Surgery, Gastroenterology and Oncology

|
|
Introduction: Endometrial cancer (EC) is the most common malignancy in female genital tract. The prognostic factors that influence the evolution of endometrial cancer are: age, histological type, depth of myometrial invasion, degree of differentiation, lymphovascular and lymphogenic involvement. Although the prognosis is relatively good for patients with low grade morphology and early stages of the disease small percentage of patients develop recurrence, which cannot be predicted at moment of diagnosis. Aim: This study purposed to estimate Ck19 and CD44 expression in two aggressive types of myoinvasion in EC and to find a correlation between their expression and prognostic significance.
Matherials and Methods: We analyzed 30 archival specimens of patients with primary EC, divided into two groups: 16 cases with microcystic, elongated and fragmented (MELF) type of invasion and 14 cases with diffuse infiltrating (DI) type. Immunohistochemistry for CK 19 and CD 44 was performed on formalin-fixed paraffin-embedded tumor tissue samples.
Results: Statistically significant difference was observed between the MELF and diffuse group in tumor invasive front for CK 19 expression. The MELF demonstrated predominantly diffuse Ck19 staining at the tumor periphery, while the diffuse type demonstrated predominantly focal CK19 staining at the tumor periphery. There was no statistically significant difference between MELF and diffuse group in tumor core (conventional glands) for CK 19 expression. The same was observed in the MELF and diffuse group in tumor core (conventional glands) and tumor invasive front for CD 44 expression.
Conclusion: CK19 can be used as additive immunohistochemical marker in cases of MELF-type of invasion and may be useful in disclosing of the discrete focuses of myometrial involvement. CD44 was expressed strongly in EC in early-stage disease and decreased as the disease became more invasive and aggressive.
INTRODUCTION
Endometrial cancer (EC) is the fourth most common malignancy in women and represents 6% of all gynecological cancers (1). According to the Bulgarian National Cancer Registry /2015/, uterine cancer accounts for 8.6% of all cancers in women and ranks 2nd after breast cancer. In Bulgaria, about 1227 women get sick every year (2).
The prognostic factors that influence the evolution of EC are: age, histological type, depth of myometrial invasion (MI), degree of differentiation, lymphovascular invasion (LVI), and lymphogenic metastases (LM). The tumor stage, which is based on the depth of MI, is one of the most important among them (3). Five main models of MI have been identified: diffuse infiltrating (DI), expansive (E), microcystic, elongated and fragmented (MELF) glands, adenomyosis-like (Am) and malignant-like adenoma (AM). DI and MELF are considered to be the most aggressive among them (4,5).
DI model of MI is determined as the presence of single or small groups (less than 3) glands with irregular glandular contours with or without desmoplastic stromal response (3). This is the most common model of MI found in 49 - 89% of the EC (3, 4). It is an indicator of poor prognosis, as it is associated with a low degree of differentiation, LVI and recurrence. Immunophenotypically shows strong expression of markers for stem cell carcinoma (SCC) - CD44, CD133 and loss of expression of hormone receptors - ER, PR (4).
CD44 is the primary hyaluronic acid receptor, and is responsible for cell adhesion to this basic component of extracellular matrix. CD44 affects carcinogenesis of many cancers through several mechanisms, notably cell migration and metastasis initiation (5). CD44 is one of the markers found on the surface of cancer stem cells, which are defined as a subtype of tumor cells with the capacity to self-renew and give rise to the differentiated cells that represent the base of the tumor (6,7).
But accessible information on the role of CD44 in pathogenesis of EC are not well investigated. MELF is a morphologically recognized model of MI in 1994 by Lee, Vacek, Belinson and defined by Murray et al. in 2003 as the presence of microcystic or fissure glands upholstered by flattened endothelium-like epithelium with eosinophilic cytoplasm and squamous appearance which are elongated or fragmented into small compact entails or single tumor cells surrounded by fibromyxoid stroma (8,9).
