Surgery, Gastroenterology and Oncology

|
|
Ovarian cysts (OC) are common in young women, with different aetiology according to their developmental stage and hormonal development. Although rare, hypothyroidism has been associated with OC development. We present a case of a 16-year-old patient diagnosed with a painful OC one year after total thyroidectomy (TT) due to papillary carcinoma) and severely increased levels of TSH despite thyroid hormonal oral therapy. After a non-complicated laparoscopic cystectomy, a mucinous cystadenoma was diagnosed. In the next two years, with better controlled levels of TSH, no contralateral or OC recurrence occurred. To our knowledge this is the first report of an OC development after a TT in a teenager. As hypothyroidism can lead to OC development, thyroid function tests should be included in all girls evaluated for OC as a more efficient hormone therapy may lead to OC resolution without need of surgery.
INTRODUCTION
Ovarian cysts (OC) are common in teenagers, given their hormonal state of development (1). Although rare, hypothyroidism has been associated with development of OC in paediatric patients, either unilateral or bilateral, isolated or multiple (2-4).
While OC development has been described in some case reports of congenital and/or severe juvenile hypothyroidism (2-5), to our knowledge, there hasn’t been a report of unilateral ovarian cyst secondary to acquired hypothyroidism.
CASE REPORT
A 16-year-old girl (Weight = 100 Kg and Height = 1.73 m; BMI = 33.3 Kg/m2) was submitted to total thyroidectomy and radio ablative iodine therapy due to a thyroid papillary carcinoma with lung metastasis. She initiated thyroid hormonal reposition the day after surgery (0.125 mg/day) and presented with normal levels of thyroid function one month after surgery. At her 4-month post-op evaluation, she presented with TSH levels > 100000 Ul/mL that persisted for 6 months even with an increased dose of levothyroxine of 0.225 mg/day.
Figure 1 - Simple cyst originating from left ovary in abdominal ultrasound
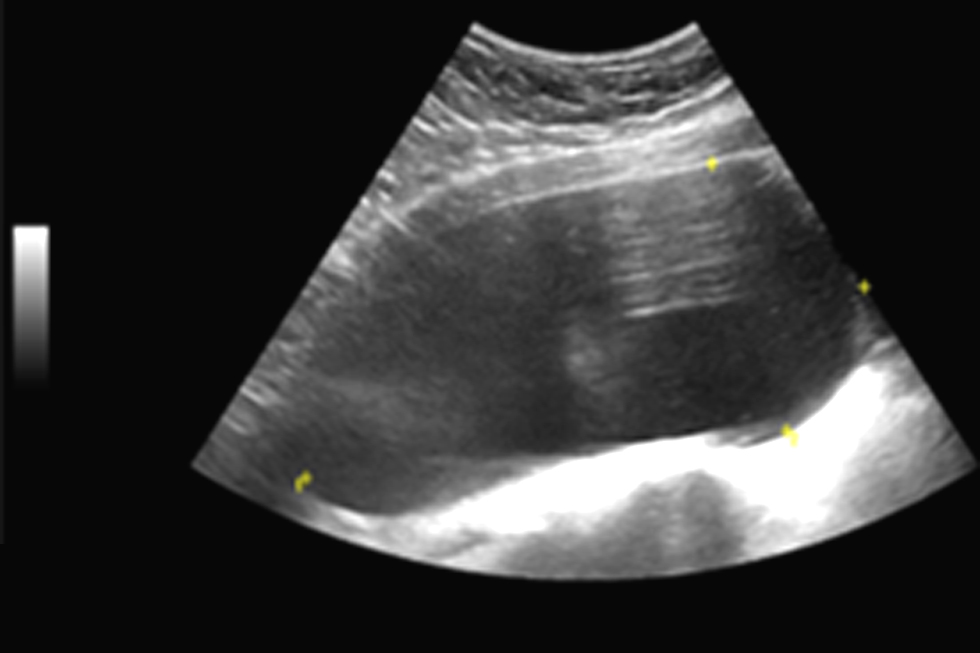
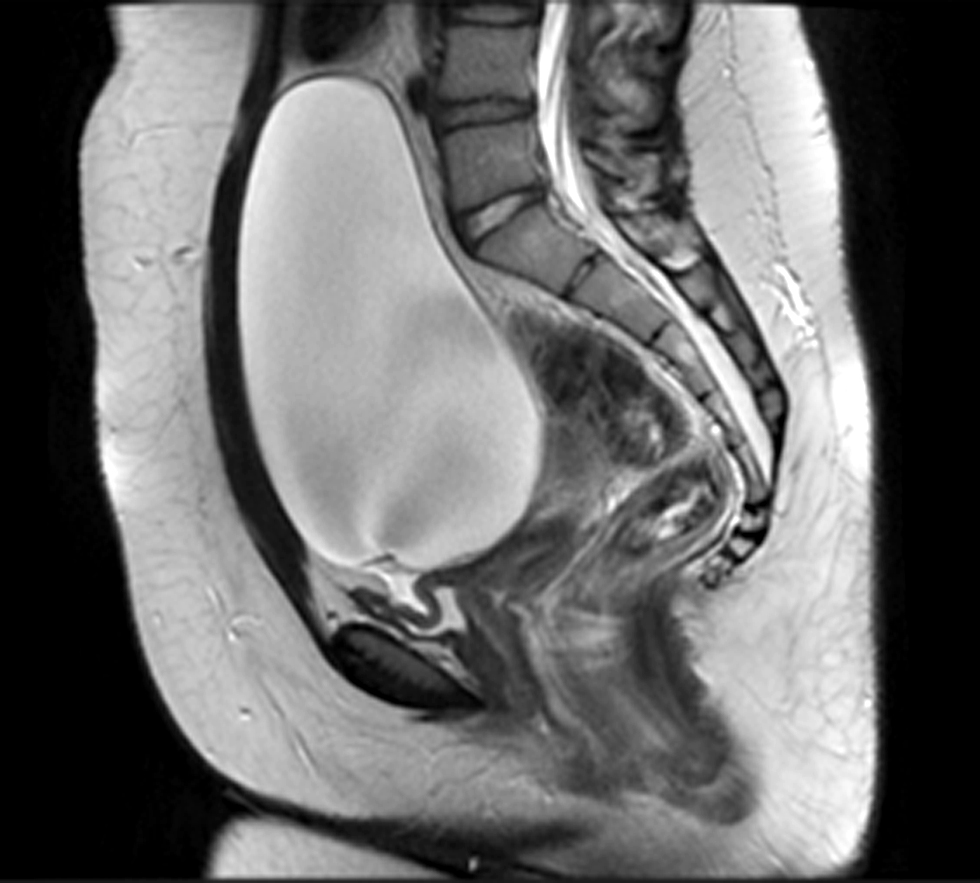
One year after total thyroidectomy, the patient complained of hypogastric discomfort and low vesical compliance, with increasing levels of urinary creatinine. Her TSH levels had increased again to >100000 UI/mL. A simple left ovarian cyst with 174 x 80 mm compressing the bladder was identified in abdominal-pelvic ultrasound (fig. 1). Magnetic resonance confirmed the presence of an OC (175 x 140 x 100 mm) in the left ovary and the absence of loco-regional aggressiveness findings (fig. 2). She had normal levels of FSH and LH, non-elevated testosterone or oestradiol levels and normal serum levels of beta-hCG, alpha-fetoprotein and CA-125. The patient had no previous history of menstrual cycle irregularities and no OC had been identified in previous imagiological abdominal exams.
