Surgery, Gastroenterology and Oncology

|
|
Background: The selection of intracorporeal anastomosis (ICA) versus extracorporeal anastomosis (ECA) after laparoscopic right hemi-colectomy remains a debatable issue. We aimed to compare the early and late outcomes between the two different technical groups (ECA versus ICA) utilizing the propensity score matching analysis.
Methods: For the period from January 2013 to June 2023, we studied 90 consecutive patients who undertook laparoscopic right hemicolectomies. We classified them into ICA and ECA groups. Propensity score matching analysis was done, after which 21 patients were included in each group.
Results: The ICA group had greater operative time, but quicker recovery time, with shorter length of stay and less time to first motion. They also tolerated a soft diet faster and had slightly fewer postoperative complications. No inter-group differences were noted in mortality and readmission rates. The 1-, 3-, 5-years overall survival (OS) for ECA group were 100%, 100%, and 83.3% respectively. The 1-, 3-, 5-years OS for ICA group were 100%, 80%, 80% respectively (p=0.575). The 1-, 3-, 5-years disease free survival (DFS) for ECA group were 88.9%, 74.1% and 74.1% respectively. The 1-, 3-, 5-years disease free survival for ICA group were 94.7%, 86.1%, 86.1% respectively (p=0.72).
Conclusion: Laparoscopic right hemicolectomy with ICA has better postoperative recovery. The rate of recurrence, disease-free survival and overall survival were similar between ICA and ECA approaches. Laparoscopic right hemicolectomy with ICA is deemed a safe operation for lesions of the right colon.
Introduction
Total laparoscopic right hemi-colectomy is limited because of hand-sewing skills needed for intracorporeal anastomosis. Moreover, it is thought that ICA increases the operative time and chance of intra-abdominal contamination with tumor cells and bowel content. There have been no clear, published guidelines for choosing the type of anastomosis, and the choice between ECA or ICA stays a matter of taste for the surgeon performing the operation, contingent upon their personal preference and previous experience. A lot of studies have shown the short-term benefits of laparoscopic right hemicolectomy with ICA (1,2,3). Some of these include that ICA aids in avoiding pulling of the bowel through the small laparotomy wound and enables longer specimen and larger lymph node yields (3,4).
In this study, our aim was to assess the short- and long-term outcomes of different techniques of bowel anastomosis after total laparoscopic right hemi-colectomy. The primary outcome was to compare the overall incidence of anastomotic leakage between the two different technical groups. The secondary outcomes were to compare the postoperative recovery, morbidity, and oncologic outcomes between the two different technical groups.
Materials and methods
Patient selection
A total of 90 consecutive patients who underwent laparoscopic right hemicolectomies from January 2013 to June 2023 at Gastrointestinal Surgery Center (GISC), Department of Surgery, Mansoura University. The current study has received approval by the Local Ethical Committee and the Institutional Review Board of Faculty of Medicine, Mansoura University (MD.22.06.656).
Preoperative preparation and work upAll patients had a standard bowel preparation, which consists of chemical and mechanical preparation for two days prior to the operation. This was achieved by utilizing a liquid diet, purgatives, as well as using an intestinal antiseptic (namely: oral metronidazole 500 mg t.d.s), and enemas. Patients who had low albumin received albumin infusion, while those with low hemoglobin levels had preoperative blood transfusion to correct the deficits. For those patients who had a high risk for thromboembolism, they received prophylactic anticoagulant therapy a day before the procedure. Just before making the skin incision on the operation day, metronidazole along with third generation cephalo-sporin were given intravenously.
Operative technique
There are various positions to choose from for performing laparoscopic right hemicolectomy, with the mild Trendelenburg position with left side tilt being the preferred position. Four ports were utilized: The first was a 10-mm port above the umbilicus acting as a camera port. Two working ports were present on the left side in the midaxillary line: a 5-mm port in the left lower quadrant and a 12-mm port in the left upper quadrant for the stapler. An assistant 5 mm port in right lower quadrant in mid axillary line. The right colon dissection was performed in a medial-to-lateral direction. Complete mesocolic excision was the standard procedure along with central vascular ligation of the ileocolic vessels. Then, complete mobilization of ascending colon and right colic flexure was done. After division of ileum and colon with endo-stapler, the ileocolic anastomosis was achieved by using either ECA or ICA. The choice of ECA or ICA was dependent on the surgeon’s preference.
In the ECA group, either a transverse supraumbilical incision or a midline incision was used, along with utilizing a wound protector. The terminal ileum and right side of the colon were externalized, and the extracorporeal anastomosis was done by one of two ways: the main method was hand-sewing both ends in an isoperistaltic fashion. The other method which a few surgeons preferred was the stapled isoperistaltic side-to-side method.
In the ICA group, the terminal ileum and transverse colon ends were laparoscopically divided using Endo GIA staplers. Then, using the Endo GIA stapler, an isoperistaltic side-to-side anastomosis was performed. Barbed sutures by 3-0 V-Loc, PDS or vicryl were then used to close the common enterotomy channel. The specimen was then extracted extending a working port or through a of the Pfannenstiel incision.
Data collection
Data for this study was retrieved from the Ibn Sina hospital electronic management system supported with paper archives, Gastrointestinal Surgical Center, Mansoura University. This study received approval by the ethical committee of Mansoura Faculty of Medicine. Preoperative data included age, gender, body mass index, comorbidities, American Society of Anesthesiologists (ASA) Class, previous abdominal surgery, and preoperative laboratory tests. The operative variables included the operative technique, operative time, anastomosis methods, blood loss, and site of specimen extraction. The post operative pathological data included type of the pathology, lesion site, lesion size, tumor stage and grade, number of dissected lymph nodes, perineural invasion and lympho-vascular emboli and the length of colonic and ileal margins. Early outcomes included complications, time to first motion, time to tolerating soft diet, length of stay, early mortality, and readmission within 30 days of discharge.