MELF varies in frequency in a wide range from 7% to 48% (3,10). This model was initially thought to be the result of degenerative changes in tumor glands (9), but subsequent studies suggest that MELF is more of a zone of intensive tumor activity, like in epithelial-mesenchymal transformation (EMT) found in infiltrating edges of other neoplasms (11-15). MELF sites have an immuno-phenotype different from conventional tumor morphology. MELF shows intense expression of CK7 and CK19 and shares the immunophenotype characteristic of EMT (12,15,16). Recent studies from 2017 show in the areas with MELF, high expression of markers for CSC (CD44, CD133, Nanog1, Sall4), capable of inducing EMT (4). MELF is associated with LVI and FIGO I and II EC, in which it is found in the area of the deepest part of MI (13,17), it is also associated with an increased risk of regional lymphogenic metastases (LM) in FIGO I and low-grade endometrioid EC, according to some authors (18,19). According to other authors, more studies are needed to determine whether MELF is a risk factor for LM and respectively for a worse prognosis (20), whether it is a risk factor for a more advanced clinical stage of EC (11,20,21) and whether MELF has clinical significance in EC (21).
CK19 is a low-molecular-weight keratin belonging to the intermediate filament protein family that are useful in determining of many epithelial cells. CK19 is positive in normal epithelial cells, like glandular epithelia, but with limited expression in stratified type. Also CK19 stain positive normal endometrial gland and endo-metrial intraepithelial neoplasia (16).
