Surgery, Gastroenterology and Oncology

|
|
Neuroendocrine tumors (NETs) are rare malignancies that often metastasize to lymph nodes and the liver. Involvement of the breast as a metastatic site is exceptionally uncommon. This article presents the case of a female patient who underwent a right hemicolectomy for an ileal NET. One year later, a breast metastasis was found and the patient was submitted to a lumpectomy. The tumor cells were positive for chromogranin, synaptophysin and CDX-2. Distinguishing between primary breast NETs and metastatic NETs to the breast may be challenging and with utmost importance, due to the differences in treatment approaches. This case highlights the importance of considering metastatic NETs in the differential diagnosis of breast lesions, especially in patients with a history of NETs.
Introduction
Neuroendocrine tumors, originating from the neuroendocrine cell system, are rare malignancies most commonly found in the gastrointestinal tract and lungs (1,2). The small bowel, particularly the ileum, is recognized as a relatively common location for these tumors (3).
Characterized by their typically indolent growth, NETs exhibit a propensity for metastasizing to lymph nodes and liver (4). Breast involvement is exceedingly rare, accounting for less than 1% of metastases (3).
In this report, we describe a case of an ileal neuroendocrine tumor with breast metastases.
Case Report
A 56-year-old woman was referred to our hospital due to a small nodule on her right breast. Her medical history included an appendectomy for appendicitis in her 20s, as well as diagnoses of diabetes and hypertension. Her family history was unremarkable.