Figure 2 – A simple, well delimited ovarian cyst, measuring 175 x 80 mm, compressing the bladder, with no locoregional criteria of malignancy
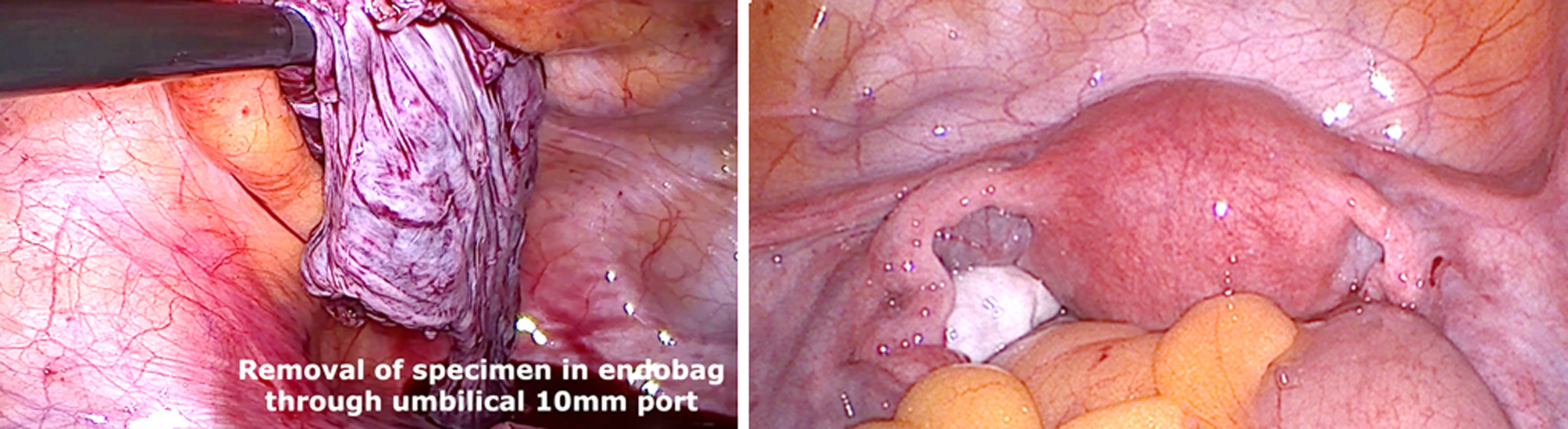
Because of the recurrent pain and lower urinary obstruction secondary to the OC, she was submitted to laparoscopic cystectomy. An OC occupying the pelvis and lower abdominal region was identified (fig. 3). Inspection of coelomic cavity was performed, and peritoneal, mesenteric, and liver metastasis were excluded. Using a Veress Needle, cyst decompression was performed, and 2L of serous liquid were aspirated. The right ovary showed no macroscopic changes. A cystectomy was performed using ultrasonic coagulation and blunt dissection (figs. 4, 5) and the specimen was removed using an Endobag. The patient was discharged 2 days after surgery and there were no postoperative complications. Histology confirmed a benign ovarian mucinous cystadenoma. Two-years after the TT, under oral thyroid replacement therapy adjustment and better control of her TSH levels, there was no OC recurrence.
