Surgery, Gastroenterology and Oncology

|
|
Background: Gallbladder cancer is a rare malignancy with an incidence of 1-2 cases per 100,000 people. Adenocarcinoma is the most common type, with gallbladder sarcomatoid carcinoma comprising 1% of the cases. Due to its rarity, less than 100 cases have been reported in the literature.
Case Presentation: We report the case of a healthy 76-year-old female that was submitted to elective laparoscopic cholecystectomy for a pre-operative diagnosis of cholelithiasis. One month after surgery, the patient presented anorexia, asthenia and fever and was admitted to the Emergency Department. CT scan revealed a neoplastic mass centered at the cholecystectomy site, a metastatic lesion in segment 4b, ascites and peritoneal carcinomatosis. Histological examination was compatible with the diagnosis of gallbladder sarcomatoid carcinoma. The patient died 14 days after admission.
Discussion/Conclusion: Preoperative diagnosis is challenging because of nonspecific clinical and radiological findings, making the definitive diagnosis dependent on pathological examination. Given the rarity of this tumor, its clinical behavior and optimal treatment are not well understood. While surgical resection is the primary treatment, the role of chemotherapy and radiation therapy remains poorly defined.
INTRODUCTION
Primary gallbladder cancer is a malignant tumor with an annual incidence of 1.2 cases per 100,000 individuals, representing 0.6% of all cancers globally. It tends to occur more frequently in older individuals, particularly women, with a female-to-male ratio ranging from 2:1 to 5:1, and an average age of 60-70 years. Gallbladder carcinoma is the fifth most common cancer of the gastrointestinal system and the leading malignancy of the biliary tract. Among these, it is the most aggressive, often showing the shortest median survival times (1-6).
Adenocarcinoma is the predominant type, constituting 98% of gallbladder cancers, while gallbladder sarcomatoid carcinoma is an exceptionally rare variant, making up less than 1% of such tumors (1-5). First described by Landsteiner in 1907 (1,2), fewer than 100 cases have been documented worldwide (6,7).
Sarcomatoid carcinoma is thought to originate from totipotent stromal stem cells and is composed of both epithelial and mesenchymal components, including undifferentiated spindle or stellate cells (1,2). While this type of tumor can occur in various organs, including the kidneys, lungs, and prostate, its occurrence in the gallbladder is exceedingly rare (5,8,9).
The exact cause of gallbladder sarcomatoid carcinoma remains unclear, but some studies suggest links to gallstones, gallbladder polyps, and estrogen levels (8).
Clinical manifestations of this carcinoma are similar to those of adenocarcinoma and may include abdominal pain, jaundice, nausea, anorexia, weight loss, and occasionally a palpable abdominal mass
(1-3,6). Due to its nonspecific symptoms, preoperative diagnosis is often difficult, and there is limited understanding of its clinical behavior, prognosis, and optimal treatment (4,7).
We report the case of a healthy 76-year-old female who, after undergoing elective laparoscopic cholecystectomy for suspected cholelithiasis, was diagnosed with gallbladder sarcomatoid carcinoma upon pathological examination.
CASE REPORT
A healthy 76-year-old female was assessed in Hepato-biliary consultation because of symptomatic cholelithiasis with an ultrasound showing a gallbladder with normal dimensions, with multiple gallstones in its lumen that do not exceed 2 cm and bile mud.
She was admitted to elective laparoscopic cholecystectomy 1,5 months after consultation. During surgery multiple adhesions of the epiploon and stomach to the gallbladder and a cholecystogastric fistula were observed. The fistula was resected with stapler. The gallbladder presented signs of chronic cholecystitis and was fused to the liver, making it impossible to excise the gallbladder without adjacent partial hepatectomy. The postoperative was uneventful and the patient was discharged on D1.
One month after surgery, just before the post-operative consultation, the patient presented anorexia, asthenia and fever and was admitted to the Emergency Department.
Laboratory analysis showed leukocytosis 12.88 × 109/L, CRP 169.6mg/L and normal liver function tests.