Follow up
Ten days after discharge, the first follow-up visit took place to remove the stitches of the surgical wound and refer the patients to the nuclear medicine department to continue their chemo-radiotherapeutic plan according to the pathology report. All patients were followed-up by means which included abdominal ultrasound, colonoscopy, pelvi-abdominal computed tomography with contrast and tumor markers.
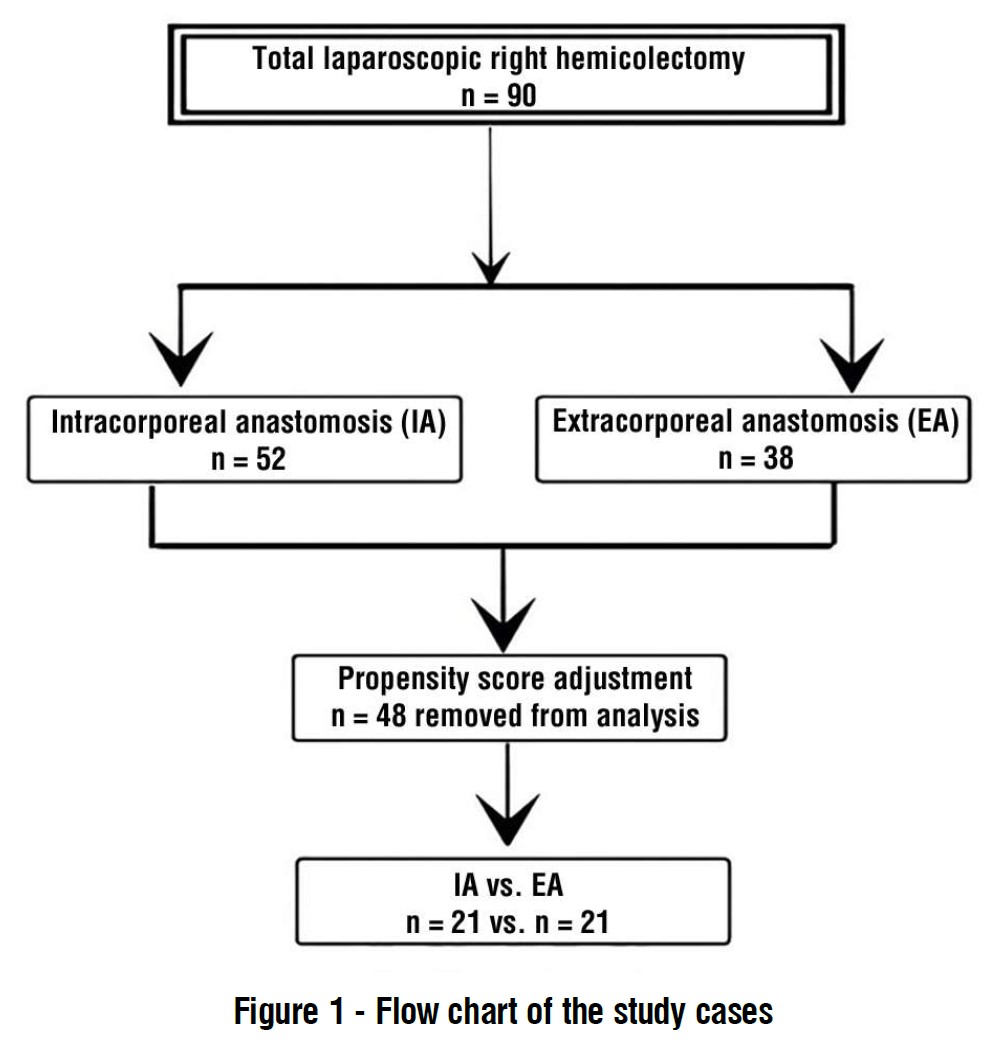
Figure 1 - Flow chart of the study cases
Statistical analysis
Statistical Package for Social Sciences (SPSS) version 24 was used for statistical analysis. A logistic regression model was used to perform Propensity score matching (PSM). The dependent variable was the type of anastomosis (ICA vs. ECA) and patients were matched 1:1. For comparisons between categorical variables, Pearson’s chi-squared test was utilized, while for continuous variables, independent sample t test was utilized. Kaplan-Meier curves with the log-rank test were used for survival analysis. Results were considered statistically significant when P was found to be less than 0.05.
Results
During the study period, 90 patients were included, 38 patients underwent ECA, and 52 patients underwent ICA. After PSM, each group included 21 patients as shown in
fig. 1.
Demographic data
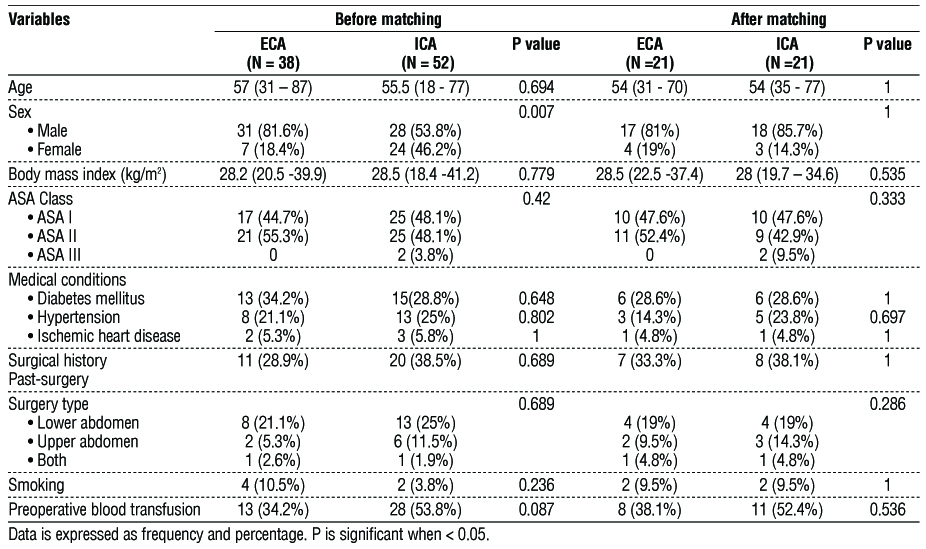
The demographics of patients of the study are shown in table 1. There was no significant difference in demographic data of the two groups.