In our research, we match CK19 and CD 44 expression in the two most aggressive models of myoinvasion in EC, and search a correlation between their expression in conventional glands and deep tumor margin (invasive front).
MATERIALS AND METHODS
In this study we used standard fixed and processed tissue samples from patients with hysterectomy treated at University Hospital Saint Marina, Pleven, Bulgaria.
Retrospectively, we randomly selected 30 patients from archives of the Pathology Laboratory with primary EC and divided them in two groups: 16 cases with MELF type invasion and 14 cases with DI type. The selected materials contained a sufficient amount of tumor tissue and the study in no way endangered their exhaustion.
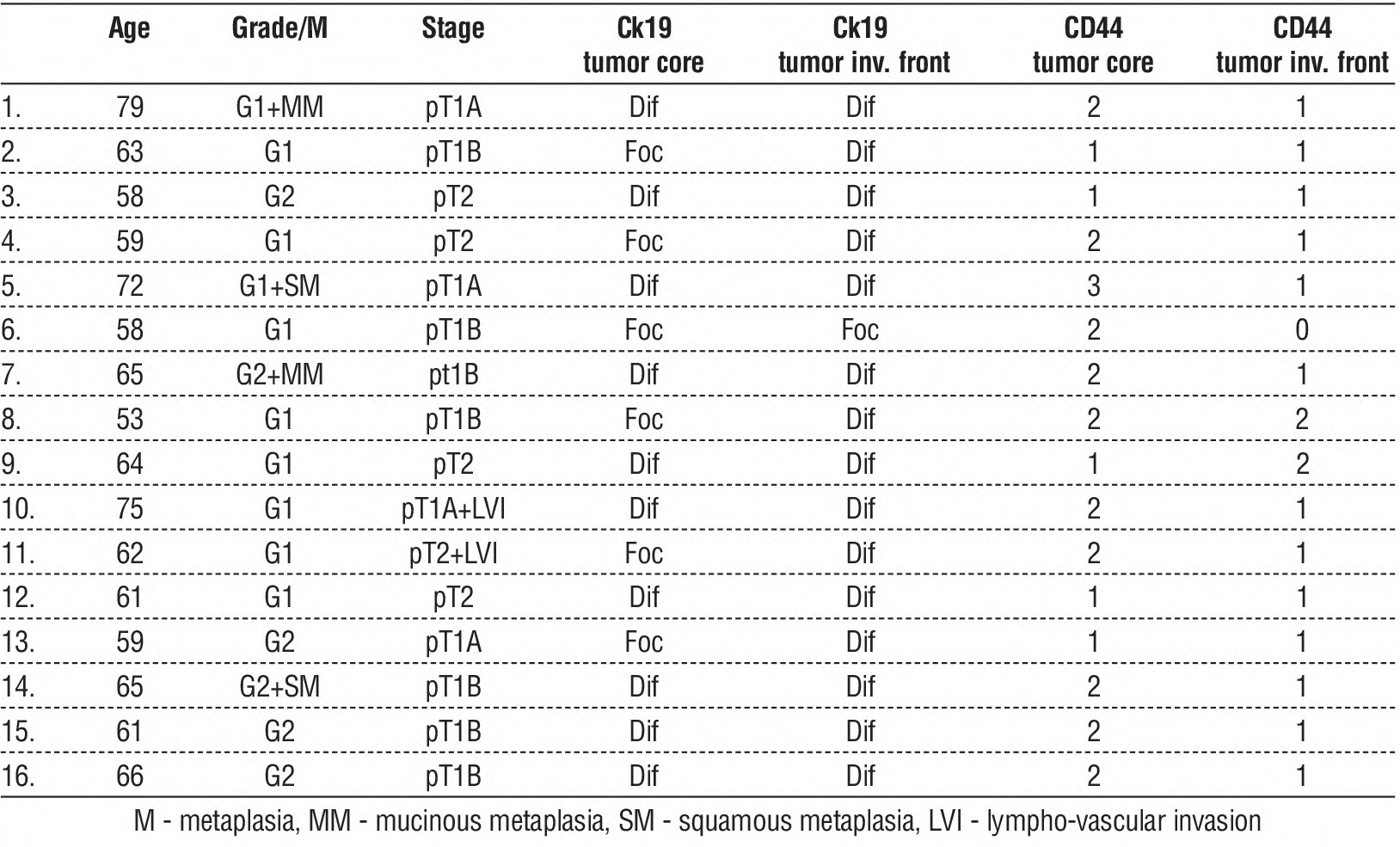
Average age of the patient in MELF group was 63.7 years (range, 53-79). There were 10 cases grade 1 and 6 grade 2; 4 of which with metaplasia (2 with squamous and 2 with mucinous metaplasia). Four tumors were of stage 1A, 7 were of stage 1B and 5 were of stage 2 by FIGO staging system (table 1).
Table 1 - Characteristics of patients with MELF
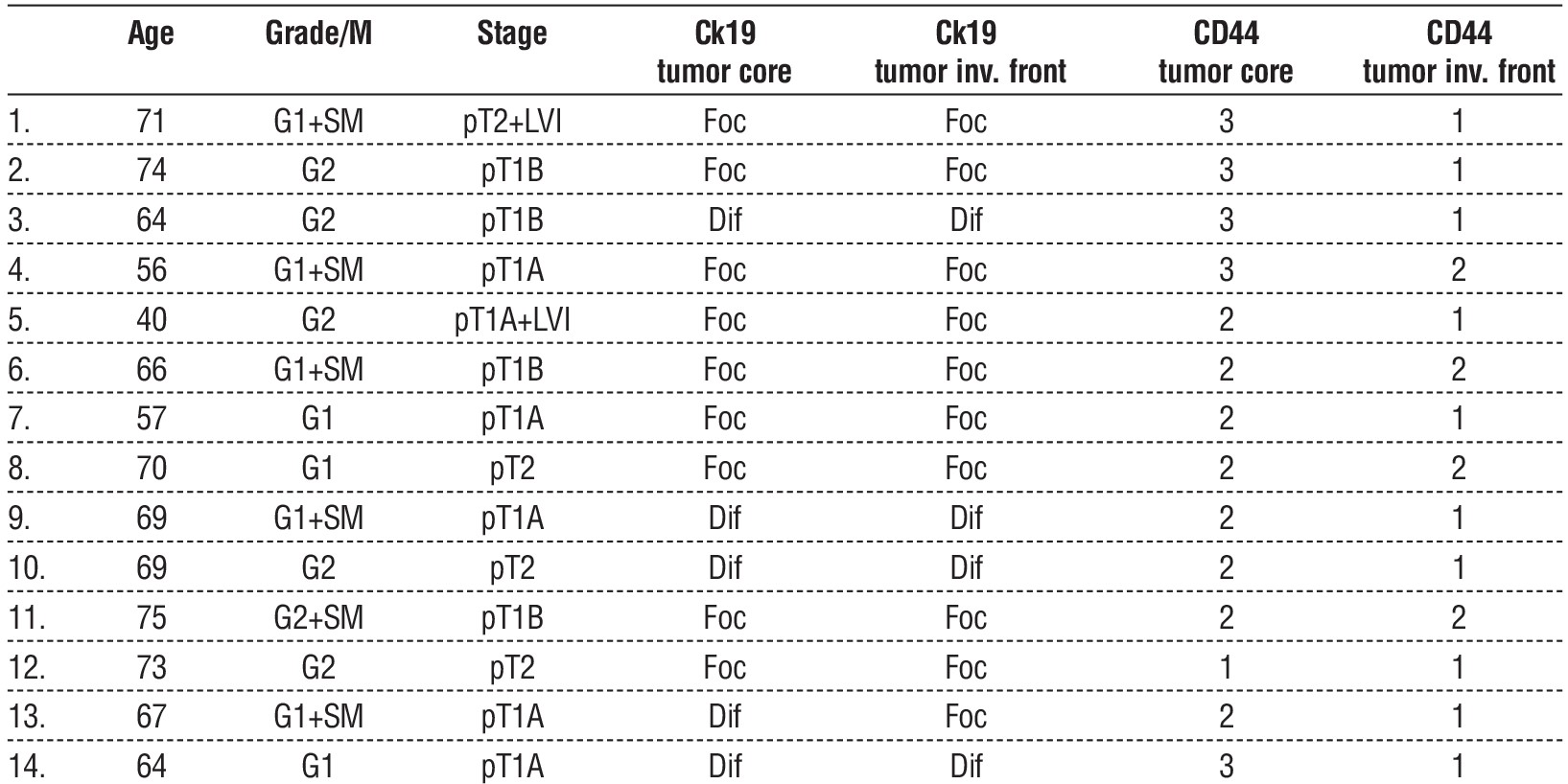
In the diffuse group, the main age of patient was 65.3 years (range, 40-75). There were 8 cases grade 1 and 6 grade 2; 6 of which with squamous metaplasia. Six tumors were of stage 1A, 4 were of stage 1B and 4 were of stage 2 according to the revised FIGO staging system (table 2).
Table2 - Characteristics of patients with diffuse MI
Immunohistochemistry
