Surgery, Gastroenterology and Oncology

|
|
Background: The cases classified as Bethesda III - Atypia of Undetermined Significance (AUS)/Follicular Lesion of Undetermined Significance (FLUS) are seen as a “gray zone” in thyroid cytopathology. Many previous studies have shown a wide variation in malignancy rates of Bethesda III thyroid nodules in different regions and institutions across the world. Objective: We want to describe the differential malignancy rates of FNACs diagnosed as Bethesda III based on cytological sub-classification and to assess the significance of demographic and ultrasonographic features in predicting malignancy in this category.
Material and Methods: A retrospective review was performed on all patients with thyroid nodules proven Bethesda category III who presented to our department from 01/2020 to 12/2021. We further classified these thyroid nodules into subgroup of Bethesda III, including AUS (cytologic atypia, cytologic and architectural atypia, Hürthle cell aspirates) and FLUS.
Results: In this study, there were 107 patients with 109 thyroid nodules that underwent surgery. Risk of malignancy (ROM) of Bethesda III thyroid nodules is 26.6%. An ACR – TIRADS score greater than or equal to 6 points had a predictive value for postoperative malignancy of Bethesda III thyroid nodules with sensitivity of 72.4% and specificity of 92.5%. The malignancy rate for nodules that featured cytologic atypia was significantly higher at 52.3% than the rate for nodules that had others atypia (p <0.001). Specifically, ROM of thyroid nodules with ACR – TIRADS score greater than or equal to 6 points and “focal cytologic atypia” – a subgroup of “cytology atypia” group – were up to 100%.
Conclusions: Bethesda III thyroid nodules with focal cytologic atypia and ACR – TIRADS score greater than or equal to 6 points were at high risk of malignancy. Those patients should undergo diagnostic surgical excision for definitive diagnosis and treatment.
INTRODUCTION
Thyroid FNA report is based on the Bethesda System for Reporting Thyroid Cytopathology 2017 (TBSRTC), a six-tier classification framework for diagnosing thyroid nodules (1). TBSRTC helps improve the quality of FNA cytology (FNAC) reporting, then reducing ambiguous diagnoses and decreasing surgery rates for benign lesions. Despite the benefits of FNAC and the Bethesda system, limitations still exist, the most significant of which are cases that fall into the “atypical” category—termed Bethesda III, including “atypia of undetermined significance (AUS)” or “follicular lesion of undetermined significance (FLUS)”. The malignancy rates for this category vary widely among institutions, ranging from 10% to 40% (2-5). Management of this category changes through different guidelines (6,7), depends on many factors such as clinical features, ultrasonographic patterns, and also cytological sub-classifications (8,9).
Therefore, the objective of this study was to assess the malignancy rate of thyroid nodules which were categorized as Bethesda III, including the significance of ultrasonographic and cytologic features. We especially aimed to determine malignant outcomes of each atypia subgroup of Bethesda III thyroid nodules.
MATERIAL AND METHODS
This was a retrospective study carried out in Ho Chi Minh Oncology Hospital from January 2020 to December 2021. Our study was approved by Ethics Committee On Biomedical Research (Number 374A/ BVUB-H???).
All patients had ultrasound results based on ACR – TIRADS 2017 grading system. Preoperative ultrasonographic features were recorded. Then we collected the FNA results which were sub-classified Bethesda III – AUS as Cytologic atypia (including focal cytologic atypia, extensive but mild cytologic atypia and atypical cyst-lining cells), Cytologic and architectural atypia and Hürthle cell aspirate. We also collected patients’ demographics, surgical method and final histopathology results.
The malignancy rate was calculated for nodules which underwent surgery. The malignant risk was evaluated in each subgroup of Bethesda III. Descriptive statistics were represented in tables.
Statistical Analysis
Statistical analysis was performed using SPSS version 25 (IBM Corporation, Armonk, NY). Ordinate demographic and ultrasonographic variables were assessed for significance using chi-square analysis. Continuous variables were evaluated using t-tests with the level of significance set at p <0.05.