Table 1 - Demographic characteristics of the patients
Operative parameters
After matching: the operative factors and their measurements are summarized in
table 2. All operative variables were non-significant between the two groups apart from anastomosis configuration, technique, type of sutures, incision type and length which showed a statistically significant difference between the two groups (p=0.001). The ECA group mainly used iso-peristaltic end to end or end to side hand sewn anastomosis and to less point side to side iso-peristaltic anastomosis with a staple with a barbed suture, but the ICA group predominantly used side to side iso-peristaltic anastomosis with a staple with a barbed suture (100%). In the ECA group, specimens were extracted from the transverse incision 61.9% of patients. The other incisions that were used included upper midline incision (23.8%) and right subcostal incision (14.3%). In the ICA group, specimen extraction was performed by a Pfannenstiel incision in 90.5% of the patients and port extension in 9.5%.
Table 2 - Operative parameters of the study patients

Pathological parameters
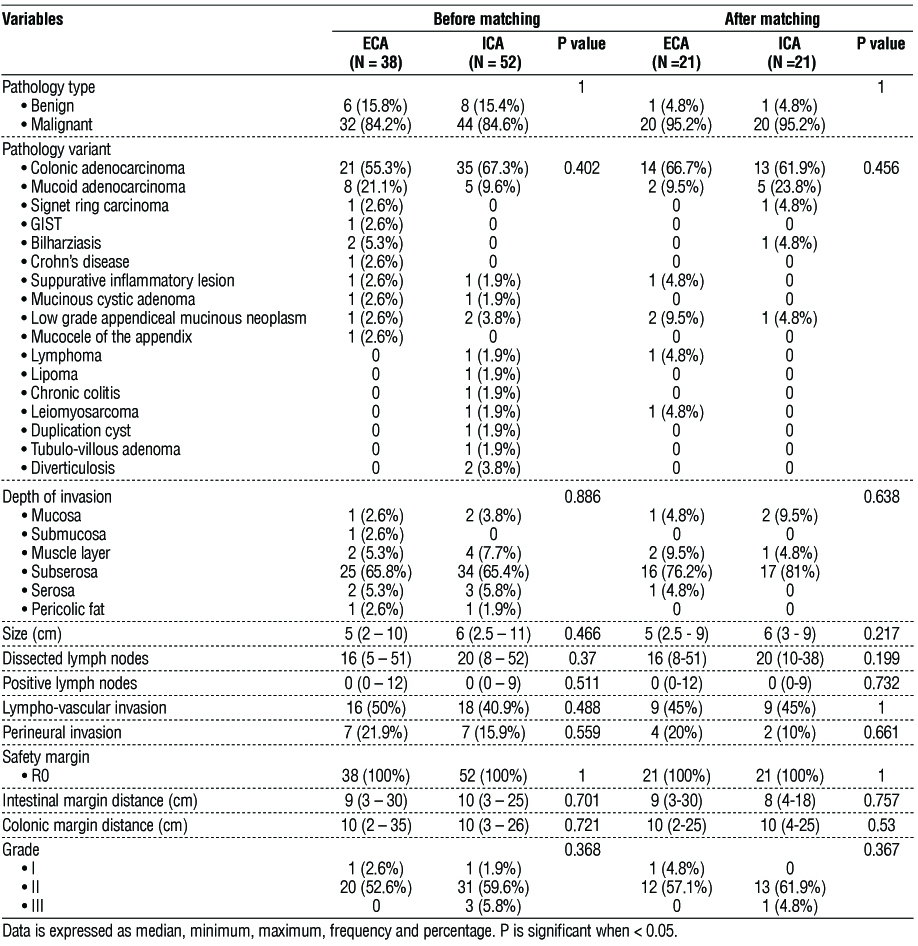
There were no significant differences in the tumor size, site, stage, grade, perineural invasion and lympho-vascular emboli between the ECA and ICA groups. The colon margin length, the ileum margin length were not statistically significant between the two groups (table 3).
Table 3 - Pathological parameters of the study patients
Short-term outcomes
The short-term outcomes and postoperative complications are shown in table 4. After matching: Recovery of bowel functions was faster in ICA group (2 days vs. 3 days in the other group respectively, p=0.045), which allowed early oral intake in ICA group at the 3rd POD compared to 4th POD in the other group, p=0.002. Post operative hospital stay (LOS) was significantly shorter in ICA group (p=0.004).