At the age of 55 the patient underwent right hemicolectomy with ileocolic anastomosis due to a neuroendocrine tumor of the terminal ileum at an external medical facility. The tumor was staged as pT2N1M0R0 – G1. No adjuvant treatment was required following surgery.
On physical examination, the breasts were noted to be symmetric, without any scars or deformities. No nipple retraction or spontaneous discharge were present. No masses were palpated.
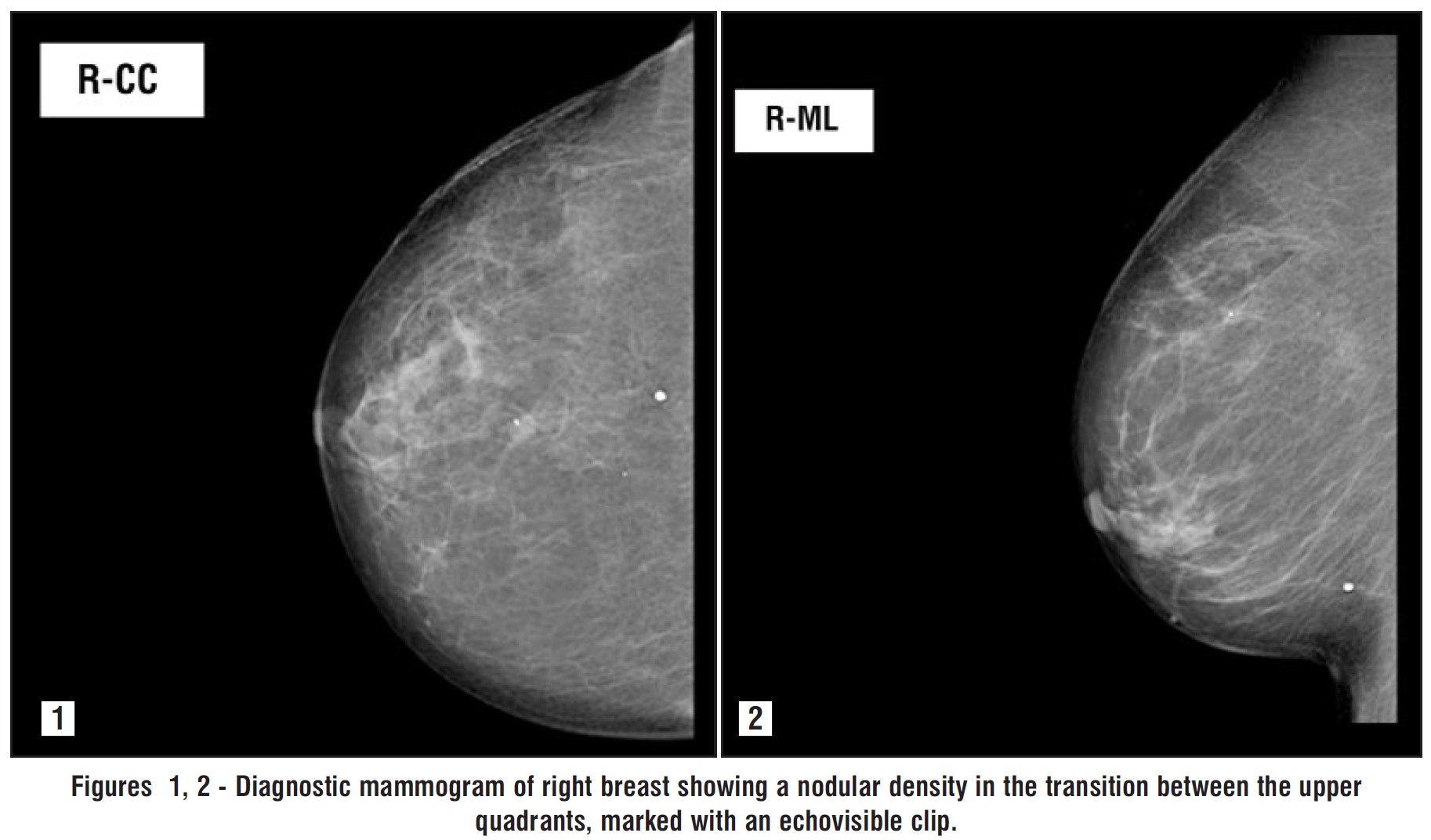
The patient did a screening mammogram (figs. 1 and 2), followed by a bilateral breast ultrasound, that showed a nodular density measuring 8 mm, projecting into the transition between the upper quadrants of the right breast. This finding was classified as BIRADS 4B. A percutaneous biopsy of the breast nodule was performed, and the pathologic examination was consistent with a metastasis of an ileal neuroendocrine tumor.
Figures 1, 2 - Diagnostic mammogram of right breast showing a nodular density in the transition between the upper quadrants, marked with an echovisible clip.
Following this, a 68Ga-DOTANOC PET and CT scan of the thorax, abdomen, and pelvis were conducted, ruling out any other secondary lesions.
Subsequently, an ultrasound-guided lumpectomy was performed. The postoperative course was uneventful and the patient was discharged the day after surgery.
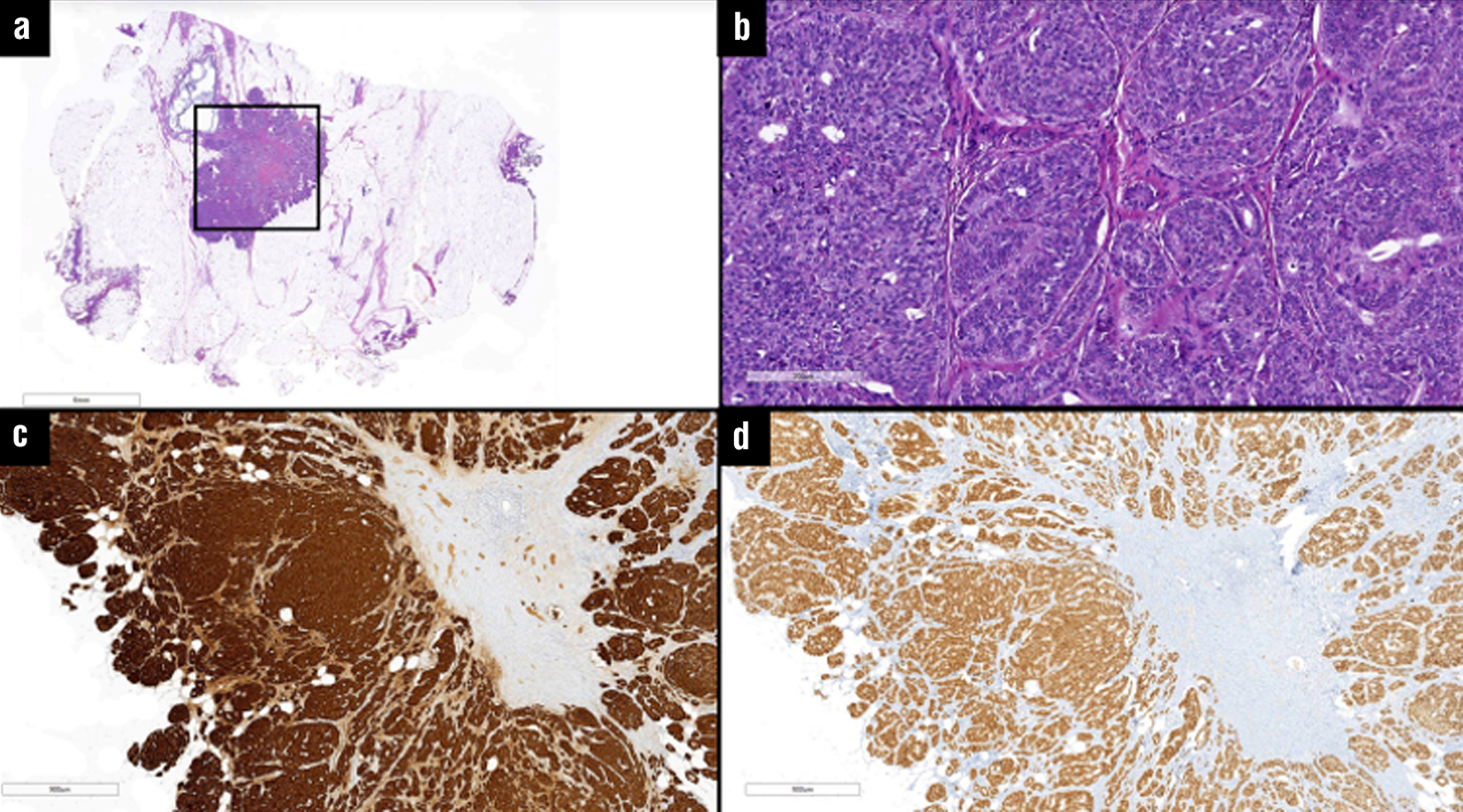