Immunohistochemistry was performed on formalin-fixed paraffin-embedded tissue specimens, with a thickness of the cuts -4µm, that were placed on 7109-A Silanized Microscope slides. The following primary antibodies were used: Cytokeratin 19 (mouse monoclonal RCK 108, Dako, Glostrup, Denmark) and CD 44 (monoclonal mouse M7082, 1:50, Dako, Glostrup, Denmark). The autoimmunostainer (Dako Link48 machine) was used for immunohistochemical staining with the FLEX Plus kit (Dako) according to manufacturer’s instructions. Wholly staining samples included suitable positive and negative controls.
Regarding the determination of the intensity of the immunohistochemical reaction:
Ck 19 - staining in half (50%) or more of the prevalent standard tumor glands was accepted as diffuse staining, whereas < 50% staining was considered as focal.
CD 44 - evaluated by a semi-qualitative method. Only the percentage of positive cells (membrane type staining) will be reported on 10 accidentally selected arias on each slide: 0 points for 0 to 5% positive cells, 1 for 5 to 25%, 2 for more than 25 to 75% and 3 points for more than 75 % cells. The average results of 10 tumor arias were rated with an immunohistochemical index representing each slide.
Comparison of the MELF group and diffuse group Ck19 and CD44 expression was statistically analyzed, using c2 - test (calculated by SPSS software). Values of p<0.05 were considered significant.
RESULTS
CK19
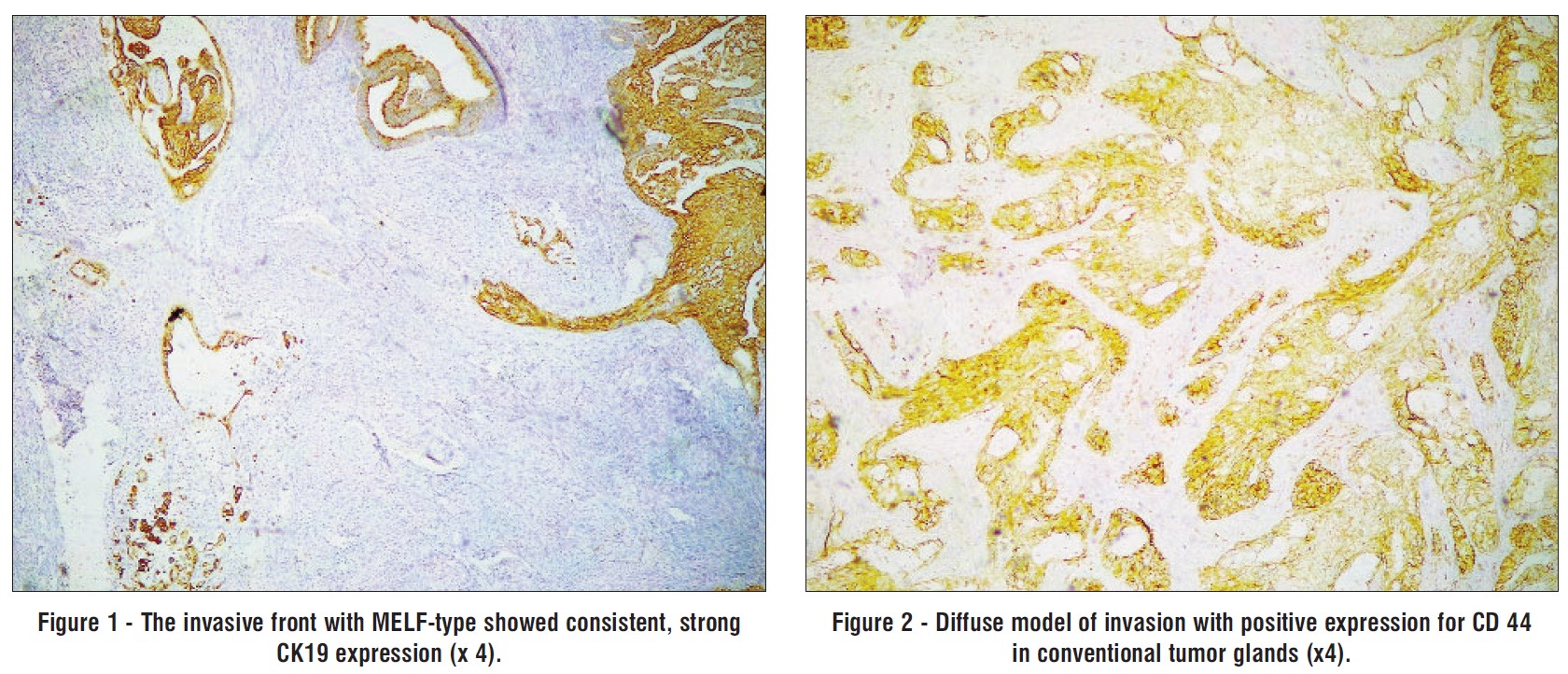
In the MELF group, all ECs were positive for CK19 in conventional tumor glands with a heterogenous staining pattern. Ten tumors (62. 5%) expressed CK19 in diffuse fashion, whereas the left 6 cases (37.5%) demonstrated focal staining (ranging from 10% to 30%). The invasive front with MELF-type showed consistent, strong type of expression for CK19 (fig. 1) in 15 cases (93.75%) and one case (6.25%) was focal type expression.
