Surgery, Gastroenterology and Oncology

|
|
Introduction: Constipation is a common health issue, with most causes considered functional. Some cases of constipation are complicated by a redundant sigmoid colon and rectal prolapse, which exacerbate symptoms and management. A redundant sigmoid colon is often asymptomatic but can lead to many complications. The combination of these three conditions is rarely reported in medical literature; however, understanding how to select effective therapies and reduce the risk of long-term complications is crucial.
Case report: We report a case of an 18-year-old male with chief complaints of difficulty defecating for an extended period, accompanied by abdominal pain. The patient has experienced hard stools and often expresses feelings of incomplete evacuation along with abdominal discomfort. He has had similar complaints since the second grade in elementary school, which necessitated medication to facilitate bowel movements. Additionally, he underwent hemorrhoid surgery a year ago due to bleeding and a persistent anal protruding mass. His mother denied any history of Hirschsprung disease. Upon physical and radiological examination, a diagnosis of redundant sigmoid with rectal prolapse was made. The patient was scheduled for laparoscopic resection and mesh rectopexy.
Conclusion: Chronic constipation in young adults require evaluation, especially if there are indications of anatomical complications such as redundant sigmoid colon and rectal prolapse. Operative management and multidisciplinary care can improve quality of life and prevent long-term complications. Operative management in this case is expected to improve functional capacity in young adults.
Introduction
Individuals have an average colon length of 120-150 centimeters in the abdominal cavity (1). The colon has a winding structure that allows it to fit within the abdomen. Abnormal conditions can cause the length of the intestine to exceed its usual limits, resulting in a redundant colon (2,3). Redundant colon can affect the entire colon or be restricted to specific areas such as the hepatic flexure, transverse colon, splenic flexure, or the distal portion of the colon. The transverse and sigmoid colons are the most frequently involved areas (4).
The redundant colon has additional loops, which can prolong the process of defecation, leading to constipation (3).
Constipation is a common problem, especially in children and elderly, with a prevalence of 1-30% worldwide (5,6). The etiology of constipation includes several systemic diseases or malformations of the intestinal tract, such as anal stenosis or colonic aganglionosis, but constipation can occur without organic etiology called functional constipation and can occur in 30-95% of children (6,7). Studies examine the etiology of functional constipation by evaluating colonic function, including transit time, speed, and anatomical factors, by measuring the diameter and length of the segment (6).
Some cases of constipation are complicated by redundant sigmoid colon and rectal prolapse, worsening symptoms, and complicated management. Rectal prolapse can occur in constipation due to increased intra-abdominal pressure resulting from straining (8). Management varies according to the primary etiology. It may include operative management of anal stenosis and colonic aganglionosis, local management of internal anal sphincter (IAS) hypertonia and anal fissures, as well as medical management. Identification of the etiology is essential to ensure effective management (6). This case report found a pediatric patient with rectal prolapse due to chronic constipation complicated by a redundant colon. This case report aims to determine effective operative management, especially in adults and young adults.
Case Report
An 18-year-old male came with chief complaints of difficulty defecating 2 weeks before admission. The patient has had hard stools and often complains of feeling an incomplete evacuation and abdominal pain.
The patient had experienced similar complaints since grade 2 of Elementary School, which required laxatives to facilitate defecation. Hirschsprung’s disease was ruled out in the early days; however, the examination during that time was lost. The patient rarely consumed fiber and often ate fast food. The patient had a history of anal surgery 1 year ago due to a persistent anal protruding mass accompanied by bleeding. He was told it was hemorrhoid surgery.
However, we were unable to confirm it. A couple of months after the surgery, the protruding anal mass reappeared, and a picture was taken (fig. 1). The patient was then referred to us. However, when he was seen at the clinic, the protruding mass reduced with conservative care, including sitz baths and laxatives. A history of diabetes mellitus, heart disease, kidney disease, trauma, or malignancy in the patient or family was denied.