The pathology report of the right breast nodule confirmed it as a metastasis from an ileal neuro-endocrine tumor. The findings included two mitoses per 10 high-power fields (HPF), absence of lymphovascular or perineural invasion and negative surgical margins. Immunohistochemical staining was positive for synaptophysin, chromogranin, and CDX-2 and hormone receptor studies were negative for ER, PR and HER2 (fig. 3). The Ki-67 proliferative index was less than 1%.
Figure 3 - Breast metastasectomy specimen with a neuroendocrine tumor (a, H&E), well differentiated, with a nest and acinar pattern, consisting of polygonal cells with an eosinophilic and granular cytoplasm (b, H&E). The immunohistochemistry shows a diffuse expression of chromogranin and CDX2 (d and d, respectively) - compatible with metastasis from a primary neuroendocrine tumor of the ileum.
The case was discussed in the multidisciplinary tumor board and the follow-up was made with clinical evaluations at three and six months, along with a CT scan at the six-month mark. No evidence of recurrence was found during the follow-up assessments.
Discussion
Breast metastases from ileal NETs are very infrequent and few cases have been reported in the literature (3). Although NET metastases tend to be equally distributed between the quadrants of the breast, they exhibit a slight predilection for the right breast over the left (5).
The initial finding in our patient was a small nodule on a screening mammogram. There are no known pathognomonic radiologic characteristics of NET metastasis to the breast. They are similar to the other malignant breast lesions (6).