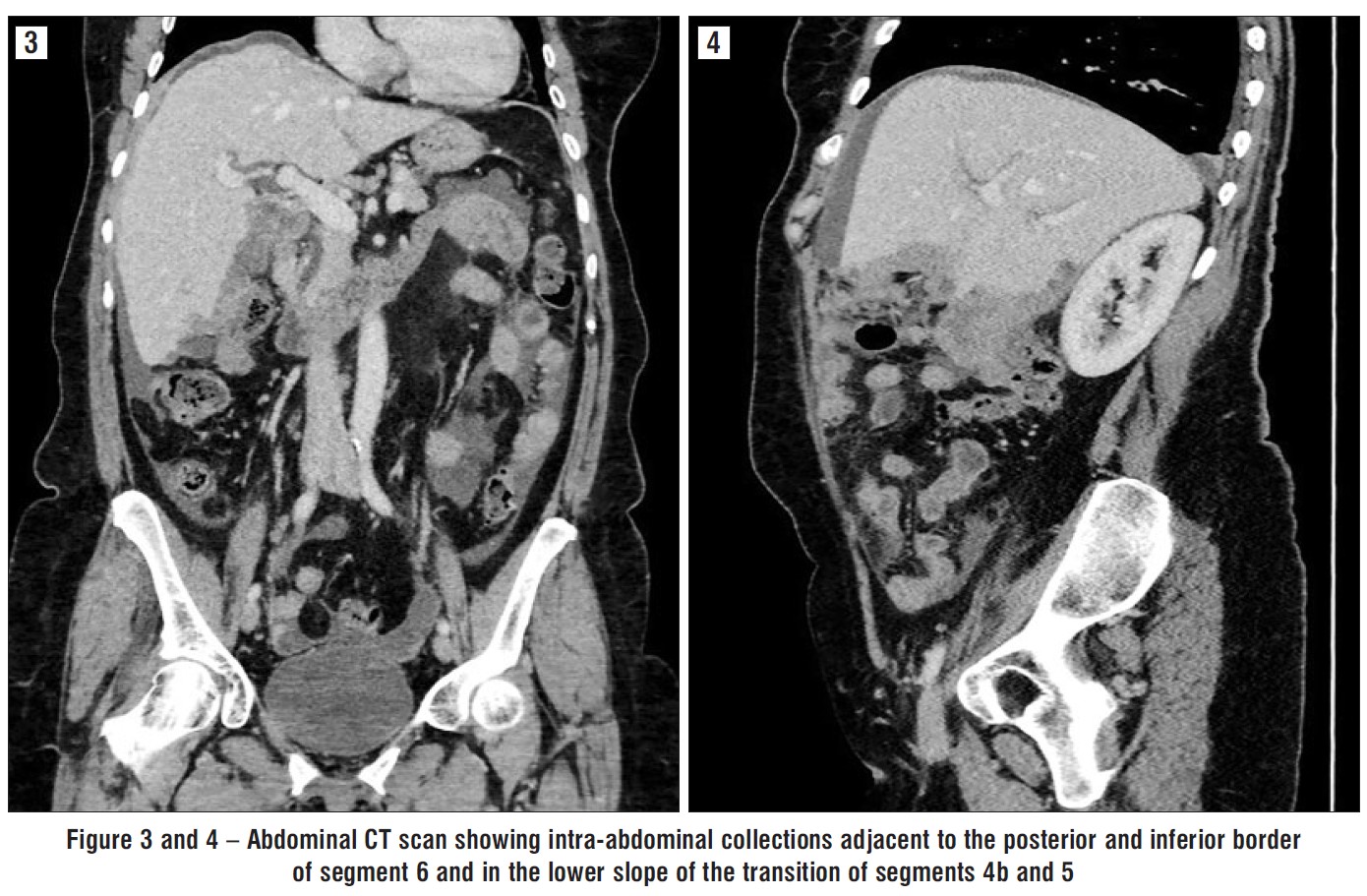
CT scan showed a neoplastic mass centered at the cholecystectomy site with infiltrative margins to segments 4b, 5 and 6, a nodular area in segment 4b, most likely to correspond to a metastatic lesion, intra-abdominal collections adjacent to the posterior and inferior border of segment 6, with 30x11 mm and in the lower slope of the transition of segments 4b and 5, with 12x10 mm, ascites and peritoneal carcinomatosis (figs. 1-4).