Figure 1 - Clinical image of prolapse recti in this patient

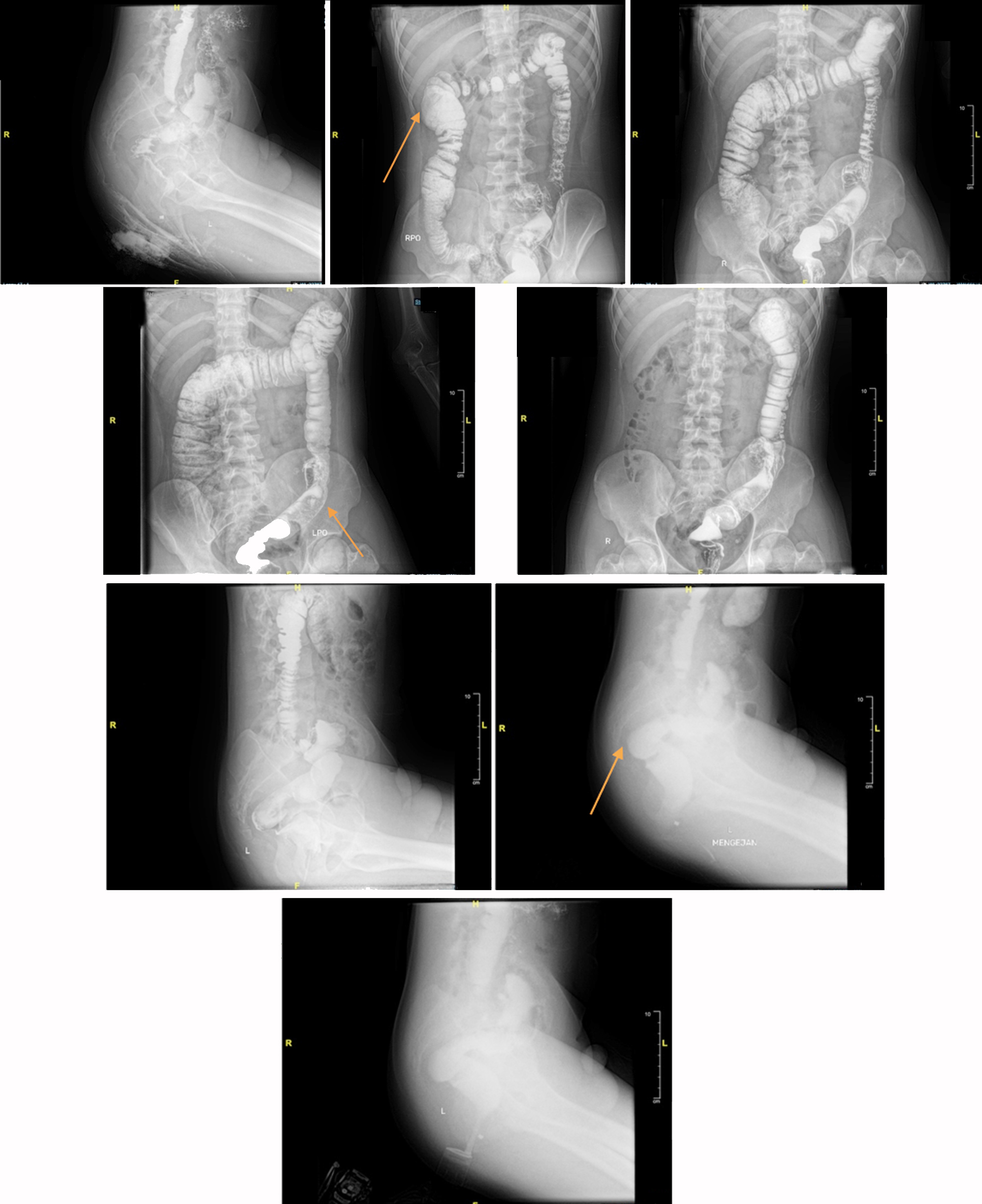
The patient had no difficulty with flatus, and there was no disturbance in urination. Vital signs were within normal limits. Physical abdominal examinations revealed distension but no pain upon palpation, and bowel sounds during auscultation were normal. We consulted the Physical Medicine and Rehabilitation Division to assess the potential for pelvic floor dysfunction, and the results were negative. A barium enema examination was performed to rule out Hirschsprung’s disease. Evaluation of colon structure abnormalities through the barium enema revealed a redundant ascending colon, hepatic flexure, and sigmoid, with no dilatation or filling defects in the colon (fig. 2). A biopsy was also performed, resulting in no aganglionic tissue.