Table 4 - Postoperative outcomes of the study patients
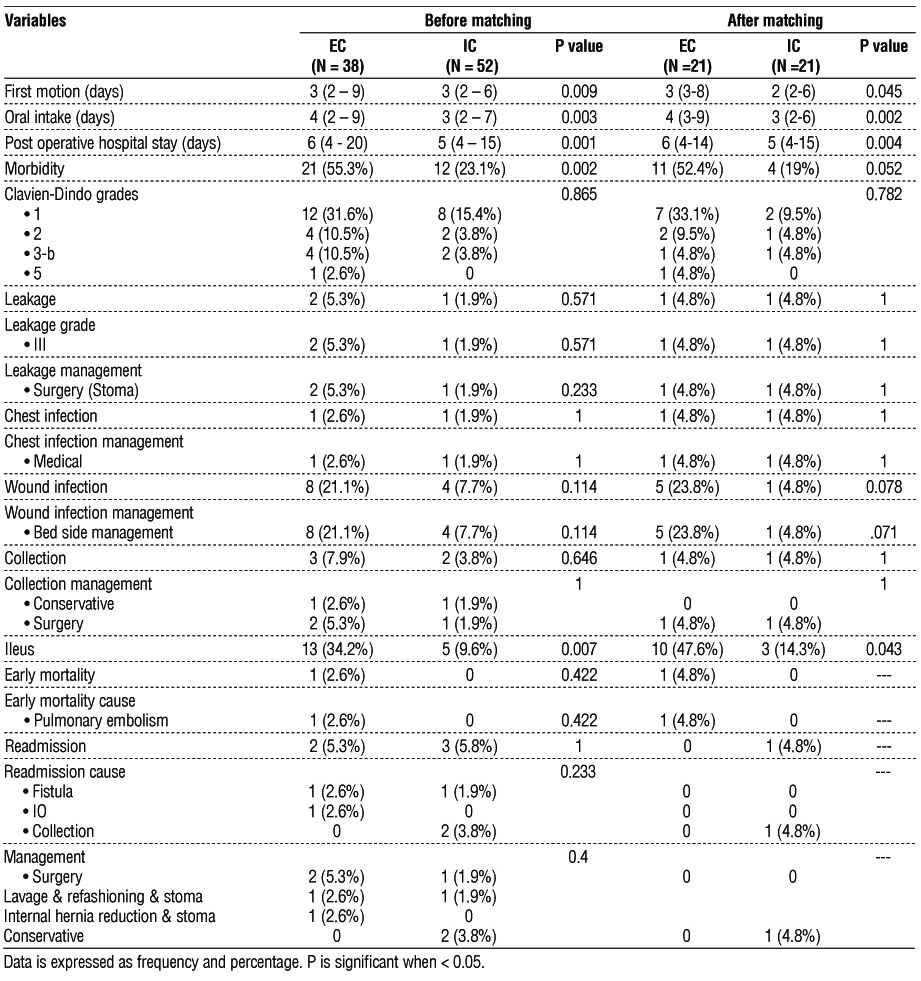
No difference among severe complications (Clavien-Dindo grade ≥ 3) was observed between the two groups (4.8% vs. 4.8%, p=0.782). The major complication in both groups was prolonged postoperative ileus, with higher incidence observed in ECA group (47.6% vs. 14.3%, p=0.043). All patients commenced conservative treatment. Two patients experienced intra-abdominal infection and collection. One patient in each group presented with anastomotic leakage and required re-exploration and stoma. one patient in the ICA group presented with collection and required readmission for conservative management. Early mortality occurred in single case of ECA group.
Long-term outcomes
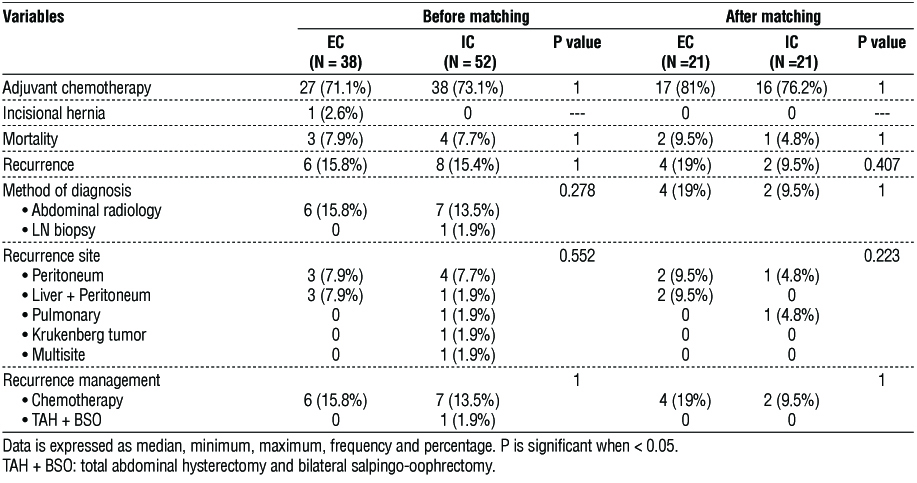
The long-term outcomes are summarized in table 5. Before matching, one incisional hernia occurred during follow-up periods in the ECA group, whereas no incisional hernia occurred in the ICA group. Post matching, the median follow-up times were 14 months and 23 months in the ICA group and ECA group, respectively. There were 2 recurrences found in the ICA group and 4 in the ECA group, all commenced chemotherapy.