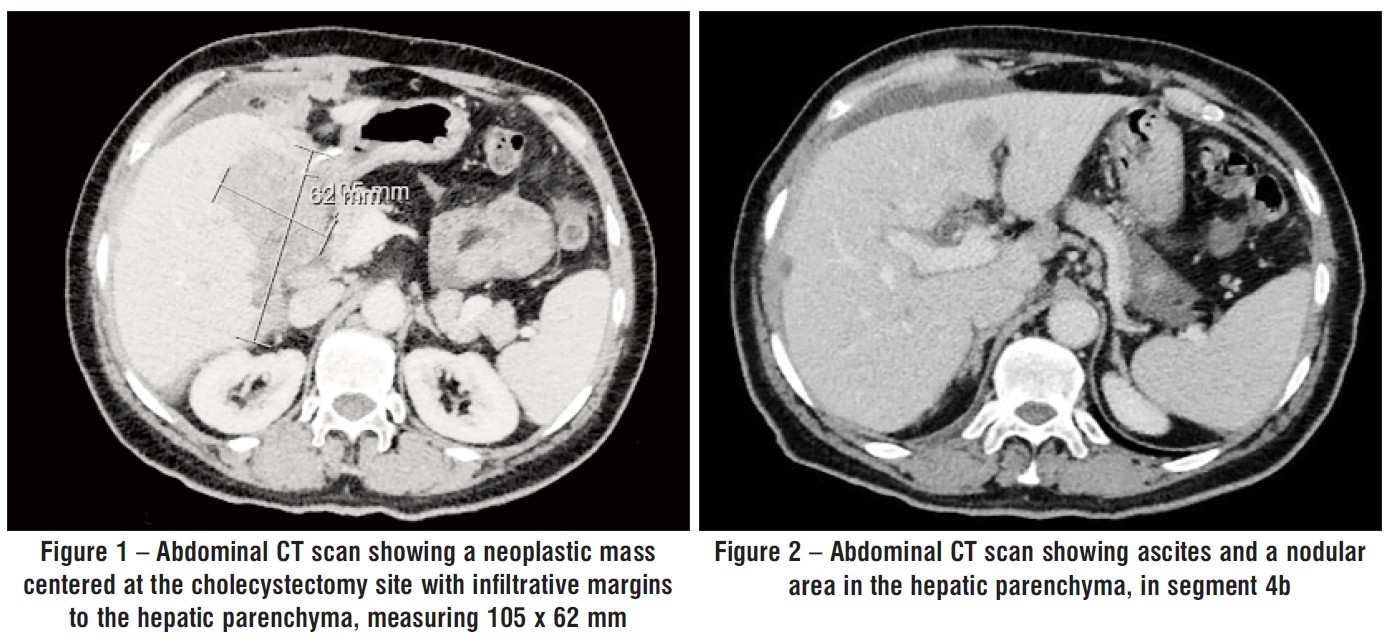
Figure 3 and 4 – Abdominal CT scan showing intra-abdominal collections adjacent to the posterior and inferior border of segment 6 and in the lower slope of the transition of segments 4b and 5
She was admitted to the Surgical Department.
Gross examination of the gallbladder revealed a protruding vegetant lesion within the lumen, measuring 2.9 × 2.5 × 1.5 cm (fig. 5 a, b), adjacent to an area showing signs of wall perforation. The majority of the mucosa was eroded, and several gallstones were identified. Histological examination revealed a solid neoplasm with areas of necrosis (fig. 6). The neoplasm consisted of epithelioid cells with pleomorphic nuclei, with a high mitotic index (>10/2 mm²), perineural invasion, and focal venous invasion. The remaining gallbladder mucosa displayed features of chronic cholecystitis with extensive erosion and low-grade biliary intraepithelial neoplasia, with high-grade foci.