Figure 3 – Ovarian Cyst occupying the pelvis and lower abdominal region (a) and aspiration of 2 litters of serous liquid from the ovarian cyst (b)
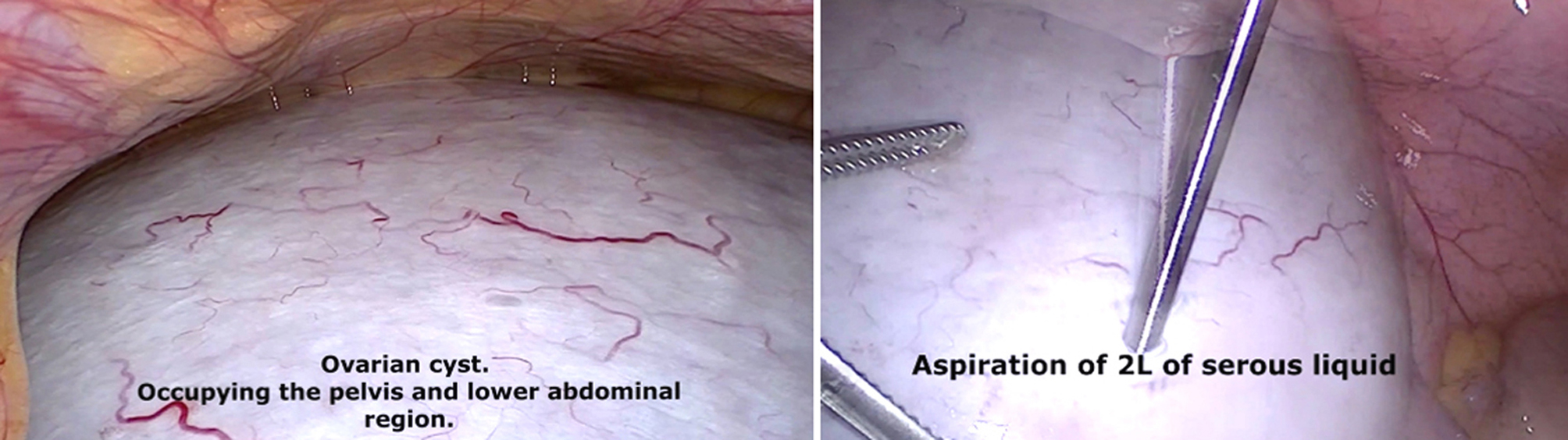
Figure 4 - Laparoscopic cystectomy using ultrasonic coagulation (a) and blunt dissection (b)
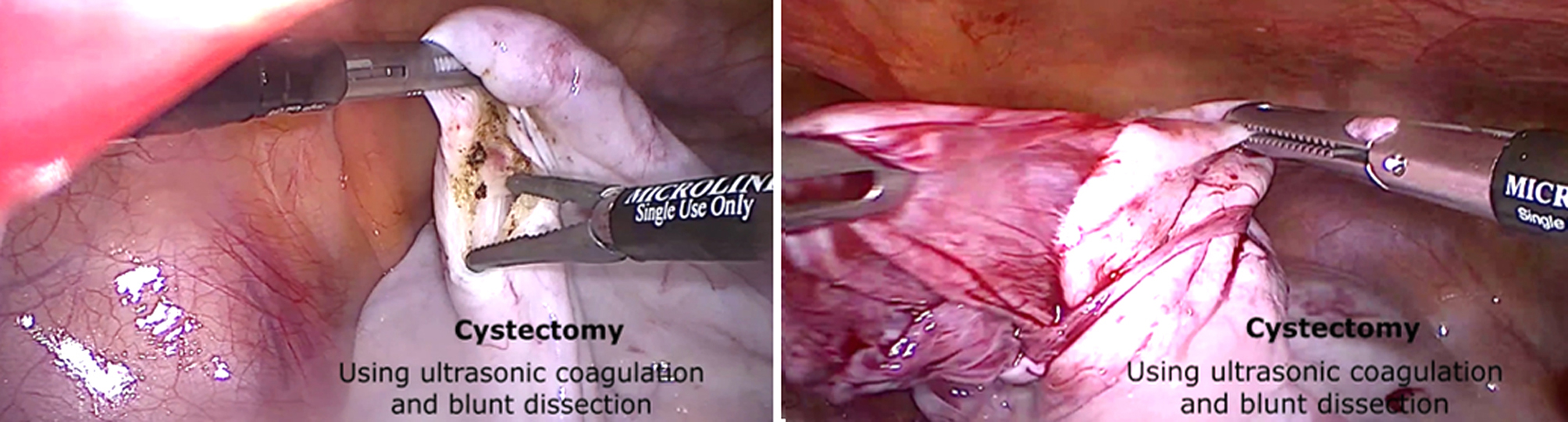
Figure 5 – Ovarian Cyst (a) and final celomic inspection (b) after cyst removal with preservation of the left ovary
DISCUSSION
Ovarian cysts occur frequently in teenage patients given their particular stage of hormonal development (1). At this age, most OC are asymptomatic and incidentally diagnosed in an ultrasound performed by other reason, and they usually correspond to functional cysts that tend to spontaneously regress (1). As so, a “watch and wait” approach is the most frequent treatment applied, but when these cysts become symptomatic or have a diameter superior to 5 to 6 cm, paediatric surgeons are faced with a dilemma between observation or active treatment (1,6). Even though ovarian malignancies only account for 1% of all the paediatric cancers (6), all patients with persistent and large OC require evaluation to exclude malignancy. Ultrasound and/or MRN evaluation and exclusion of malignant criteria images (namely, < 10 cm in diameter, papillary projections or thick septations, solid component, irregular borders increased blood flow)(1,7) and blood tumour markers (B-hCG, alfa-fetoprotein, CA 125, and oestradiol)(8,9) are essential to help the surgeon decide the adequate approach to these tumours. In the presented case, despite a size >10 cm, no other imaging findings suggested a malignant aetiology and all tumour markers were negative, pointing to a probable benign OC.
Because of the patient's previous TT and need of thyroid hormone replacement therapy, her TSH, T3 and T4 levels were periodically evaluated. An elevation of TSH levels > 100000 UI/mL was detected 4 months after TT, and those persisted almost for one year despite increasing levels of levothyroxine. One year after TT the symptoms of abdominal pain and urinary discomfort prompted the identification of the OC.
There is a growing awareness that longstanding and severe hypothyroidism can cause OC, ovarian hyperstimulation syndrome and sexual precocity (2-5,10). Some cases of OC in juvenile hypothyroidism and rarer thyroid conditions associated with reduced bone age and isosexual precocious puberty (the Van Wyk and Grumbach syndrome)(11) have also been described in teenagers. To our knowledge, this is the first case of an OC secondary to an acquired hypothyroidism (after TT).