Table 5 - Long-term outcomes of the study patients
Survival outcomes
Disease Free Survival (DFS)
* Before Matching:
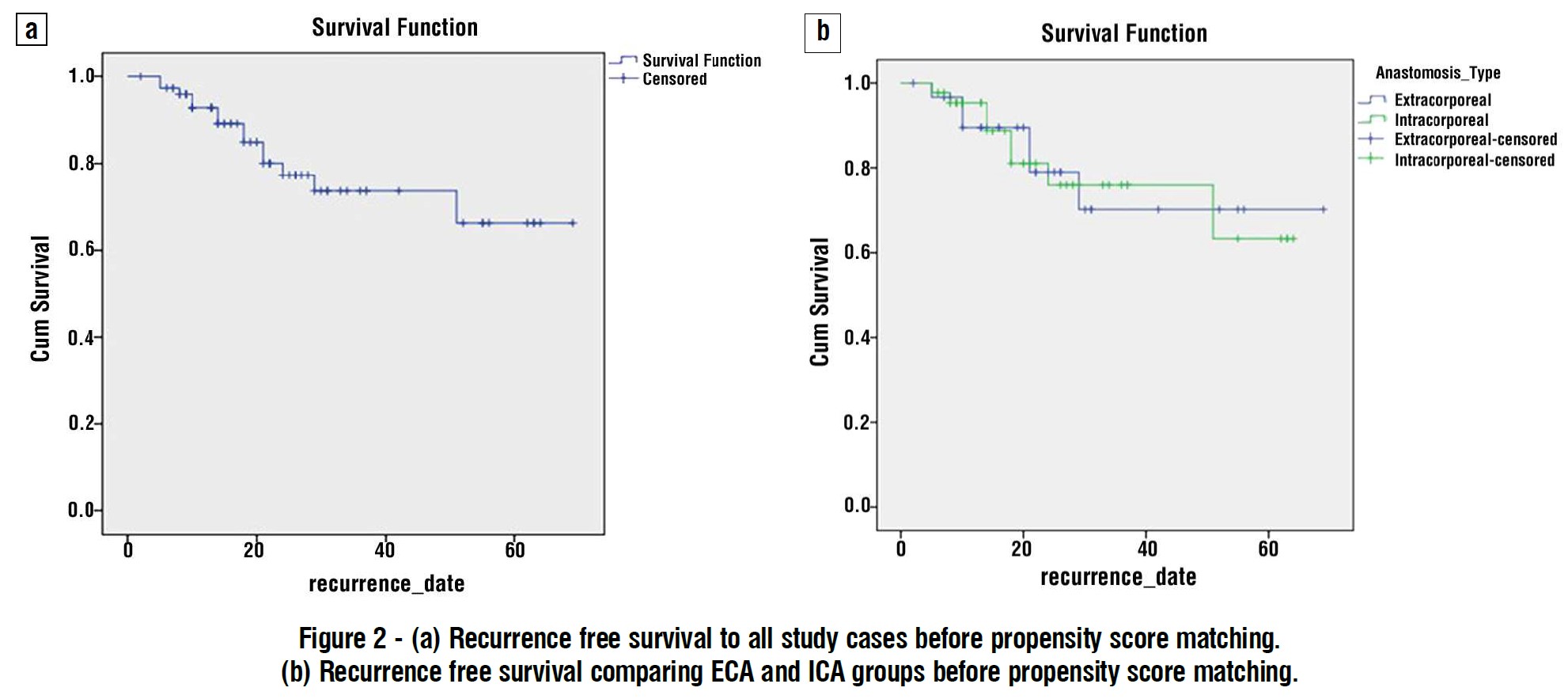
All study cases: 1-, 3-, 5-years DFS rates were 92.8%, 73.6%, and 66.3% respectively (fig. 2 a). The 1-, 3-, 5-years DFS rates for ECA group were 89.5%, 70.2%, 70.2% respectively. The 1-, 3-, 5-years DFS rates for ICA group were 95.3%, 76%, 63.3% respectively. There was no significant difference between the two groups (Log Rank: Chi Square = 0.003, df = 1, p = 0.955) (fig. 2 b).
Figure 2 - (a) Recurrence free survival to all study cases before propensity score matching. (b) Recurrence free survival comparing ECA and ICA groups before propensity score matching.
* After Matching:
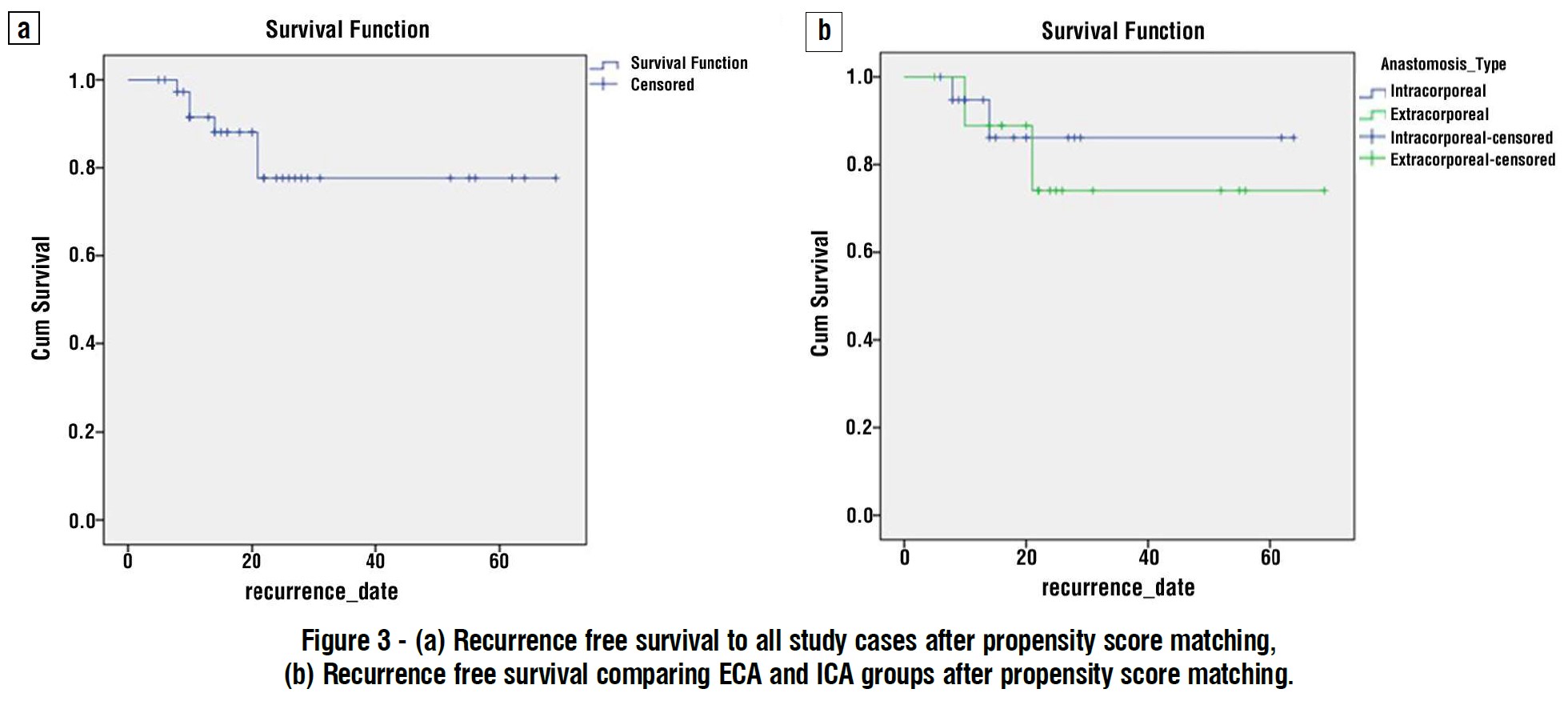
All study cases: 1-, 3-, 5-years disease free survival were 91.4%, 77.7%, and 77.7% respectively (fig. 3 a). The 1-, 3-, 5-years disease free survival for ECA group were %, 88.9%, 74.1% and 74.1% respectively. The 1-, 3-, 5-years disease free survival for ICA group were 94.7%, 86.1%, 86.1% respectively. There was no significant difference between the two groups (Log Rank: Chi Square = 0.129, df=1, p=0.72) (fig. 3 b).