Figure 5 – The gallbladder exhibits a vegetant neoplasm (a) within the lumen, with perforation of the wall (b)

Figure 6 – Histological examination exhibiting a neoplasia infiltrating the gallbladder wall (a: H&E; low power). Sarcomatoid carcinoma with epithelioid cell morphology and pleomorphic nuclei (b: H&E; 200x) exhibiting focal cytokeratin expression (d: CK8/18 100x). Dysplasia was identified in the adjacent mucosa (c: H&E; 100x)
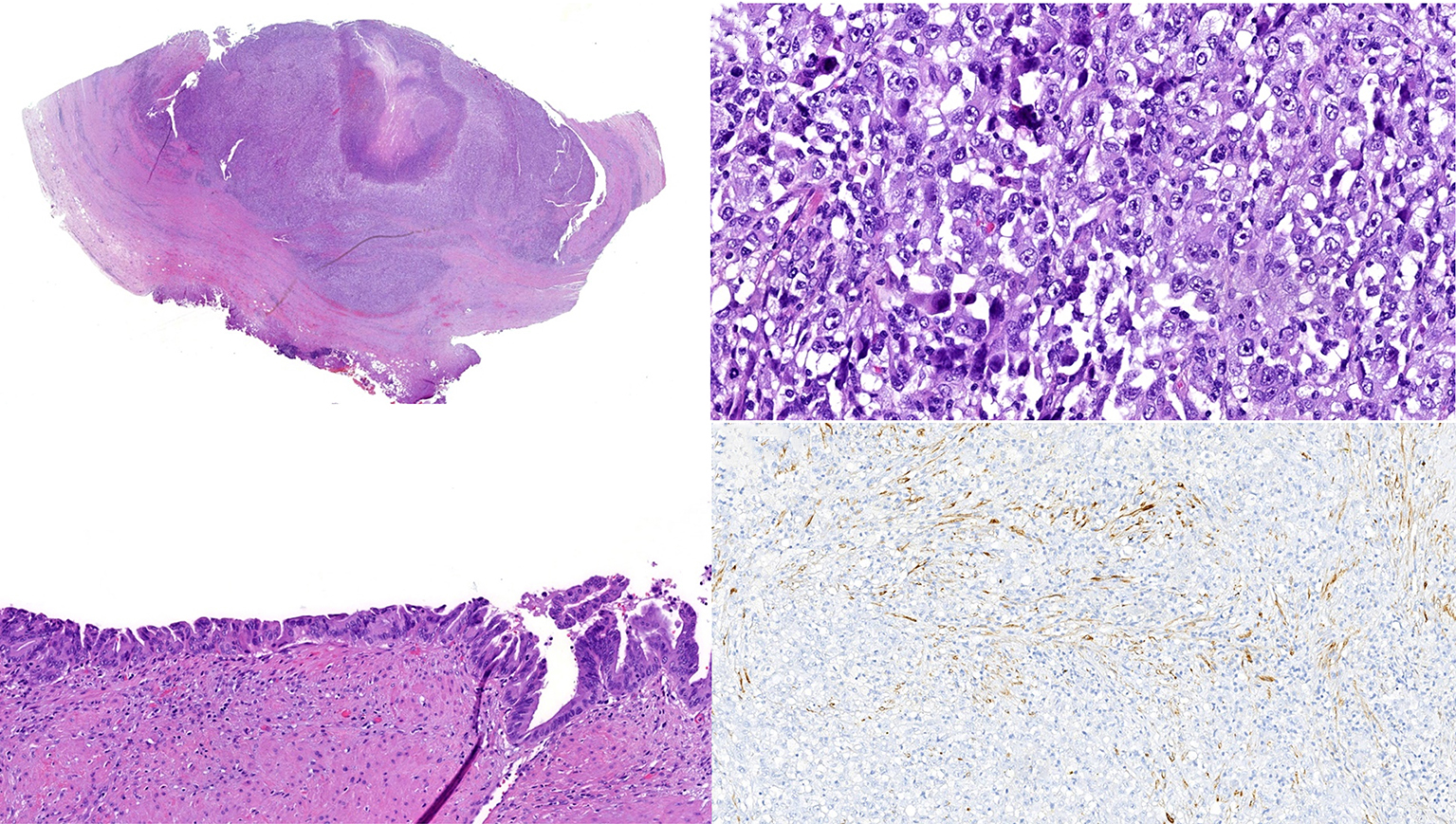
In the immunohistochemical study, the neoplastic cells exhibited diffuse expression of vimentin, with only focal expression of CK8/18, SMA, desmin, CD68, and SATB2. The remaining immunohistochemical markers were negative, including: Melan-A, S100 protein, SOX-10, HMB-45, ERG, CD34, CD30, CD23, CD21, CD20, CD3, CD45, AE1/AE3, EMA, and MyoD1. The p53 status was wild-type. This was compatible with the diagnosis of gallbladder sarcomatoid carcinoma.
