treatment for HCV. Liver Int. 2018;38(1):76-83.
9. Llorens-Revull M, Costafreda MI, Rico A, Guerrero-Murillo M, Soria ME, Píriz-Ruzo S, et al. Partial restoration of immune response in Hepatitis C patients after viral clearance by direct-acting antiviral therapy. PLoS One. 2021;16(7):e0254243.
10. Tacke F, Boeker KHW, Klinker H, Heyne R, Buggisch P, Pathil A, et al. Baseline risk factors determine lack of biochemical response after SVR in chronic hepatitis C patients treated with DAAs. Liver Int. 2020;40(3):539-548.
11. Golden-Mason L, Rosen HR. Natural killer cells: multifaceted players with key roles in hepatitis C immunity. Immunol Rev. 2013; 255(1):68-81. A
12. Laursen TL, Siggard CB, Kazankov K, Sandahl TD, Møller HJ, Ong A, et al. Rapid and persistent decline in soluble CD163 with successful direct-acting antiviral therapy and associations with chronic hepatitis C histology. Scand J Gastroenterol. 2018; 53(8):986-993.
13. Kostadinova L, Shive CL, Zebrowski E, Fuller B, Rife K, Hirsch A, et al. Soluble markers of immune activation differentially normalize and selectively associate with improvement in AST, ALT, albumin, and transient elastography during IFN-free HCV therapy. Pathog Immun. 2018;3(1):149-163.
14. Burchill MA, Golden-Mason L, Wind-Rotolo M, Rosen HR. Memory re-differentiation and reduced lymphocyte activation in chronic HCV-infected patients receiving direct-acting antivirals. J Viral Hepat. 2015;22(12):983-91.
15. Burchill MA, Golden-Mason L, Wind-Rotolo M, Rosen HR. Memory re-differentiation and reduced lymphocyte activation in chronic HCV-infected patients receiving direct-acting antivirals. J Viral Hepat. 2015;22(12):983-91.
16. Chamorro-de-Vega E, Gimenez-Manzorro A, Rodriguez-Gonzalez CG, Escudero-Vilaplana V, Collado Borrell R, Ibañez-Garcia S, et al. Effectiveness and Safety of Ombitasvir-Paritaprevir/ Ritonavir and Dasabuvir With or Without Ribavirin for HCV Genotype 1 Infection for 12 Weeks Under Routine Clinical Practice. Ann Pharmacother. 2016;50(11):901-908.
17. Lin ZH, Xin YN, Dong QJ, Wang Q, Jiang XJ, Zhan SH, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatology. 2011;53(3):726-36.
18. Chou R, Wasson N. Blood tests to diagnose fibrosis or cirrhosis in patients with chronic hepatitis C virus infection: a systematic review. Ann Intern Med. 2013;159(5):372.
19. Sterling RK, Lissen E, Clumeck N, Sola R,Correa MC, Montaner J, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006; 43(6):1317-25.
20. Fehily SR, Papaluca T, Thompson AJ. Long-term impact of direct-acting antiviral agent therapy in HCV cirrhosis: critical review. Semin Liver Dis. 2019;39(3):341-353.
21. Kanda T, Lau GKK, Wei L, Moriyama M, Yu ML, Chuang WL, et al. APASL HCV guidelines of virus-eradicated patients by DAA on how to monitor HCC occurrence and HBV reactivation. Hepatol Int. 2019; 13(6):649-661.
Full Text Sources:
Abstract:
Views: 5106

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.