Figure 2 - Barium enema pre-operative (July 2024): redundant ascendence colon, hepatic flexure, and sigmoid with no dilatation of colon
The patient underwent laparoscopic resection and mesh rectopexy. Intraoperative exploration revealed a redundant sigmoid colon, which was noted to be spirally oriented. Rectal dissection was carried out along the holy plane up to the seminal vesicles, and a digital rectal examination was performed to assess the rectum, which was then retracted proximally. A ventral mesh was secured to the rectal serosa and the promontory, and the peritoneal reflection was subsequently closed. The sigmoid colon was released from lateral wall adhesions, and the left white line was incised until mobilization was achieved. A left lower abdominal incision was made, and the resection of the sigmoid colon and proximal rectum was followed by an anastomosis of the descending colon to mid-rectum using a linear stapler. Re-evaluation found no evidence of bleeding or an abnormal rectal slope. The patient was discharged eight days postoperatively and was scheduled for regular follow-up appointments to monitor for any postoperative complications, including stricture or infection, and to ensure proper gastro-intestinal function. This approach is anticipated to yield optimal long-term outcomes and enhance the patient’s overall quality of life.
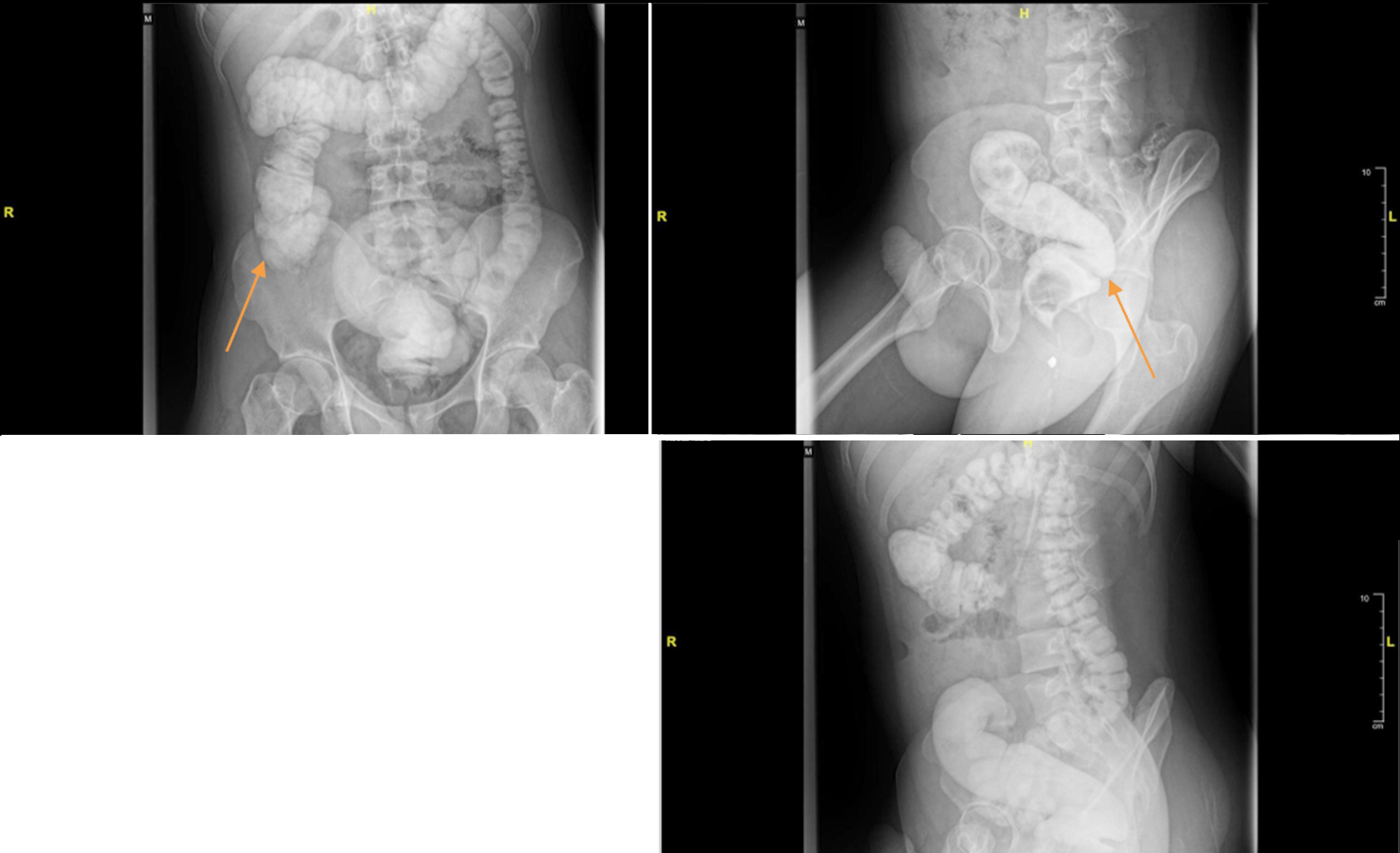
A barium enema evaluation was performed two months post-operative. The results showed no significant stenosis or filling defect in the visualized colon, with no visible redundancy of the sigmoid (fig. 3).