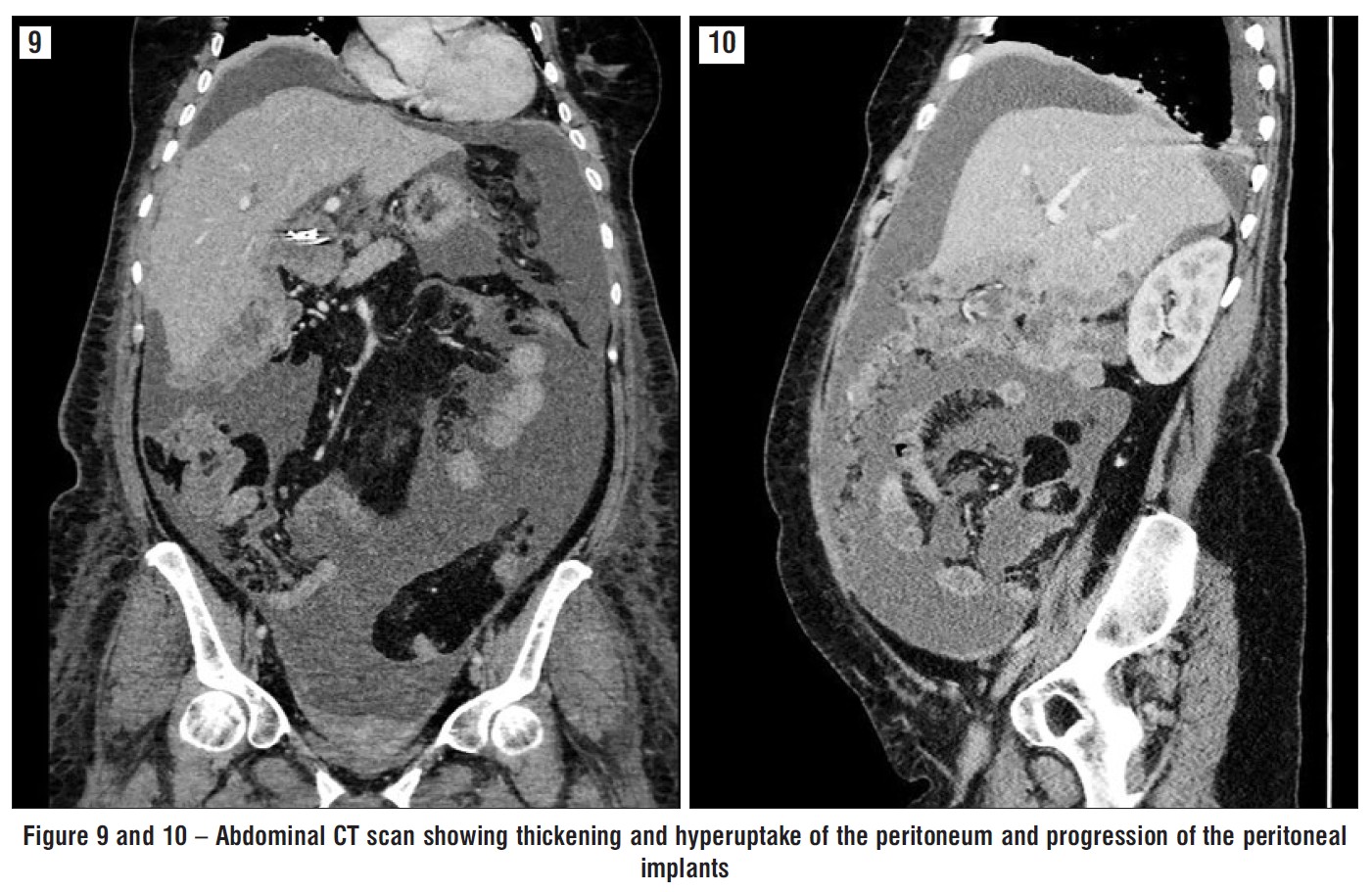
Since the patient presented aggravated inflammatory parameters under antibiotherapy a CT scan was repeated 7 days after that showed thickening and hyperuptake of the peritoneum, ascites with marked increase and progression of the peritoneal implants, compatible with peritonitis superimposed on peritoneal carcinomatosis (figs. 7-10).