RESULTS
We identified 107 patients with 109 thyroid nodules that met our criteria. Of these patients, 20 (18.7%) were men and 87 (81.3%) were women. The mean age was 41.72 ± 1.226. By reviewing the ultrasonographic features of the thyroid nodules and their corresponding pathology results, we identified which features were more likely to be associated with malignancy. Table 1 below lists the specific ultrasound features and the pathology results following excision. Certain features, such as irregular margins and microcalcifications were significantly associated with malignancy, while hypo-echogenicity was significantly associated with benign pathology.
Table 2 - Malignancy rate of thyroid nodule associated with ACR – TIRADS result
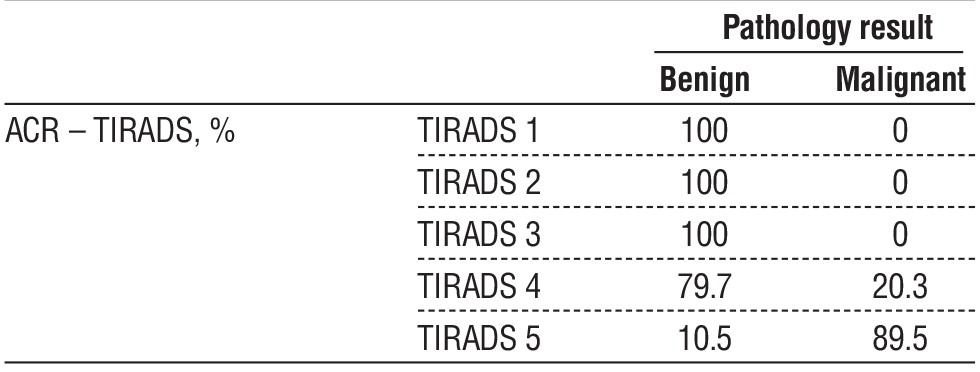
We also compared the ACR-TIRADS Scoring of the thyroid nodules with the pathology findings following biopsy. We found that TIRADS 1 through 3 were 100% benign. TIRADS 4 had a malignancy rate of 20.3%, while TIRADS 5 had a malignancy rate of 89.5% (table 2). To understand the importance of cytological subgroups, we compared the cytologic features with the pathology results. The group cytologic atypia was associated with a malignancy rate of 52.3% Specifically, the focal cytologic atypia feature (a subgroup of cytologic atypia) was highly associated with malignancy (68.4%) compared to other cytologic features (table 3).
To better understand the correlation among TIRADS Score, cytological subgroups, and malignancy rate, we stratified the data AUS subgroups by TIRADS Scores with a cut-off of 6 (fig. 1). We found the combination of TIRADS score of >6 points and focal cytological atypia resulted in a malignancy rate of 100% (table 4).

Figure 1 - ROC curve of ACR – TIRADS score predicts malignant thyroid nodules.

DISCUSSION
Bethesda III is a heterogeneous category with differing rates of malignancy across different institutions (10). The standard management of these patients is ill-defined with many options, including observation with ultrasound, repeat FNA, molecular studies, core biopsy thyroid nodule or thyroidectomy (6,7).
Ultrasound is a highly sensitive method for the detection of thyroid nodules and can be used to determine the morphological features of the nodule, nodal involvement and the need for FNA. Some ultrasound factors suggest suspicion of malignancy, such as hypoechoic, irregular margin, microcalcification, taller-than-wide shape, and extrathyroidal invasion. Although no single factor is sufficiently reliable to suspect malignancy, the combination of these factors increases diagnostic accuracy. In our study, irregular margin was an independent prognostic factor, with p < 0.001. This is similar to the studies of Chng and Maia, when they demonstrated that irregular margin was the strongest prognostic factor, with a positive predictive value of up to 100% (11,12). The ACR – TIRADS result is closely correlated with the risk of postoperative malignancy. The higher the ACR – TIRADS score, the higher the risk of malignancy, and up to 100% when all 5 factors suspicious for malignancy were present, according to author Chng (11). Our study found the same conclusion of ACR – TIRADS score, and the cut-off value according was 6 points, with AUC = 0.895.