Figure 3 - Barium enema post-operative (September 2024): no stenosis and filling defect on the visualized colon with no visible redundancy of the sigmoid compared to pre-operative (shown with the orange arrow).
Discussion
Constipation remains a common problem, especially in children and the elderly, with a prevalence of 1-30% worldwide (5,6).
Constipation is far more common among the elderly than among younger people. Common causes of constipation in the elderly are linked to several factors, including lack of regular bowel movements, aging, pelvic floor weakness, lack of proper diet, lack of adequate fluid intake, lack of sufficient physical activity, illness, or the use of drugs. The prevalence of this condition is higher in adults over 65 years of age, often due to loose-fitting dentures or tooth loss, resulting in chewing difficulty that forces patients to select soft and flexible fiber materials. Individuals who have lost their appetite or are experiencing difficulty swallowing often consume low-fiber foods (9).
Rome IV symptom-based criteria are used to diagnose functional constipation. A low-fiber diet, lack of physical activity, and changes in the gut microbiome can also trigger constipation. The primary pathophysiological mechanism involves stool withholding, accompanied by alterations in rectal function, the anal sphincter, the pelvic floor, and colonic dysfunction (10). Similar to the data presented above, the patient in this case report exhibited that inadequate fiber intake led to constipation. Functional constipation carries a financial burden and negatively impacts the adult health-related quality of life (10). Some cases of constipation are complicated by redundant colon, particularly the sigmoid colon, and rectal prolapse, which exacerbate symptoms and complicate management. Colonic redundancy can affect the entire colon or only certain areas, including the hepatic flexure, transverse colon, splenic flexure, or distal colon, with the transverse and sigmoid colon being the most commonly involved areas (4). Colonic redundancy creates additional loops, resulting in a prolonged stool elimination process that contributes to constipation (3).
The colon is part of the intestine that stores stool and absorbs fluid; therefore, patients with colonic redundancy experience greater water reabsorption, resulting in harder stool consistency (6). This requires management, such as advanced fluid balancing, stool softeners, or laxatives, and often leads to chronic constipation (4). In this case, the patient has suffered from chronic constipation since elementary school up to the present, with a history of using laxatives to facilitate defecation.
Several authors note that the etiology of redundant colon is primarily congenital; however, function and fecal transport may also contribute to some changes. Colon growth is tied to activity and depends on diet. Recently, research demonstrated in mice that the large bowel undergoes significant changes in length as it fills with fecal matter, and the stretching of longitudinal muscles leads to slow colonic transit (11).
Nevertheless, in this case, functional constipation occurs in a young adult aged 18 years, progressing to rectal prolapse. This suggests that dietary changes and a sedentary lifestyle may be contributing factors. According to the study by Zhang Y et al., students aged 18-21 years are at a higher risk for functional constipation. In addition to dietary habits and physical activities, the study indicates that sleep patterns exhibit a bidirectional relationship with constipation. University students with functional constipation often experience poor sleep quality due to increased screen time from electronic devices right before bed, engaging in activities like chatting, gaming, and online shopping. Furthermore, academic pressures, work, and social interactions contribute to reduced sleep duration and quality, leading to sleep disorders, intestinal dysfunction, and a higher likelihood of functional constipation. It may also contribute to shorter sleep duration and poorer sleep quality due to the effects of functional constipation, resulting to a vicious cycle. This suggests that both lifestyle factors, such as diet and sleep, play significant roles in the development of functional constipation among university students (12).
Operative management for these conditions became a last resort. Charalampopoulos A. et al. presented cases of 12 patients, with a mean age of 32 years, all of whom had a history of psychiatric disease, constipation, and a redundant sigmoid colon on endoscopy. The surgical treatment applied in all cases was an anterior resection of the rectum and the redundant sigmoid colon, with an anastomosis performed in the mid-rectum. No rectopexy was performed. There were no anastomotic leaks and no significant complications. The functional result was good in all cases, with subjective improvement in constipation. Follow-up was 6 months, with no recurrences of rectal prolapse (13).