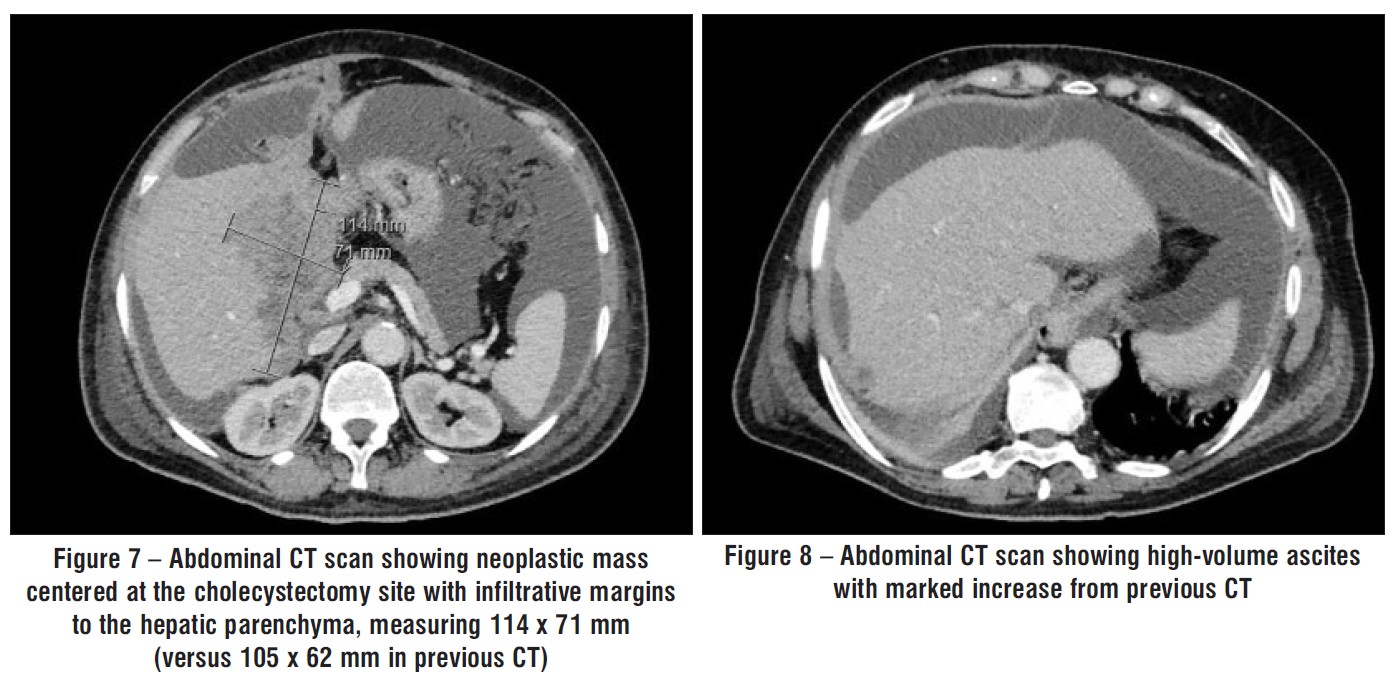
Figure 9 and 10 – Abdominal CT scan showing thickening and hyperuptake of the peritoneum and progression of the peritoneal implants
The case was discussed in the Hepatobiliary Tumor Board and was decided palliative care.
The patient died 14 days after admission.