One crucial reason for the wide range of malignancy rate in Bethesda III is the cytological subclassification. According to Elomami, 80% of confirmed malignancy cases demonstrated features of cytologic atypia (13). A meta-analysis of Soon-Hyun Ahn, 2017 (8) showed that the risk of malignancy in the cytologic atypia group was higher than all other subgroups, up to 44.5%, compared with 19.5% in microfollicular pattern subgroup, 15.1% in Hürthle cell pattern subgroup and 23% in other pattern subgroup. In our study, ROM of cytologic atypia subgroup was 52.3% (table 3), significantly higher than other subgroups. This result was similar to other studies which showed ROM of nuclear atypia subtype was over 40%, while ROM of other atypias were approximately 15 – 20% (9,14,15). This finding seems to be because of the similarities in nuclear atypia between Bethesda III – AUS group and Bethesda V – which has a higher ROM. Both classifications have some atypias such as mild nuclear enlargement, irregular nuclear contours, etc (1).
Therefore, the distinction between these two categories could be challenging (16). In contrast, other subgroups of Bethesda III like architectural atypia, Hürthle cell aspirates or FLUS, they share some same features with benign lesions which have a lower ROM, such as nodular goiter, hyperplastic changes, follicular neoplasm or Hurthle cell neoplasm (1).
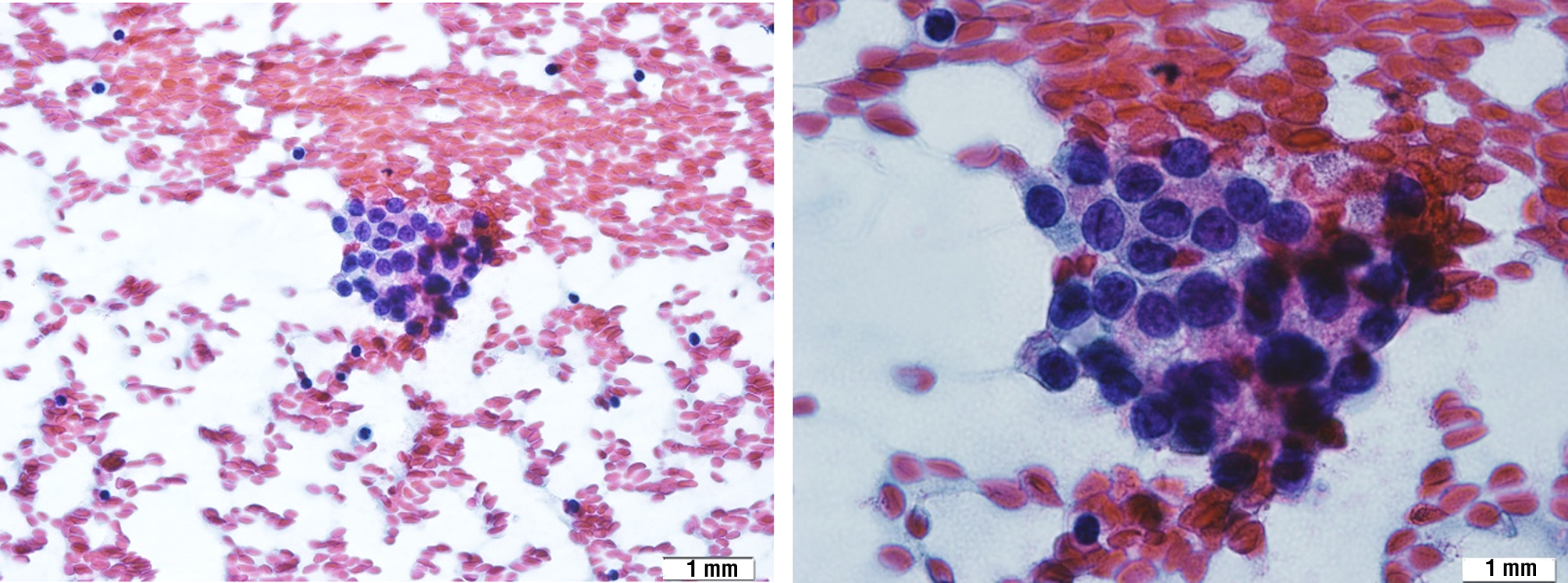
Remarkably, in the latest update of TBSRTC in 2023 (17), the term “follicular lesion of undetermined significance – FLUS” was discontinued to avoid confusion with reporting terminology and management. The authors believed that AUS was made the most confusion whether malignant or benign, so only the term “AUS” was kept in TBSRTC 2023. The author also highlighted that the recent subclassification of AUS focuses on differentiating nuclear atypia, which is associated with a comparatively higher risk, from other AUS morphologic patterns that indicate a lower risk. This approach aims to enhance communication between cytopathologists and the clinical team responsible for managing the patient, especially regarding the risk of malignancy.(17). Our study highly supported that viewpoint, as we found the malignancy rate of FLUS was only 11.4%, which did not cause any concern. In addition to that finding, cytologic atypia (fig. 2) had a significantly higher malignancy rate than other atypias (52.3% vs 5.6%).
