Surgery, Gastroenterology and Oncology

|
|
Background: Hepatocellular carcinoma (HCC) is a major type of liver tumor. It represents up to 90% of all liver malignancies. There are currently no reliable tumor markers or imaging technologies that can accurately diagnose early HCC. The use of circulating micro-RNAs (miRNAs or miR) as a potential tool for early detection of HCC has become an emerging area of study. Objectives: This study aimed to evaluate the role of miR-23b and miR-331 as biomarkers in HCC and chronic hepatitis C (CHC) patients.
Patients and Methods: This study included 100 subjects, selected from outpatient clinics of Damanhur Oncology Center from 1/1/2020 to 19/12/2021, they were classified into three groups. Group 1 included 40 patients with HCC, group 2 included 40 patients with chronic hepatitis C infection (CHC), and group 3 included 20 healthy control subjects. Complete blood count (CBC), liver function tests, Alfa fetoprotein (AFP) in addition to miR-23b and miR-331 was estimated in the serum of each studied groups.
Results: miRNA-23b gene expression level was significantly decreased in the HCC group when compared to the HCV and control groups. On the other hand, miRNA-331 gene expression level showed significantly higher expression level in the HCC group when compared to the HCV and control groups. The miRNA-23b gene expression level showed significantly decreased level associated with increased BCLC stage, increased tumor size, multiplicity. While higher miRNA-331 gene expression level was significantly associated with higher BCLC stage, larger tumor size, multiple lesions.
Conclusion: Serum miR-331 and miR-23b are suggested to be predictors for development and complications of HCC.
Abbreviations: AFP: alpha fetoprotein; AUC: area under ROC curve; BCLC: Barcelona-clinic liver cancer; CBC: complete blood count; CHC: chronic hepatitis C; CHCV: chronic hepatitis C virus infection;
CLD: chronic liver diseases; CT: computed tomography; HBV: hepatitis B virus; HCC: hepatocellular carcinoma; HCV: hepatitis C virus; miR: micro RNA; MRI: magnetic resonance imaging; NAFLD: nonalcoholic fatty liver disease; ROC: receiver operating characteristic curve; TNM: tumor-node-metastasis.
Background
Hepatocellular carcinoma (HCC) is a primary tumor of the liver. It occurs in approximately 85% of patients diagnosed with cirrhosis. HCC is now the fifth most common cause of cancer worldwide. The second leading cause of cancer death after lung cancer in men is HCC. The five-year survival of HCC is 18% and second to pancreatic cancer. The annual incidence of HCC in patients with cirrhosis is 2-4% (1).
Non-alcoholic fatty liver disease (NAFLD) is now a leading cause of HCC worldwide, especially in western countries. In Egypt, it represents the fourth common cancer (2). There are many risk factors that play an important role in the development of HCC: Both hepatitis B virus (HBV) and hepatitis C virus (HCV) infection increase HCC risk by 20-fold (3). Non-cirrhotic related HCC may be asymptomatic in the early stage of the disease. Cirrhotic-related HCC patients may present with symptoms of decompensated liver failure. The most common extra hepatic metastasis of HCC is to the lung, intra-abdominal lymph node, bone, and adrenal, respectively (4).
HCC may be diagnosed on ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI) (5). Liver biopsy is not routinely performed for HCC (6). Patients with Barcelona- clinic liver cancer (BCLC) classification of very early (0) and early-stage (A) are ideal candidates for surgical resection (7). Patients with Child–Turcotte–Pugh A and without clinically significant portal hypertension have favorable surgical resection outcomes (8). Liver transplantation is associated with the removal of tumors and the potential for cure (9). Patients with BCLC classification of very early (0) and early-stage (A) who do not meet surgical resection criteria are appropriate for ablation (10). Tumor-node-metastasis (TNM) does not account for the degree of performance status and liver dysfunction. The most widely used staging system is the Barcelona clinic liver cancer (BCLC), which offers the most prognostic information. The system stratifies patients with HCC in one of five stages. Substrata of 0, A, B, C, and D providing treatment (11).
MicroRNAs are small non-coding RNAs (12). Although some extracellular miRNAs are regarded as by-products of cellular activities, such as cell injury or death, increasing evidence suggests that the release of extracellular miRNAs is a regulated process (13). miRNAs modulate the expression of approximately 30% of all human genes, many of which are tumor-associated or are in regions of instability in the genome. There is clear evidence of key roles for miRNAs in human carcinogenesis (14).