DISCUSSION
Diagnosing gallbladder sarcomatoid carcinoma before surgery is challenging, primarily due to its nonspecific clinical signs, lack of distinct biomarkers, and unclear radiological presentation. In approximately 70% of cases, the disease is associated with gallstones (2,6,7). In the present case, the preoperative diagnosis was cholelithiasis, and the sarcomatoid carcinoma was only discovered after the gallbladder specimen was analysed.
Gallbladder cancers, including sarcomatoid carcinoma, are often asymptomatic in the early stages, which complicates timely diagnosis (5). Histo-pathological analysis is essential to confirm the diagnosis, revealing the characteristic malignant epithelial and mesenchymal (sarcomatous) tumor components (6,7).
Immunohistochemical staining or electron micro-scopy is required to identify the dual differentiation of the tumor. Sarcomatous cells in these tumors are typically undifferentiated spindle cells that express both cytokeratin and vimentin and show desmo-somal-like junctions and cytoplasmic intermediate filament aggregates, indicating an epithelial origin for the sarcomatous component (2,5,6,8).
Sarcomatoid carcinomas tend to be more aggressive than typical gallbladder adenocarcinomas. Their aggressive behavior is further supported by high p53 expression (60%) and a high proliferation index (median 40%) (10). These tumors usually progress rapidly, with a high propensity for systemic metastasis, even in early stages, and a high recurrence rate (1,6-9). In the case discussed, the patient experienced rapid disease progression, with metastatic lesions and peritoneal carcinomatosis appearing within a month of surgery, leading to death soon after. The median survival rate is generally very poor, with some studies reporting only 5.5 months, and metastasis to the liver, lymph nodes, and peritoneum are common (2,6).
A meta-analysis by Zhang et al. (11) found a mean survival of 17.5 months and a median survival of 5 months, with a 1-year survival rate of about 19%. In a separate study by Taskin et al., 656 gallbladder cancer cases were examined, 11 of which contained a sarcomatoid component. Of these, 84% presented with advanced-stage disease, and the median survival of those with sarcomatoid carcinoma was 8 months compared to 26 months for typical gallbladder carcinoma cases (10).
Surgical resection remains the primary treatment for sarcomatoid carcinoma, although there is no standardized approach. Radical cholecystectomy with lymph node dissection and liver resection, has been recommended, as patients who undergo radical surgery tend to have better overall survival. However, even with radical treatment, recurrence is common, and adjuvant therapy may be necessary. Unfortunately, evidence-based treatments for post-operative recurrence are lacking, and the role of chemotherapy and radiation therapy remains unclear. Chemoradiotherapy has been explored in earlier studies, but its effectiveness in improving patient outcomes remains limited (1,2,4,5,8,9).
A study conducted between 2018 and 2022 examined 2669 gallbladder carcinoma cases, identifying 14 cases of sarcomatoid carcinoma. Most patients (8 out of 14) presented with locally advanced or metastatic disease (5 out of 14). The chemotherapy regimens most commonly used were gemcitabine and cisplatin, with some patients also receiving external beam radiotherapy. Despite treatment, most patients died within a year of diagnosis (12). Another study by Qin et al. reported that all patients with advanced-stage sarcomatoid carcinoma died shortly after surgery, though one patient with stage IIIb disease who received adjuvant chemoradiotherapy (gemcitabine and capecitabine) experienced a progression-free survival of 12 months (4).
Currently, due to a lack of specific chemotherapy regimen for sarcomatoid carcinoma we follow the NCCN guidelines for gallbladder cancer, that recommend gemcitabine monotherapy or in combination with cisplatin or capecitabine, capecitabine monotherapy or in combination with cisplatin or oxaliplatin, and 5-fluorouracil (13).
However, recent research suggests that S-1 based chemotherapy (Tegafur, Gimeracil and Oteracil Potassium Capsules), may improve survival (9). Further exploration of targeted therapies and novel chemo-therapy options is essential for improving outcomes for patients with this rare and aggressive cancer (1).