In the diffuse group, 6 tumors (42.8%) demonstrated diffuse type of expression for CK19, whereas the remaining 8 cases (57.2%) showed focal staining (ranging from 5% to 20%). In contrast to the conventional neoplastic glands, the tumor front showed 5 cases (35.7%) with diffuse expression of CK19 and 9 cases (64.3%) with focal type of expression.
CD44
In the MELF group, the conventional tumor glands were positive (ranging from 25% to approximately 90%) for CD44 in 11 cases (68.75%). The invasive front with MELF-type showed positive staining only in 2 cases (12.5%) and 14 cases (87.5%) showed very focal staining.
In the diffuse group, 12 tumors (85.7%) showed positive expression for CD 44 in conventional glands (fig. 2), whereas the remaining 2 cases (14.3%) showed focal staining. In contrast to the conventional neoplastic glands, the tumor front showed only 5 cases (35.7%) with positive expression and 9 cases (64.3%) with focal type of expression.
When the MELF group Ck19 tumor core (conventional glands) expression was compared to the diffuse group Ck19 tumor core (conventional glands) expression, no statistically significant difference was observed c2 = 2.1428, Df=1, p=0.1432 (table 3).
Statistically significant difference was observed between the MELF group Ck19 tumor invasive front expression and the diffuse group Ck19 tumor invasive front expression c2 = 13.6594, Df = 1, p < 0.0001. The MELF demonstrated predominantly diffuse Ck19 staining at the tumor periphery, while the diffuse type demonstrated predominantly focal CK19 staining at the tumor periphery (table 4).