Despite unknowing the exact etiological mechanism, there are several theories regarding OC formation in severe hypothyroidism (usually with TSH levels > 100000 U/mL) (12). On one hand, some authors postulate that sine TSH, FSH, LH and GH are all glycoproteins with common alpha chain, TSH may cross react with the gonadotropin receptors directly activating these gonadotropin receptors or sensitizing ovaries to gonadotropin stimulation. As a consequence of this gonadotropin stimulation, nuclear thyroid receptors in the granulosa cells are activated leading to ovarian hyperstimulation. On the other hand, TSH high levels can lead to a myxomatous type of ovarian infiltration can also interfere with steroidogenesis leading to cyst formation (10,12).
Although thyroid hormone reposition therapy frequently leads to regression of the OC (13), preventing an unnecessary surgery, in this case, the absence of response to hormonal reposition therapy and the patient’s symptoms prompted a surgical approach. Given the preoperative suspicion of a benign ovarian mass, an ovarian preserving laparoscopic approach was decided and the patient was discharged two days after surgery. Two years after surgery, no recurrence of an OC was detected in the follow-up, which, in line with other studies (14,15), suggests that cyst decompression and an ovarian sparing surgery are both good options when dealing with OC or ovarian masses suspected to be benign in the pre-operative study.
CONCLUSION
Despite unknown etiological mechanism, there is a growing awareness of longstanding and severe hypothyroidism as a cause of ovarian cysts development, ovarian hyperstimulation syndrome and sexual precocity. Some cases of OC development in juvenile hypothyroidism and other rarer thyroid conditions have been described. To our knowledge, this is the first case of an ovarian cyst development secondary to an acquired hypothyroidism (after total thyroidectomy). Although in the other cases thyroid hormone reposition generally leads to regression of ovarian cysts, in this case the absence of response to hormonal reposition, the symptoms and the preoperative suspicion of a benign ovarian mass in the complementary exams, led to an ovarian preserving laparoscopic approach for OC treatment.