Drugs such as entrectinib, larotrectinib, repotrectinib (NTRK fusion), pembrolizumab, dostarlimab-gxly, nivolumab plus ipilimumab (MSI-H or MMR deficiency), dabrafenib plus trametinib (BRAF V600E mutation), futibatinib, pemigatinib, erdafitinib (GFR2 fusion), ivosidenib (IDH1 mutation), trastuzumab, zanidatamab-hrii (HER2 overexpression), pralsetinib, selpercatinib and adagrasib (KRAS mutation, MET amplification, ALK, RET or ROS fusions) may benefit certain patients with advanced disease harboring specific genomic mutations (13).
Unfortunately, our patient was never able to receive therapy due to complications from the underlying disease process.
CONCLUSION
Gallbladder sarcomatoid carcinoma is a rare and highly aggressive malignancy. Preoperative diagnosis is difficult due to nonspecific clinical and radiological features, making histopathological examination critical for diagnosis. The rarity of this tumor has hindered a comprehensive understanding of its clinical behavior and treatment strategies. Although surgical resection remains the main treatment option, the role of chemotherapy and radiation therapy in improving outcomes is yet to be established. More research is needed to identify effective treatments for this aggressive form of cancer.
Author’s Contributions
Conceptualization: EC, RRD, MA. Data curation: EC, RRD, MA, CPC. Methodology: EC, RRD, MA. Visualization: EC, RRD, MA, CPC. Writing - original draft: EC, RRD. Writing - review & editing: MA, HC, LG, SC.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
REFERENCES
1. Kataria K, Yadav R, Seenu V. Sarcomatoid carcinoma of the gallbladder. J Surg Case Rep. 2012;2:5.
2. Yasmeen K, Kulkarni D, Patel R, Bankapur A. Sarcomatoid carcinoma of the gallbladder: A case report and review of the literature. Clinical Cancer Investigation Journal. 2015;4:274-276.
3. Liu KH, Yeh TS, Hwang TL, Jan YY, Chen MF. Surgical management of gallbladder sarcomatoid carcinoma. World J Gastroenterol. 2009; 15:1876-9.
4. Qin Q, Liu M, Wang X. Gallbladder sarcomatoid carcinoma: Seven case reports. World J Clin Cases. 2020;17:3881-3889.
5. Cho YH, Cha SW, Cho YD, Lee MY, Chu CW, Hong SS, Jin SY. Gallbladder Sarcomatoid Carcinoma Diagnosed after Surgery. The Korean Journal of Pancreas and Biliary Tract. 2023;2:38-42.
6. Siddiqui M, Hegde S, Nguyen T, DePaul S. Sarcomatoid carcinoma of the gallbladder: A rare form of gallbladder cancer. SAGE Open Med Case Rep. 2020;8:2050313X20906739.
7. Limaiem F, Bayar R, Omrani S. Sarcomatoid carcinoma of the gallbladder: A rare and aggressive form of gallbladder cancer. Clin Case Rep. 2023;1:e6876.
8. Shi Y, Chen J, Chen H, Hong X. Sarcomatoid carcinoma of the gallbladder: a case report. J Int Med Res. 2020;6:300060520935283.
9. Zou RQ, Hu HJ, Lv TR, Liu F, Ma WJ, Wang JK, et al. Clinico-pathological characteristics and outcome of primary sarcomatoid carcinoma of the gallbladder. Front Oncol. 2022;12:1009673.
10. Taskin OC, Akkas G, Memis B, Seven IE, Basturk O, Jang KT, et al. Sarcomatoid carcinomas of the gallbladder: clinicopathologic characteristics. Virchows Arch. 2019;1:59-66.
11. Zhang L, Chen Z, Fukuma M, Lee LY, Wu M. Prognostic significance of race and tumor size in carcinosarcoma of gallbladder: a meta-analysis of 68 cases. Int J Clin Exp Pathol. 2008;1(1):75-83.
12. Yadav S, Vaidya M, Kumar R, Deodhar K, Ramadwar M, Bal M. Sarcomatoid carcinoma of gallbladder: A series of 14 cases from a single tertiary-care oncology centre. Ann Oncol. 2022;33: S1480.
13. Al B. Benson AB, D’Angelica MI, Abrams T, Ahmed A, Akce M et al. Biliary Tract Cancers Version 2.2025, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Net: JNCCN. 2025.
Full Text Sources:
Abstract:
Views: 1185

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.