Overall Survival (OS)
* Before Matching:
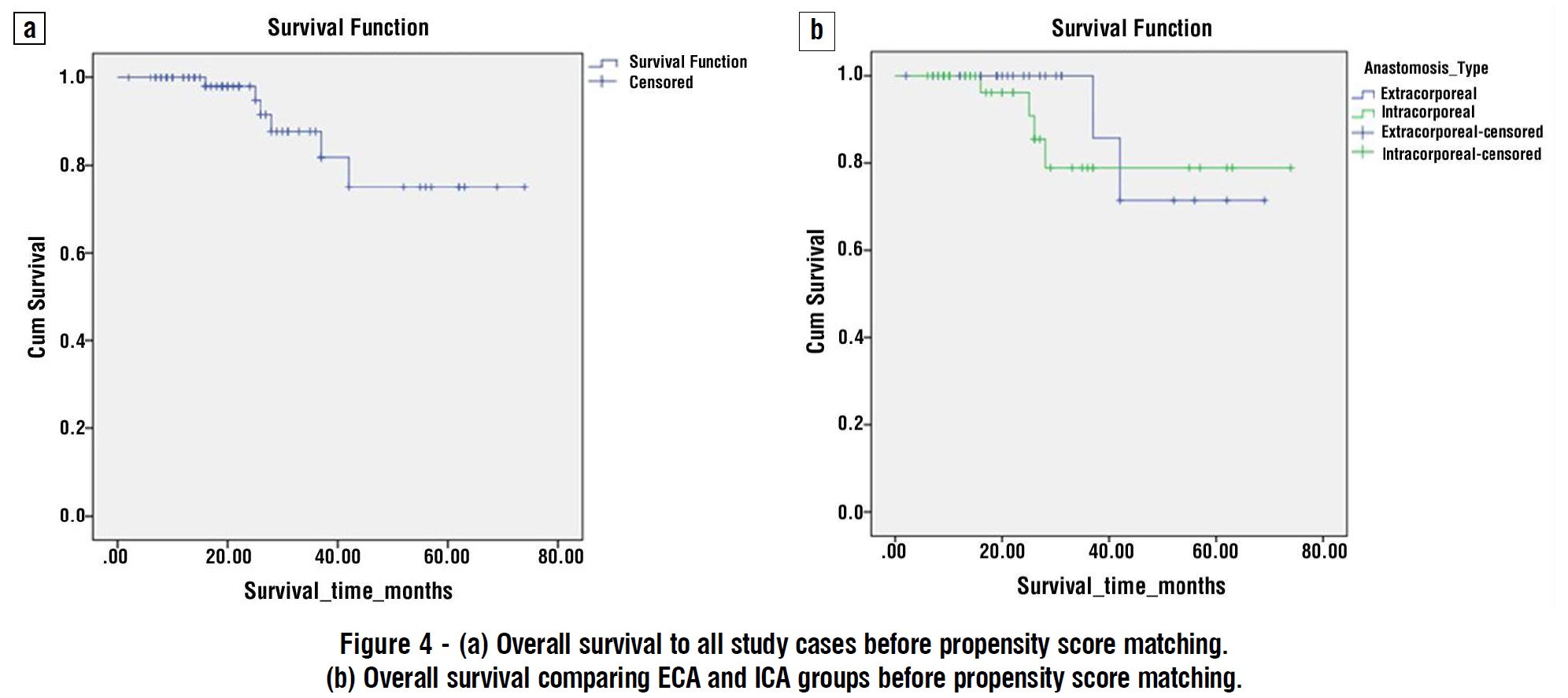
All study cases: 1-, 3-, 5-years OS rates were 100%, 87.7%, and 75% respectively
(fig. 4 a). The 1-, 3-, 5-years OS rates for ECA group were 100%, 85.7%, 71.4% respectively. The 1-, 3-, 5-years OS rates for ICA group were 100%, 78.9%, 78.9% respectively. There was no significant difference between the two groups (Log Rank: Chi Square = 0.347, df=1, p=0.556) (fig. 4 b).
* After Matching:
All study cases: 1-, 3-, 5-years OS rates were 100%, 92.3.7%, and 80.8% respectively (fig. 5 a). The 1-, 3-, 5-years OS rates for ECA group were 100%, 100%, 83.3% respectively. The 1-, 3-, 5-years OS rates for ICA group were 100%, 80%, 80% respectively. There was no significant difference between the two groups (Log Rank: Chi Square = 0.315, df=1, p=0.575) (fig. 5 b).