When the MELF group CD44 tumor core (conventional glands) expression was compared to the diffuse group CD44 tumor core (conventional glands) expression, no statistically significant difference was observed c2=2.7121, Df=1, p=0.9959 (table 5).
When the MELF group CD44 tumor invasive front expression was compared to the diffuse group CD44 tumor invasive front expression, no statistically significant difference was observed c2 = 1.2054, Df=1, p=0.2723 (table 6).

DISCUSSION
Clement and Young have described the DI pattern of invasion which represents individually dispersed glands widely scattered throughout the myometrium (22). Quick et al. define this model as invasion by a single or small group of 3 or less glands with irregular contours that may be accompanied by desmoplastic stromal reaction (3). According to some authors DI pattern of invasion associated with advanced disease, high grade tumors (4), LVI, and tumor recurrence (3,23,24). Immunohistochemically DI pattern shows following immunophenotype – positive for CD44 and CD133 and negative for estrogen receptors (ER), progesterone receptors (PR), and decreased expression of E-cadherin which can be related to the induction of the epithelial-mesenchymal transition (EMT) process. Park et al. have identified a special type of stem cell (cancer stem cell CSCs), which is responsible for the processes of invasion, spread of tumor cells, and the development of resistance to conventional therapy. Also are described reciprocal interactions between tumor environment and the stromal matrix leading to proliferation of CSCs and initiation of EMT of the epithelial cells, followed by processes of invasion and metastasis, followed by an adaptive processes such as hormonal, chemotherapy, and radiotherapy resistance acquirement. CD44 and CD133 are useful for the identification of CSCs and their expression was closely associated with disease progression and poor prognosis (4,5). CD44 are cell-surface glycoproteins that affect structural and functional tissue organization and play role in cell migration and invasion. Alterations of adhesion intensity can free a cell from its environment and allow it to migrate and become invasive with parallel morphological transformation - a hallmark of carcinogenesis (4,5,24).
El-Shorbagy et al. investigated CD44 in endometrioid and serous EC in hysterectomy and curettage specimens. They noticed significantly stronger CD44 expression in endometrioid than in serous EC in both type specimens and they assumed that decrease CD44 in serous EC could be related to poor prognosis with a stronger tendency for deep MI. The biologic aggressiveness of this tumor type may, in part, be related to its lack of CD44 expression (7). In study of Ayhan et al. CD44v6 expression strongly correlated with lack of myometrial invasion. The authors suggest this could be marker for cancers with MI, that would be helpful for preoperative planning of lymphadenectomy. However, this contradicts to the hypothesis that increased vCD44 expression occurs in more advanced and aggressive tumors (25). Stokes et al. observed expression of standard CD44 and depth of MI to be inversely, but not significantly correlate (26). Leblanc et al. reported increase CD44 expression with increase depth of MI. They suggested that alterations of CD44 concentration could mainly be due to local process of invasion (27). ?hese different data may be due to distinct methodology and small patient number. In cases with cervical, serosal or adnexal involvement CD44 expression was not significantly affected, CD44 expression tended to be slightly less in both curettage and resected specimens, which suggested that CD 44 loses its expression in more invasive type of tumor (6,25).
It is reported that CD44 and some of its variants were expressed significantly more in early stage EC. However, CD44 expression decreased as the disease became invasive and aggressive (7). The results of our study tended to support this hypothesis. In our study in MELF group conventional glands showed 11(16) cases (68.75%) positive reaction for CD44 while in tumor front only 2(16) cases (12.5%). In DI group conventional glands with positive reaction in 12(14) cases (85.7%) and in invasive front - 5(14) cases (35.7%).
CK19 is widely used in diagnostic pathology, for example, in the differential diagnosis of thyroid neoplasms (mainly of papillary carcinoma) (16,28) and in the context of liver neoplasia (10% -15% of primary hepatocellular carcinomas are positive) and correlates with more aggressive clinical behavior (29). Stewart et al. investigated distribution of CK19 in normal endo-metrium and in endometrial endometrioid carcinoma. They found that CK19 was most strongly expressed in the functional layer and in the surface epithelium of normal endometrium, whereas the epithelium of basal zone was more weakly labeled or not stained. In this study all low-grade endometrioid carcinomas were CK19 positive but with some distinct microanatomic difference in its expression. Most of cases showed consistent CK19 expression in the conventional neoplastic glands (that formed the predominant tumor component) only within the central glandular areas, including intralumenal papillae and the epithelium lining internal glandular spaces. In contrast, the peripheral or basal zone of the larger neoplastic glands typically showed only focal staining, or were not stained. In cases of EC with MELF type MI CK19 showed strong diffuse cytoplasmic reactivity (16). Our study also confirmed that the invasive front with MELF-type showed strong CK19 expression in 15 cases (93.75%) while in DI the tumor front showed 5 cases (35.7%) with diffuse expression of CK19 and 9 cases (64.3%) with focal type of expression.