Conflict of interest and source of funding
All authors declare no sources of funding received for the research and no conflicts of interest.
Ethical approval
For this case, ethical approval was obtained.
Author’s contributions
All authors had been actively involved in the reported case and took full responsibility for the content of this article.
REFERENCES
- Brandt ML, Helmrath MA. Ovarian cysts in infants and children. Semin Pediatr Surg. 2005;14(2):78-85.
- Xie Z, Li L, Liu W, Liu S, Luo J, Liao E. Successful treatment of a giant ovarian cyst by levothyroxin in a young adult woman: A case report. J Obstet Gynaecol Res. 2018;44(11):2115-8.
- Krishnamurthy S, Seth A, Puri A, Anand R, Aneja S. Ovarian tumors with elevated CA-125 levels and severe juvenile hypothyroidism: a need for increased awareness. Indian J Pediatr. 2010;77(6):693-4.
- Panico A, Lupoli GA, Fonderico F, Colarusso S, Marciello F, Poggiano MR, et al. Multiple ovarian cysts in a young girl with severe hypothyroidism. Thyroid. 2007;17(12):1289-93.
- Dharmshaktu P, Kutiyal A, Dhanwal D. Vanishing large ovarian cyst with thyroxine therapy. Endocrinol Diabetes Metab Case Rep. 2013;2013:130050.
- Tessiatore P, Guana R, Mussa A, Lonati L, Sberveglieri M, Ferrero L, et al. When to operate on ovarian cysts in children? J Pediatr Endocrinol Metab. 2012;25(5-6):427-33.
- Templeman CL, Fallat ME. Benign ovarian masses. Semin Pediatr Surg. 2005;14(2):93-9.
- Lawrence AE, Fallat ME, Hewitt G, Hertweck P, Onwuka A, Afrazi A, et al. Understanding the Value of Tumor Markers in Pediatric Ovarian Neoplasms. J Pediatr Surg. 2020;55(1):122-5.
- Papic JC, Finnell SM, Slaven JE, Billmire DF, Rescorla FJ, Leys CM. Predictors of ovarian malignancy in children: overcoming clinical barriers of ovarian preservation. J Pediatr Surg. 2014;49(1):144-7; discussion 7-8.
- Tresa A, Rema P, Suchetha S, Dinesh D, Sivaranjith J, Nath AG. Hypothyroidism Presenting as Ovarian Cysts-a Case Series. Indian J Surg Oncol. 2021;12(Suppl 2):343-7.
- Chattopadhyay A, Kumar V, Marulaiah M. Polycystic ovaries, precocious puberty and acquired hypothyroidism: The Van Wyk and Grumbach syndrome. J Pediatr Surg. 2003;38(9):1390-2.
- Shu J, Xing L, Zhang L, Fang S, Huang H. Ignored adult primary hypothyroidism presenting chiefly with persistent ovarian cysts: a need for increased awareness. Reprod Biol Endocrinol. 2011;9:119.
- Sharma Y, Bajpai A, Mittal S, Kabra M, Menon PS. Ovarian cysts in young girls with hypothyroidism: follow-up and effect of treatment. J Pediatr Endocrinol Metab. 2006;19(7):895-900.
- Braungart S, Craigie RJ, Losty PD. Controversies in the management of ovarian tumours in prepubertal children - A BAPS and UK CCLG Surgeons Cancer Group National Survey. J Pediatr Surg. 2018;53(11):2231-4.
- Renaud EJ, Somme S, Islam S, Cameron DB, Gates RL, Williams RF, et al. Ovarian masses in the child and adolescent: An American Pediatric Surgical Association Outcomes and Evidence-Based Practice Committee systematic review. J Pediatr Surg. 2019;54(3):369-77.
Full Text Sources:
Abstract:
Views: 3783

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.