Figure 2 - Focal cytologic atypia (37-year-old female). A. Papanicolaou, x40 ; B. Papanicolaou, x100
Furthermore, our study supports the reported idea that the more suspicious ultrasound patterns, combined with subclassification of nuclear atypia, the more malignant risk of thyroid nodule. Eisa reported that on multivariable analysis, both ATA high – risk ultrasonographic patterns and nuclear atypia were independently associated with an increased ROM (9). Lee et al. showed that nodules with nuclear atypia and ATA high-risk ultrasound features were more likely to be malignant (18). Similarly, Rosario et al. found that malignant rate when cytological subcategory and ultrasound were combined was 87% (19). Our study showed that this number, when combining cytologic subclassification of cytologic atypia and ACR – TIRADS score greater than or equal to 6 points, was up to 100%. Therefore, it is important to assert that patients with cytologic atypia, especially focal cytologic atypia, in combination with TIRADS 5 in ultrasound features are at increased risk of thyroid malignancy.
CONCLUSION
Bethesda III thyroid nodules with focal cytologic atypia and ACR – TIRADS score greater than or equal to 6 points were at high risk of malignancy. Thereupon, we suggest that those cases should be lobectomy or total thyroidectomy.
Conflict of interest
All author declare that they have no conflict of interest.
Financial Disclosure Statement
Dr. Nguyen has nothing to disclose. No funding was received for this article.
Ethical Statement
This research was approved by the Ethics Committee On Biomedical Research (No 374A/ BVUB-H??? 23nd December 2021). Complete written informed consent was obtained from the patient for the publication of this study and accompanying images.
REFERENCE
-
Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid.2017;27(11):1341-1346.
-
Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L, Baloch ZW. The Bethesda System for Reporting Thyroid Cytopathology: a meta-analysis. Acta Cytol. 2012;56(4):333-9.
-
Godoi Cavalheiro B, Kober Nogueira Leite A, Luongo de Matos L, Palermo Miazaki A, Ientile JM, Kulcsar MAV, et al. Malignancy Rates in Thyroid Nodules Classified as Bethesda Categories III and IV: Retrospective Data from a Tertiary Center. Int J Endocrinol Metab. 2017;16(1):e12871.