Various miRNAs, such as miR-122 and miR-132, play pivotal roles in the innate and adaptive immunity involved in hepatic inflammation. miR-122 is the most representative miRNA in the liver, and its loss results in inflammation, fibrosis, and HCC, indicating that miR-122 modulates anti-inflammatory effects (15). Various HCC-associated miRNAs, including miR-21, miR-221, and miR-222, are increased in HCC, whereas others, such as miR-122a, miR-145, miR-199a, and miR-223, are decreased in this disease. Several HCC-specific miRNAs have recently been classified; miRNA profiles differed between hepatocytes and HCC cells (16).
Recent studies have demonstrated that miRNAs, including miR-92a, miR-221, miR-487a, and miR-1468, have the potential to serve as prognostic biomarkers (17). The miR-23b and miR-331 have been evaluated in previous studies in HCC Chinese population (18). The aim of this study is to evaluate the role of miR-23b and miR-331 as biomarkers in HCV-Related HCC and chronic hepatitis C (CHC) in Egyptian patients.
Patients and Methods
The current study aimed to evaluate the role of miR-23b and miR-331 as biomarkers in HCC and chronic hepatitis C (CHC) Egyptian patients. This study is a comparative case-control study. This study was carried out on 100 individuals selected from outpatient clinics of Damanhur Oncology Center from 10/1/2020 to 15/12/2021. They were classified into three groups. Group 1 included 40 patients diagnosed as HCC, group 2 included 40 patients diagnosed as chronic hepatitis C virus infection (CHCV), and group 3 included 20 healthy subjects taken as control group. This study was approved by the Ethical committee of the Faculty of Pharmacy, Damanhur University (reference no. 420PB18). An informed written consent was obtained from all participants prior to enrollment in the study. Regarding HCC cases, the mean age was 59.3 years, there were 85% males and 15% females. While the mean age of CHCV positive cases was 46.9 years, they were 65 % males and 35% females. Twenty healthy control subjects were recruited to the study as a control group. They were matched with HCC and CHCV groups regarding age and gender. All patients were subjected to the following: patients assessment, name, age, history of blood transfusion, history of previous operations; full history, history of jaundice, history of abdominal distension or weight loss or night sweating, history of hematemesis or bleeding per rectum, history of hepatic coma or encephalopathy; family history of hepatitis C infection or hepatocellular carcinoma; drug history, complete clinical examination, laboratory assessment to verify the diagnosis and patient general conditions, which included CBC, liver function tests, INR, AFP. Moreover, all subjects (HCC group) underwent Triphasic CT of the abdomen to assess the diagnosis and complications.
Determination of miR-23b, miR-331 in serum by RT-PCR
Extraction of miR331 and miR23b from serum samples: miRNeasy mini kit (Geneaid, Taiwan, Catalog no. 217004). miR-331 and miR-23b Amplification and quantification was done using Quantitative Real Time PCR By using SYBR Green PCR Kit: (QIAGEN Germany, Catalog no 218073, 218075, 218076). The master mix was aliquoted into separate 0.2 ml PCR tubes before adding the DNA template, mixed gently and centrifuged. Briefly, the cycling conditions were stage 1, 95°C for 15 min, stage 2, 94°C for 30 sec and 55°C for 60 and 70°C for 60 sec. Stage 2 was repeated for 39 cycles. Reactions were added and incubated into qPCR thermocycler, during the last stage, SYBR Green intercalates with the amplicon to generate a fluorescent signal which is detected by PCR instrument. Once the reaction is complete Ct value data were analyzed for gene expression. After the end of the program, the expression of miR-331and miR- 23b levels in each sample were finally determined after correction with Housekeeping gene expression level. Controls were chosen as the reference samples, and fold changes in the levels of miR-331and miR- 23b were determined by 2-ΔΔCT (cycle threshold) method and expressed as fold change (FC) using Step One software (Applied Biosystems, USA).