CK19 can be used as additive immunohistochemical marker in cases of MELF-type of invasion and may be useful in disclosing of the discreet focuses of myometrial involvement. (9,13,16). It is also useful for identifying intravascular tumor cells and the discrete lymph node involvement in EC with MELF type MI (16,21).
CONCLUSION
Recognition of this model and its inclusion in the pathological report is important to warn oncogynecologists about a possible worsening of the prognosis of the disease. Development of new methods to identify patients at high risk of metastases is needed.
Acknowledgements
The study was supported by a grant (D 4/2020) from Medical University – Pleven, Bulgaria.
Conflict of interest
All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Ethical consideration and Consent to participate
It was approved by the Commission for Scientific Research Ethics of Medical University, Pleven. All patients included in this study are signed informed consent.
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2019; 69(1):7-34.
2. Valerianova Z, Atanasov T, Vukov M. Incidence of cancer in Bulgaria, 2014 and 2015. Paradigma Publishing House; 2017. p. 216-219.
3. Quick CM, May T, Horowitz NS, Nucci MR. Low-grade, lowstage endometrioid endometrial adenocarcinoma: a clinicopathologic analysis of 324 cases focusing on frequency and pattern of
myoinvasion. Int J Gynecol Pathol. 2012;31(4):337-343.
4. Park JY, Hong D, Park JY. Association between morphological patterns of myometrial invasion and cancer stem cell markers in endometrial endometrioid carcinoma. Pathol Oncol Res. 2019; 25(1):123-130.
5. Amalinei C, Aignatoaei AM, Balan RA, Giusca SE, Lozneanu L, Avadanei ER, et al. Clinicopathological significance and prognostic value of myoinvasive patterns in endometrial endometrioid carcinoma. Rom J Morphol Embryol. 2018;59(1):13-22.
6. Wojciechowski M, Krawczyk T, Smigielski J, Malinowski A. CD44 expression in curettage and postoperative specimens of endometrial cancer. Arch Gynecol Obstet. 2015;291:383-390.
7. El-Shorbagy SH, Orieby R, EL-Shorbagy ShH. Expression of hormone receptors; p53 and CD44 in endometrial carcinoma and their prognostic significance. Life Science Journal. 2016;13(4):94-104.
8. Lee KR, Vacek PM, Belinson JL. Traditional and nontraditional histopathologic predictors of recurrence in uterine endometrioid adenocarcinoma. Gynecol Oncol. 1994;54(1):10-8.
9. Murray SK, Young RH, Scully RE. Unusual epithelial and stromal changes in myoinvasive endometrioid adenocarcinoma: a study of their frequency, associated diagnostic problems, and prognostic significance. Int J Gynecol Pathol. 2003;22(4):324-33.
10. Euscher E, Fox P, Bassett R, Al-Ghawi H, Ali-Fehmi R, Barbuto, et al. The pattern of myometrial invasion as a predictor of lymph node metastasis or extrauterine disease in low-grade endometrial carcinoma. Am J Surg Pathol. 2013;37(11):1728-1736.
11. Altunpulluk MD, Kir G, Topal CS, Cetiner H, Gocmen A. The association of the microcystic, elongated, and fragmented (MELF) invasion pattern in endometrial carcinomas with deep myometrial invasion, lymphovascular space invasion and lymph node metas-tasis. J Obstet Gynaecol. 2015;35:397-402.
12. Stewart CJ, Little L. Immunophenotypic features of MELF pattern invasion in endometrial adenocarcinoma: evidence for epithelial-mesenchymal transition. Histopathology. 2009;55:91-101.
13. Stewart CJ, Brennan BA, Leung YC, Little L. MELF pattern invasion in endometrial carcinoma: association with low grade, myoinvasive endometrioid tumours, focal mucinous differentiation and vascular invasion. Pathology. 2009;41(5):454-9.