Discussion
Bergamaschi et al. published a total laparoscopic right colectomy with ICA for cancer colon in 2008 and mentioned favorable short-term results (1). This study was carried out in Mansoura University at the Gastrointestinal Surgical Center, with the aim of comparing the short-term and long-term outcomes in patients who had right-sided colon lesions and then underwent laparoscopic right hemicolectomy with ICA with those who underwent the same procedure but with ECA.
Our results have demonstrated that the median operative time for the ICA group was longer than in the ECA group. This is primarily due to requiring laparoscopic hand-sewing skills inside the abdominal cavity. The fact that ICA prolongs the surgical time has been previously mentioned by several studies (1,3,5,6).
ECA requires exteriorization of the ileum and colon for performing the anastomosis; consequently, the transverse incision is typically longer than in the ICA. In our study, length of incision was relatively longer in ECA group vs the ICA group (7 cm vs. 5 cm, p=0.001). When performing an ICA, the incision was smaller and had a better cosmetic outcome. In our center, we prefer the Pfannenstiel incision for specimen extraction as it has been our experience that it leads to better postoperative outcomes as well as better cosmetic results. Other authors have stated that patients with lower abdominal incisions tend to report experiencing fewer complications and less pain (7,8). During the follow-up of the study patients, a single case incisional hernia was diagnosed in of the ECA group, which agrees with the reports of previous studies (7,9).
In our study, ICA group showed early bowel motion and early oral intake, which is similar to that found in other studies (3,10,11). This is attributed to more manipulation and dissection of the transverse colon and small bowel to allow their easy extraction of them through the mini-abdominal incision in case of ECA. Also, excess mesenteric traction and hand manipulation of the bowel in case of ECA.
After reviewing the post operative pathology, the number of lymph nodes harvested was similar in both groups, which is in agreement with what was reported by other studies (3,10). In our study, there was no significant difference in the length of colonic and intestinal margins between the ECA and ICA groups, which is consistent with Allaix et al. findings (12) but, contrary to Biondi et al. who stated that the margins lengths were longer in the ICA method (4). In this study, the length of stay was significantly shorter in the ICA group compared to the ECA group (median 5 days vs. 6 days, p=0.001). Many authors revealed the same results in systemic reviews and meta-analyses (9,13-17).
In our study after PSM, the ECA group showed slightly greater overall morbidity than the ICA group (52.4% vs 19% respectively), but it was not statistically significant (p=0.052). Other studies showed similar results (18,19). In our study, we did not find a statistically significant difference in anastomotic leakage between the two groups, which is consistent with other studies (15,20,21). In our study, ECA group patients had a significantly higher incidence of postoperative ileus (47.6% vs. 14.3%, p=0.043). Other studies showed similar results (22,23). The prevalence of postoperative wound contamination was higher in ECA group (23.8% vs. 4.8%, p=0.078). This agrees with the reporting of Ricci et al. (24).
In our study, the overall survival and disease-free survival showed no statistically significant difference between the two groups. This is in agreement with Hanna et. al, who showed that the 5-year overall survival for the ICA & ECA groups showed no significant difference (66% vs. 78%, p=0.698) and showed the same for the disease-free survival (86% vs. 78%, p= 0.999) (10). This was similarly reported by Anania et al. (25).
The main limitation of this study lies in its retrospective nature; however, by using PSM, the variables used for analysis for both groups were the same. The choice of ECA and ICA and the anastomosis technique and configuration were dependent on the surgeon’s preference. The difference in some variables between the reported literature and our findings could be attributed to the small sample size of this study and that it is a single center experience. To prove these findings, we recommend larger, prospective, multi-center studies to be carried out.
Conclusions
Laparoscopic right hemicolectomy with ICA has better postoperative recovery and provides an assortment of incisions to choose from for specimen extraction. The rate of recurrence, disease-free survival and overall survival were similar between ICA and ECA approaches. Laparoscopic right hemicolectomy with ICA is deemed a safe operation for lesions of the right colon.
Conflicts of interest
All authors declare no conflicts of interest.
Funding
No external funding resources for research.
References
1. Bergamaschi R, Schochet E, Haughn C, Burke, M, Reed JF, Arnaud JP. Standardized laparoscopic intracorporeal right colectomy for cancer: short-term outcome in 111 unselected patients. Dis Colon Rectum. 2008;51(9):1350-5.
2. Lee KH, Ho J, Akmal Y, Nelson, R, Pigazzi A. Short-and long-term outcomes of intracorporeal versus extracorporeal ileocolic anastomosis in laparoscopic right hemicolectomy for colon cancer. Surg Endosc. 2013;27(6):1986-90.
3. Magistro C, Di Lernia S, Ferrari G, Zullino A, Mazzola M, De Martini P, et al. Totally laparoscopic versus laparoscopic-assisted right colectomy for colon cancer: is there any advantage in short-term outcomes? A prospective comparative assessment in our center. Surg Endosc. 2013;27(7):2613-8.
4. Biondi, A, Santocchi P, Pennestrì F, Santullo F, D’Ugo D, Persiani R. Totally laparoscopic right colectomy versus laparoscopically assisted right colectomy: a propensity score analysis. Surg Endosc. 2017;31(12):5275-5282.
5. Shapiro R, Keler U, Segev L, Sarna S, Hatib K, Hazzan D. Laparoscopic right hemicolectomy with intracorporeal anastomosis: short-and long-term benefits in comparison with extracorporeal anastomosis. Surg Endosc. 2016;30(9):3823-9.