Statistical analysis
Data were fed to the computer and analyzed using IBM SPSS software package version 25.0. (Armonk, NY: IBM Corp). Chi-square test was used for categorical variables, to compare between different groups; One way ANOVA test was used for normally distributed quantitative variables, to compare between more than two groups, and Post Hoc test (Tukey) for pairwise comparisons; Mann Whitney test, was used for not normally distributed quantitative variables, to compare between two studied groups; Kruskal Wallis test, for not normally distributed quantitative variables, to compare between more than two studied groups, and Post Hoc (Dunn's multiple comparisons test) for pairwise comparisons; Spearman coefficient was used to correlate between two distributed abnormally quantitative variables; Receiver operating characteristic curve (ROC) was generated by plotting sensitivity on Y axis versus 1-specificity on X axis at different cut off values. The area under the ROC curve denotes the diagnostic performance of the test. An area of more than 50% gives acceptable performance and an area about 100% is the best performance for the test. The ROC curve also allows a comparison of performance between two tests. All tests were considered significant if p value <0.05.
Results
The results showed a significant increase in AFP concentration in the HCC group when compared to both CHCV and control groups. Regarding to miRNA-23b gene expression level, the results showed significant decrease in miRNA-23b gene expression level in the HCC group when compared to CHCV and control groups. On the other hand, miRNA-331 gene expression level showed significantly
higher miRNA-331 gene expression level in the HCC group when compared to CHCV and control groups. Table 1 and fig. 1 illustrate these results.
Table 1 - Comparison between the three studied groups according to AFP, miRNA-23b, and miRNA-331

Figure 1 - Comparison between the three studied groups according to (a) AFP, (b) miRNA-23b, and (c) miRNA-331. a: Significant with Control b: Significant with HCV