14. Zaino RJ. Unusual patterns of endometrial carcinoma including MELF and its relation to epithelial mesenchymal transition. Int J Gynecol Pathol. 2014;33(4):357-364.
15. Stewart CJ, Crook ML, Leung YC, Platten M. Expression of cell cycle regulatory proteins in endometrial adenocarcinoma: variations in conventional tumor areas and in microcystic, elongated and fragmented glands. Mod Pathol. 2009;22(5):725-33.
16. Stewart CJ, Crook ML, Lacey J, Louwen K. Cytokeratin 19 expression in normal endometrium and in low-grade endometrioid adenocarcinoma of the endometrium. Int J Gynecol Pathol. 2011; 30(5):484-491.
17. Singh N, Hirschowitz L, Zaino R, Alvarado-Cabrero I, Duggan MA, Ali-Fehmi R, et al. Pathologic Prognostic Factors in Endometrial Carcinoma (Other Than Tumor Type and Grade). Int J Gynecol Pathol. 2019;38 Suppl 1: S93-S113.
18. Han G, Lim D, Leitao MM Jr, Abu-Rustum NR, Soslow RA. Histological features associated with occult lymph node metastasis in FIGO clinical stage I, grade I endometrioid carcinoma. Histo-pathology. 2014;64(3):389-398.
19. Joehlin-Price AS, McHugh KE, Stephens JA, Li Z, Backes FJ, Cohn DE, et al. The microcystic, elongated, and fragmented (MELF) pattern of invasion: a single institution report of 464 consecutive FIGO grade 1 endometrial endometrioid adenocarcinomas. Am J Surg Pathol. 2017;41(1):49-55.
20. Naki MM, Oran G, Tetikkurt SÜ, Sönmez CF, Türkmen Ï, Köse F. Microcystic, elongated, and fragmented pattern of invasion in relation to histopathologic and clinical prognostic factors in endometrioid endometrial adenocarcinoma. J Turk Ger Gynecol Assoc. 2017;18(3):139-142.
21. Pavlakis K, Messini I, Vrekoussis T, Panoskaltsis T, Chrysanthakis D, Yiannou P, et al. MELF invasion in endometrial cancer as a risk factor for lymph node metastasis. Histopathology. 2011;58(6):966-73.
22. Clement PB, Young RH. Endometrioid carcinoma of the uterine corpus: A review of its pathology with emphasis on recent advances and problematic aspects. Adv Anat Pathol. 2002;9(3):145-84.
23. Cole AJ, Quick CM. Patterns of myoinvasion in endometrial adenocarcinoma: Recognition and implications. Adv Anat Pathol. 2013; 20(3):141-7.
24. Mateva S, Nikolova M, Yordanov A. Patterns of Myometrial Invasion in Endometrial Adenocarcinoma with Emphasizing on Microcystic, Elongated and Fragmented (MELF) Glands Pattern: A Narrative Review of the Literature. Diagnostics (Basel). 2021;11(9):1707.
25. Ayhan A, Tok EC, Bildirici I, Ayhan A. Overexpression of CD44 variant 6 in human endometrial cancer and its prognostic significance. Gynecol Oncol. 2001;80(3):355-8.
26. Stokes GN, Shelton JB Jr, Zahn CM, Kendall BS. Association of CD44 isoform immunohistochemical expression with myometrial and vascular invasion in endometrioid endometrial carcinoma. Gynecol Oncol. 2002;84(1):58-61.
27. Leblanc M, Poncelet C, Soriano D, Walker-Combrouze F, Madelenat P, Scoazec JY, et al. Alteration of CD44 and cadherins expression: possible association with augmented aggressiveness and invasiveness of endometrial carcinoma. Virchows Arch. 2001;438(1):78-85.
28. Cheung CC, Ezzat S, Freeman JL, Rosen IB, Asa SL. Immunohistochemical diagnosis of papillary thyroid carcinoma. Mod Pathol. 2001;14(4):338-42.
29. Yoneda N, Sato Y, Kitao A, Ikeda H, Sawada-Kitamura S, Miyakoshi M, et al. Epidermal growth factor induces cytokeratin 19 expression accompanied by increased growth abilities in human hepatocellular carcinoma. Lab Invest. 2011; 91(2):262-72.
Full Text Sources:
Abstract:
Views: 2626

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.