-
Sheffield BS, Masoudi H, Walker B, Wiseman SM. Preoperative diagnosis of thyroid nodules using the Bethesda System for Reporting Thyroid Cytopathology: a comprehensive review and meta-analysis. Expert Rev Endocrinol Metab. 2014;9(2):97-110.
-
Straccia P, Rossi ED, Bizzarro T, Brunelli C, Cianfrini F, Domenico Damiani 1, et al. A meta-analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated?. Cancer Cytopathol. 2015;123(12):713-22.
-
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133.
-
National Comprehensive Cancer Network. Thyroid carcinoma (version 1.2021). Retrieved from https://www.nccn.org/professionals/-physician_gls/pdf/thyroid.pdf.
-
Ahn SH, Kim SD, Jeong WJ. Comparison of risk of malignancy in a subgroup with atypia of undetermined significance/follicular lesion of undetermined significance: A meta-analysis. Head Neck. 2017; 39(8):1699-1710.
-
Eisa N, Khan A, Akhter M, Fensterwald M, Saleem S, Fananapazir G, et al. Both Ultrasound Features and Nuclear Atypia are Associated with Malignancy in Thyroid Nodules with Atypia of Undetermined Significance. Ann Surg Oncol. 2018;25(13):3913-3918.
-
Kholová I, Ludvíková M. Thyroid atypia of undetermined significance or follicular lesion of undetermined significance: an indispensable Bethesda 2010 diagnostic category or waste garbage? Acta Cytol. 2014;58(4):319-29.
-
Chng CL, Kurzawinski TR, Beale T. Value of sonographic features in predicting malignancy in thyroid nodules diagnosed as follicular neoplasm on cytology. Clin Endocrinol (Oxf). 2015;83(5):711-6.
-
Maia FFR, Matos PS, Pavin EJ, Zantut-Wittmann DE. Thyroid imaging reporting and data system score combined with Bethesda system for malignancy risk stratification in thyroid nodules with indeterminate results on cytology. Clin Endocrinol (Oxf). 2015; 82(3):439-44.
-
Elomami A, Elhag SA, Alseddeeqi E. Cytological Sub-Classification of Atypia of Undetermined Significance May Predict Malignancy Risk in Thyroid Nodules. Acta Cytol. 2021;65(3):205-212.
-
Kim SJ, Roh J, Baek JH, Hong SJ, Shong YK, Kim WB, et al (2017). Risk of malignancy according to sub-classification of the atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) category in the Bethesda system for reporting thyroid cytopathology. Cytopathology. 2017;28(1):65-73.
-
Valderrabano P, Khazai L, Thompson ZJ, Sharpe SC, Tarasova VD, Otto KJ, et al. Cancer Risk Associated with Nuclear Atypia in Cytologically Indeterminate Thyroid Nodules: A Systematic Review and Meta-Analysis. Thyroid. 2018;28(2):210-219.
-
Gweon HM, Son EJ, Youk JH, Kim JA. Thyroid nodules with Bethesda system III cytology: can ultrasonography guide the next step? Ann Surg Oncol. 2013;20(9):3083-8.
-
Ali SZ, Baloch, ZW, Cochand-Priollet B, Schmitt FC, Vielh P, VanderLaan PA. The 2023 Bethesda System for Reporting Thyroid Cytopathology. Thyroid. 2023;33(9):1039-1044.
-
Lee JH, Han K, Kim EK, Moon HJ, Yoon JH, Park VY, et al. Risk stratification of thyroid nodules with atypia of undetermined significance/follicular lesion of undetermined significance (AUS/ FLUS) cytology using ultrasonography patterns defined by the 2015 ATA Guidelines. Ann Otol Rhinol Laryngol. 2017;126(9):625-633.
-
Rosario PW. Thyroid nodules with atypia or follicular lesions of undetermined significance (Bethesda Category III): importance of ultrasonography and cytological subcategory. Thyroid. 2014;24(7): 1115-20.
Full Text Sources:
Abstract:
Views: 16021

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.