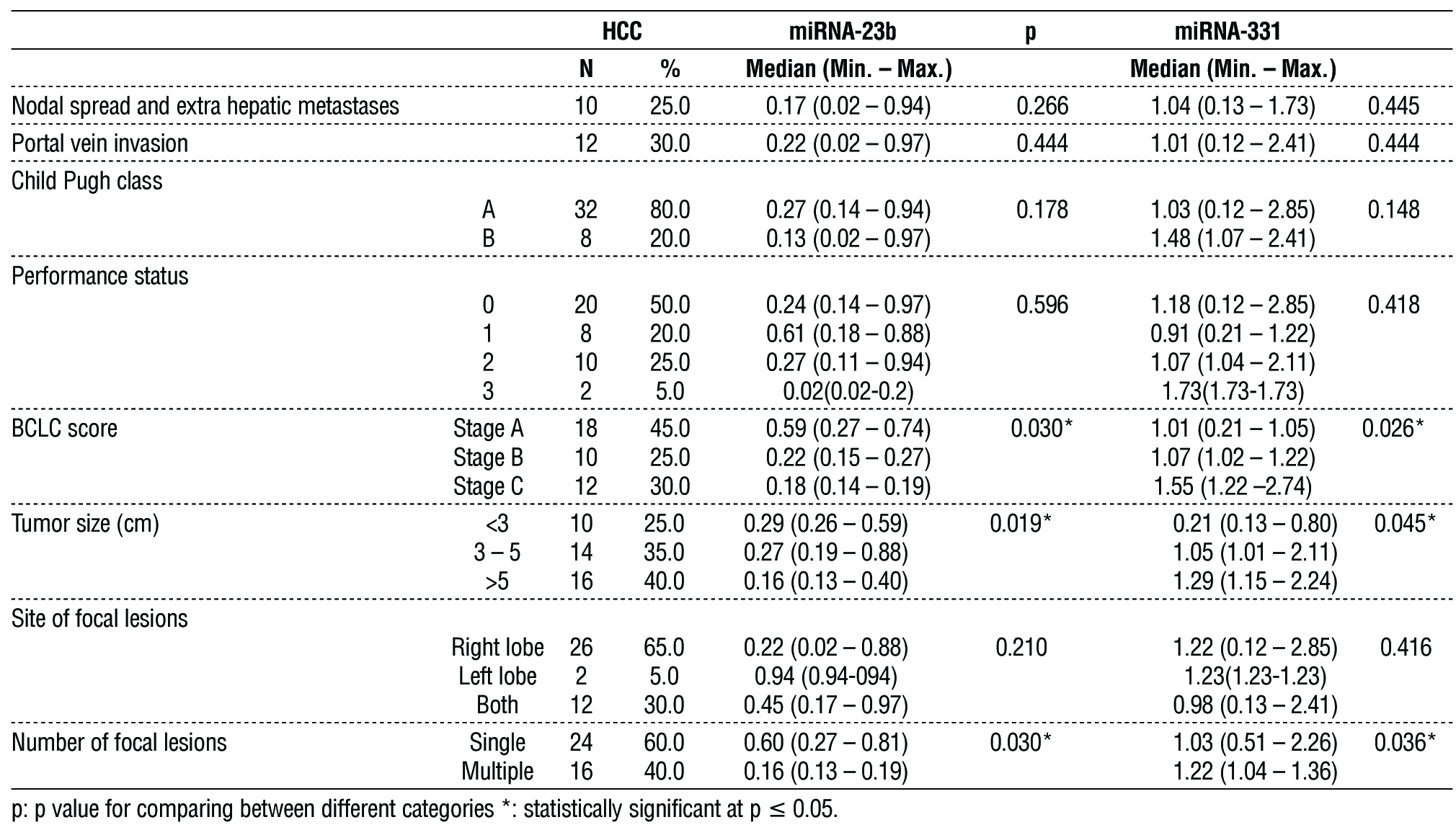
Among all studied HCC cases, Nodal spread, and extra hepatic metastases was present in 25%, while Portal vein invasion was present in 30% of all studied HCC cases, Child Pugh classes were assessed, 80% had class A, 20% had class B. Performance status was evaluated for all HCC cases, 50% had status 0, 20% had status 1, 25% had status 2, 5% had status 3. BCLC score was calculated, 45% had stage A, 25% had stage B, and 30% had stage C. Tumor size was <3 cm in 25%, from 3 to 5 cm in 35%, and more than 5 cm in 40%. Most lesions were found in the right lobe (65%), while only 5% were found in the left lobe and 30% were found in both lobes. The miRNA-23b gene expression level showed significantly decreased level associated with increased BCLC stage, increased tumor size, multiplicity. While it did not differ significantly according to metastasis, PV invasion, Child Pugh classes, PS, lesion side. On the other hand, higher miRNA-331 gene expression level was significantly associated with higher BCLC stage, larger tumor size, and multiple lesions. Otherwise, it did not differ significantly according to metastasis, PV invasion, Child Pugh classes, PS, lesion side. Table 2 clarifies theses data.
Table 2 - Association of miRNA-23b and miRNA-331 with different parameters in HCC group
Receiver operating characteristic (ROC) curve was conducted for discrimination of CHCV patients from control subjects. Moderate accuracy AUCs were found regarding AFP and miRNA-23b (AUC=0.74, 0.708 respectively).
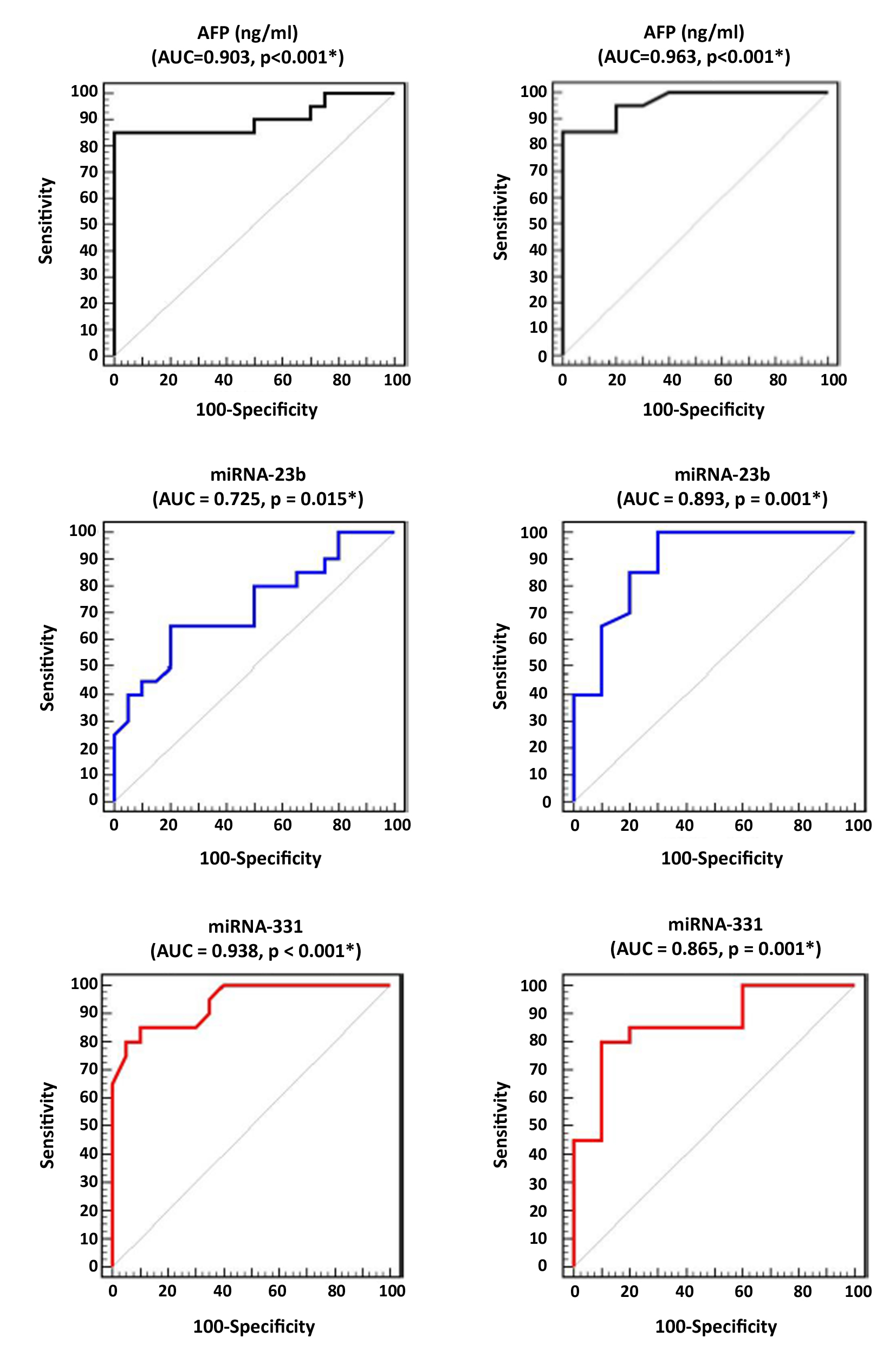
While miRNA-331 showed low accuracy AUC (AUC=0.635). Best cut off values and perform ace characteristics are shown in Combining different markers, increased AUC of miRNA-331 when combined to AFP to 0.795 and when combined to miRNA-23b to 0.700; increased AUC of miRNA-23b when combined to AFP to 0.765; increased AUC of AFP when combined to miRNA-331 to 0.795, and when combined to miRNA-23b to 0.765. In addition, ROC curve was conducted for discrimination of HCC patients from control subjects. High accuracy AUC was found regarding AFP (AUC=0.963). While miRNA-23b and miRNA-331 showed moderate accuracy AUCs (AUC=0.893, 0.865 respectively).