Another approach in Germany, by Rudroff C et al., was presented for a female 86-year-old with obstructive defecation syndrome and pelvic organ prolapse; they performed laparoscopic resection rectopexy (RRP) combined with mesh sacrocolpopexy (SCP) (14), a technique similar to this case.
Conclusions
This case illustrates the complexities of managing functional constipation, redundant sigmoid colon, and rectal prolapse in young adults. The combination of these conditions complicates treatment, prolonging symptoms and reducing quality of life. The patient, an 18-year-old male with a history of constipation and abdominal pain, presented with both a redundant sigmoid colon and irreversible rectal prolapse. After thorough assessment, he underwent laparoscopic resection and mesh rectopexy, which effectively addressed the underlying issues, relieved symptoms, and improved gastrointestinal function.
Managing such complex cases requires a multi-disciplinary approach, combining conservative and surgical treatments. Non-invasive measures like dietary adjustments and laxatives are crucial for constipation management, but surgery is necessary when complications worsen symptoms. The success of the laparoscopic method in this case emphasizes timely intervention's role in preventing long-term complications and enhancing quality of life. Future studies and additional case reports will be vital in refining
treatment strategies and understanding how to manage these challenging conditions in young adults.
Conflict of Interest
All author declare that they have no conflict of interest.
Funding
No funding sources.
References
1. Nayak SB, Pamidi N, Shetty S, Sirasanagandla S, Ravindra S, Guru A, et al. Displaced sigmoid and descending colons: a case report. OA Case Reports. 2013;2(17):166.
2. Zarokosta M, Piperos T, Zoulamoglou M, Theodoropoulos P, Nikou E, Flessas I, et al. Anomalous course of the sigmoid colon and the mesosigmoid encountered during colectomy. A case report of a redundant loop of sigmoid colon. Int J Surg Case Rep. 2018;46:20-23.
3. Bharata MBS, Bharata MDY, Jayaningrum IGAAB. Anomalies of the sigmoid colon during laparotomy exploration: a case report of a redundant colon in the sigmoid and transverse colon. Intisari Sains Medis. 2021;12(1):52-54.
4. Raahave D. Dolichocolon revisited: An inborn anatomic variant with redundancies causing constipation and volvulus. World J Gastrointest Surg. 2018;10(2):6-12.
5. Koppen IJ, Vriesman MH, Saps M, Rajindrajith S, Shi X, van Etten-Jamaludin FS, et al. Prevalence of functional defecation disorders in children: a systematic review and meta-analysis. J Pediatr. 2018; 198:121-130.e6.
6. Noviello C, Nobile S, Romano M, Mazzarini A, Papparella A, Cobellis G. Functional constipation or redundancy of the colon? Indian J Gastroenterol. 2020;39(2):147-152.
7. Allen P, Setya A, Lawrence VN. Pediatric functional constipation. StatPearls [internet]: StatPearls Publishing; 2024.
8. Diaz S, Bittar K, Mendez MD. Constipation. Psychol Issues. 2018; 17:18.
9. Forootan M, Bagheri N, Darvishi M. Chronic constipation: A review of literature. Medicine (Baltimore). 2018;97(20):e10631.
10. Rajindrajith S, Devanarayana NM, Benninga MA. Childhood constipation: Current status, challenges, and future perspectives. World J Clin Pediatr. 2022;11(5):385-404.
11. Raahave D. Dolichocolon revisited: An inborn anatomic variant with redundancies causing constipation and volvulus. World J Gastrointest Surg. 2018;10(2):6-12.
12. Zhang Y, Lin Q, An X, Tan X, Yang L. Factors Associated with Functional Constipation among Students of a Chinese University: A Cross-Sectional Study. Nutrients. 2022;14(21):4590.
13. Charalampopoulos A, Pikouli A, Latsonas P, Kirkilesis G, Bagias G, Papaconstantinou D, et al. Complete Rectal Prolapse Associated with Redundant Sigmoid Colon in Young Psychiatric Patients: Anterior Resection of the Rectosigmoid is a Safe and Effective Choice of Operation. Journal of Surgery and Research. 2023;6:260-263.
14. Rudroff C, Ludwig S. Laparoscopic resection rectopexy (RRP) combined with mesh sacrocolpopexy (SCP) for obstructed defecation syndrome with pelvic organ prolapse in an interdisciplinary approach. Facts Views Vis Obgyn. 2024;16(2):231-236.
Full Text Sources:
Abstract:
Views: 6087

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.