6. Cleary RK, Kassir A, Johnson CS, Bastawrous AL, Soliman MK, Marx DS, et al. Intracorporeal versus extracorporeal anastomosis for minimally invasive right colectomy: A multi-center propensity score-matched comparison of outcomes. PLoS One 2018; 13(10):e0206277.
7. Orcutt ST, Balentine CJ, Marshall CL, Robinson CN, Anaya DA, Artinyan A, et al. Use of a Pfannenstiel incision in minimally invasive colorectal cancer surgery is associated with a lower risk of wound complications. Tech Coloproctol. 2012;16(2):127-32.
8. Benlice C, Stocchi L, Costedio MM, Gorgun E, Kessler H. Impact of the specific extraction-site location on the risk of incisional hernia after laparoscopic colorectal resection. Dis Colon Rectum. 2016; 59(8):743-50.
9. Milone M, Elmore U, Di Salvo E, Delrio P, Bucci L, Ferulano GP, et al. Intracorporeal versus extracorporeal anastomosis. Results from a multicentre comparative study on 512 right-sided colorectal cancers. Surg Endosc. 2015;29(8):2314-20.
10. Hanna MH, Hwang GS, Phelan MJ, Bui TL, Carmichael JC, Mills SD, et al. Laparoscopic right hemicolectomy: short-and long-term outcomes of intracorporeal versus extracorporeal anastomosis. Surg Endosc. 2016;30(9):3933-42.
11. Mari GM, Crippa J, Costanzi A, Pellegrino R, Siracusa C, Berardi V, et al. Intracorporeal anastomosis reduces surgical stress response in laparoscopic right hemicolectomy: a prospective randomized trial. Surg Laparosc Endosc Percutan Tech. 2018;28(2):77-81.
12. Allaix ME, Degiuli M, Bonino MA, Arezzo A, Mistrangelo M, Passera R, et al. Intracorporeal or extracorporeal ileocolic anastomosis after laparoscopic right colectomy: a double-blinded randomized controlled trial. Ann Surg. 2019;270(5):762-767.
13. Feroci F, Lenzi E, Garzi A, Vannucchi A, Cantafio S, Scatizzi M. Intracorporeal versus extracorporeal anastomosis after laparos-copic right hemicolectomy for cancer: a systematic review and meta-analysis. Int J Colorectal Dis. 2013;28(9):1177-86.
14. van Oostendorp S, Elfrink A, Borstlap W, Schoonmade L, Sietses C, Meijerink J, et al. Intracorporeal versus extracorporeal anastomosis in right hemicolectomy: a systematic review and meta-analysis. Surg Endosc. 2017;31(1):64-77.
15. Wu Q, Jin C, Hu T, Wei M, Wang Z. Intracorporeal Versus Extracorporeal Anastomosis in Laparoscopic Right Colectomy: A Systematic Review and Meta-Analysis. J Laparoendosc Adv Surg Tech A. 2017;27(4):348-357.
16. Vergis AS, Steigerwald SN, Bhojani FD, Sullivan PA, Hardy KM. Laparoscopic right hemicolectomy with intracorporeal versus extracorporeal anastamosis: a comparison of short-term outcomes. Canadian journal of surgery. Can J Surg. 2015;58(1):63-8.
17. Widmar M, Aggarwal P, Keskin M, Strombom PD, Patil S, Smith JJ, et al. Intracorporeal anastomoses in minimally invasive right colectomies are associated with fewer incisional hernias and shorter length of stay. Dis Colon Rectum. 2020;63(5):685-692.
18. Emile SH, Abdallah EM, Shalaby M, Sakr A, Bassuni M, Christensen PR et al. Intracorporeal versus extracorporeal anastomosis in minimally invasive right colectomy: an updated systematic review and meta-analysis. Tech Coloproctol. 2019;23(11):1023-1035.
19. Vallribera F, Kraft M, Pera M, Vidal L, Espín-Basany E. Outcomes of Intra- versus Extra-Corporeal Ileocolic Anastomosis after Minimally Invasive Right Colectomy for Cancer: An Observational Study. J Clin Med. 2021;10(2):307.
20. Creavin B, Balasubramanian I, Common M, McCarrick C, El Masry S, Carton E, et al. Intracorporeal vs extracorporeal anastomosis following neoplastic right hemicolectomy resection: a systematic review and meta-analysis of randomized control trials. Int J Colorectal Dis. 2021;36(4):645-656.
21. Zheng JC, Zhao S, Chen W, Tang Y, Wang YY, Wu JX. Comparison of intracorporeal and extracorporeal anastomosis and resection in right colectomy: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021;406(6):1789-1801.
22. Bollo J, Turrado V, Fueyo AR, Carrillo EH, Gich, I, Martínez MC, et al. Randomized clinical trial of intracorporeal versus extracorporeal anastomosis in laparoscopic right colectomy (IEA trial). Br J Surg. 2020;107(4):364-372.
23. Zhang T, Sun, Y, Mao W. Meta-analysis of randomized controlled trials comparing intracorporeal versus extracorporeal anastomosis in minimally invasive right hemicolectomy: upgrading the level of evidence. Int J Colorectal Dis. 2023;38(1):147.
24. Ricci C, Casadei R, Alagna V, Zani E, Taffurelli G, Pacilio CA, et al. A critical and comprehensive systematic review and meta-analysis of studies comparing intracorporeal and extracorporeal anastomosis in laparoscopic right hemicolectomy. Langenbecks Arch Surg. 2017; 402(3):417-427.
25. Anania G, Tamburini N, Sanzi M, Schimera A, Bombardini C, Resta G, et al. Extracorporeal versus intracorporeal anastomosis in laparoscopic right hemicolectomy for cancer. Minim Invasive Ther Allied Technol. 2022;31(1):112-118.
Full Text Sources:
Abstract:
Views: 2554

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.