Best cut off values and performance characteristics are shown in fig. 2. Combining markers led to increased HCC diagnostic ability of miRNA-23b and miRNA-331. Fig. 2 represents these results.
Figure 2 - ROC curves for discrimination between HCC and CHCV cases regarding(a) AFP, (b) miRNA-23b, (c) miRNA-331, discrimination between HCC and controls regarding (d) AFP, (e) miRNA-23b, and (f) miRNA-331.
Regression analysis was conducted for prediction of HCC susceptibility using, age, gender, AFP, miRNA-23b, and miRNA-331 as covariates. Higher AFP, miRNA-331, lower miRNA-23b were considered as predictors of HCC susceptibility in uni- and multi-variable analyses as showed in (table 3).
Table 3 - Regression analysis for prediction of HCC susceptibility

Moreover, regression analyses were conducted for prediction of HCC complications. Higher AFP, miRNA-331, lower miRNA-23b were considered as predictors of HCC higher BCLC stage. Higher miRNA-331, lower miRNA-23b was considered as predictors of HCC larger tumor size. Lower miRNA-23b was considered as predictor of HCC multiplicity. None of the confounders was considered as predictor of PV invasion. Table 4 demonstrated theses data.
Table 4 - Regression analysis for prediction of HCC complications

Discussion
Liver cancer remains a global health challenge, with an estimated incidence of >1 million cases by 2025. Infection by hepatitis B virus and hepatitis C virus are the main risk factors for HCC development, although non-alcoholic steatohepatitis associated with metabolic syndrome or diabetes mellitus is becoming a more frequent risk factor in the West (19). Aberrant miRNA expression has been identified in a variety of human cancers including HCC. In addition to up- and down-regulated miRNAs were reported in HCC tissues (20).