Breast metastases may mimic primary breast carcinoma both clinically and radiologically (7). We rely on histopathological examination to distinguish them. Some diagnostic problems arise from the overlap of morphological features between breast metastases from ileal NETs and invasive breast carcinomas, particularly those presenting neuroendocrine differentiation (3). In this case, prior knowledge of the patient's ileal NET facilitated a more straightforward diagnosis.
Chromogranin A and synaptophysin are sensitive and specific NET markers. However, they lack the
ability to differentiate between primary NETs of the breast and NET metastasis from another origin. Although most primary NETs of the breast express estrogen and progesterone receptors, this alone is not enough to distinguish between these entities (2). In this case, the tumor expressed chromogranin and synaptophysin. Besides that, the tumor stained diffusely positive for CDX-2, consistent with the final diagnosis of breast metastasis from an ileal neuro-endocrine tumor (4).
Due to the small number of metastatic ileal NETs to the breast, there are currently no established guidelines about the treatment of these tumors (3). Although the treatment of most metastatic neoplasms includes systemic therapy, in NET, the surgical resection with curative intent is the mainstay of treatment (4,8). For primary NETs of the breast, standard of care typically involves lumpectomy with radiation or chemotherapy. However, in cases of metastatic NETs to the breast, the excision of the lesion may be enough. Considering these differences in treatment, a correct diagnosis is of utmost importance (3,4,5).
Conclusion
We presented the case of a female patient with a history of neuroendocrine tumor originating from the ileum, who had previously undergone a right hemicolectomy. One year post-surgery, a routine screening mammogram revealed an incidental breast mass. Subsequent biopsy confirmed that the breast mass was a metastasis of the primary ileal neuroendocrine tumor.
Although this case did not involve complex diagnostic or treatment processes, the occurrence of breast metastases from ileal neuroendocrine tumors is exceptionally rare. This report aims to highlight the importance of considering such a diagnosis in patients with a history of neuroendocrine tumor. Awareness of this rare metastatic pattern is essential for accurate diagnosis and effective management of similar cases.
Conflicts of interest and source of funding
Authors declare no conflicts of interest.
This article received no external funding.
Ethical statement
Compliance with ethical standards.
References
1. Kamei DJ, Shiguihara RS, Araújo FR. Neuroendocrine tumor of the small intestine: case report. ABCD Arq Bras Cir Dig. 2020; 33(1):e1492. English, Portuguese
2. Díaz JA, González M, Romero-Rojas A, Strosberg J, Jiménez-Vásquez P. Neuroendocrine tumor metastases to the breast: a case report and review of the literature. Cureus. 2023;15(6):e40703.
3. Papalampros A, Mpaili E, Moris D, Sarlanis H, Tsoli M, Felekouras E et al. A case report on metastatic ileal neuroendocrine neoplasm to the breast masquerading as primary breast cancer - a diagnostic challenge and management dilemma. Medicine (Baltimore). 2019; 98(16):e14989.
4. Ahn S, Bhagwandin S, Reindl B, Jaffer S, Bickell N, Labow D et al. Metastatic Carcinoid Tumor Presenting as a Breast Mass: A Case Report and Review of the Literature. Arch Surg Oncol. 2016;2:111.
5. Dervishaj OA, Renzi AS, Genato R, Xiao PQ, Asarian AP. Neuroendocrine tumor of the breast: Is it primary or metastatic? Int J Case Rep Images. 2016;7(1):34-39.
6. Gîvan I, Ciulei G, Cozma A, Indre M, ?âru V, Pop A et al. Neuro-endocrine carcinoma of the breast: a case report. J Mind Med Sci. 2021;8(2): 306-311.
7. Solanki R, Gupta P, Sood A, Mittal BR. Breast metastasis arising from ileal neuroendocrine tumor: an unusual presentation. Nucl Med Mol Imaging. 2023;57(4):201-205.
8. Davis C, Castro J, Bass B, Bailey R. Ileal neuroendocrine tumor incidentally found on screening colonoscopy. ACS Case Reviews in Surgery. 2020;2(6):55–57.
Full Text Sources:
Abstract:
Views: 2026

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.