AFP concentration in the current study was significantly higher in HCC group when compared to CHCV and control groups, which was in same line with previous studies, found that elevated AFP levels are associated with higher pathological grade (21). AFP measurements showed a statistically significant difference between the studied groups, which increased in HCC in comparison to cirrhosis and the control group (22). The present study revealed that significant decrease in miRNA-23b gene expression level in HCC group when compared to CHCV and control groups. On the other hand, higher miRNA-331 gene expression level was found in HCC group when compared to CHCV and control groups. For discrimination of HCC patients from control subjects, ROC curve was conducted. High accuracy AUC was found regarding AFP. In addition, miRNA-23b and miRNA-331 showed moderate accuracy AUCs. These results agreed with Sun et al., 2019 who found that serum miR-331-3p was significantly higher in early-stage HCC than that in chronic liver diseases (CLD) and HCV infection respectively, and its level was decreased significantly after surgery in early-stage HCC. Contrarily, serum miR-23b-3p was significantly lower in early-stage HCC and increased significantly after surgery (23).
Furthermore, ROC demonstrated AUC for serum miR-23b-3p in discriminating early-stage HCC from CLD patients, higher than that for AFP. In discrimination early-stage HCC from severe fibrosis/cirrhosis patients, both miR-23b-3p and miR-331-3p had better diagnostic performances than AFP. Serum miR-331-3p levels also showed a significant correlation with BCLC stages of HCC (23). Mohamed et al., 2017, found that serum microRNA 23a level was significantly higher in the HCC group in comparison to other groups (24).
The miRNA-23b gene expression level showed significantly decreased level associated with increased BCLC stage, increased tumor size, multiplicity, while higher miRNA-331 gene expression level was significantly associated with higher BCLC stage, larger tumor size, and multiple lesions. ROC curve was conducted for discrimination of HCV patients from control subjects. Moderate accuracy AUCs were found regarding AFP and miRNA-23b, while miRNA-331 showed low accuracy AUC. The diagnostic sensitivities and specificities of both miR-331-3p and miR-23b-3p had been calculated using the ROC curves, it was shown that miR-23b-3p had the best sensitivity (80%) and specificity (74%), miR-23b-3p had better sensitivity compared to miR-331-3p, but miR-331-3p showed the highest specificity (25).
High accuracy AUC was found regarding AFP and miRNA-331, while miRNA-23b showed moderate accuracy AUC in our study which is in agreement with Wu et al. (26). On the other hand, serum
miR-331-3p was significantly increased in HCC compared to patients with benign hepatic tumors and was associated with poor HCC prognosis (27). Moreover, miR-23b-3p showed a significant decrease in the plasma of patients with early HCC compared to cirrhotic patients. (28) These results are consistent with those results reported previously by Cao et al. 2017 (29).
Higher AFP, miRNA-331, lower miRNA-23b were considered as predictors of HCC susceptibility. Elgamal et al., 2018 found that age greater than 58 years, females, hypoalbuminemia, and AFP greater than 11.2 can predict 76.3% of HCC cases (30). We also suggested that lower miRNA-23b may be considered as predictor of HCC multiplicity, while none of the studied confounders was considered as predictor of PV invasion.
Limitation of the study was small sample size and future studies should be done in large number of patients to verify our results.
Conclusion
Serum miRNA-331 is a more effective predictor than miRNA-23b and AFP for the development of HCC in cirrhotic HCV patients. Lower miRNA-23b and higher miRNA-331 may be responsible for HCC development, higher stage, larger tumor size and multiplicity.
Author's contributions
All authors included in this research work, read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Source of funding
This study did not receive any funding
Ethics approval and consent to participate
This study was approved by the Ethical committee of the Faculty of Pharmacy, Damanhour University (reference no. 420PB18). An informed written consent was obtained from all participants prior to enrollment in the study.
References
1. Asafo-Agyei KO, Samant H. Hepatocellular Carcinoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
2. Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, Allen C, et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level. JAMA Oncol. 2017;3(12):1683-1691.
3. Zhao C, Nguyen MH. Hepatocellular Carcinoma Screening and Surveillance. J Clin Gastroenterol. 2016;50(2):120-33.
4. Harding JJ, Abu-Zeinah G, Chou JF, Owen DH, Ly M, Lowery MA, et al. Frequency, Morbidity, and Mortality of Bone Metastases in Advanced Hepatocellular Carcinoma. J Natl Compr Canc Netw. 2018;16(1):50-58.
5. D'Onofrio M, Faccioli N, Zamboni G, Malagò R, Caffarri S, Fattovich G, Mucelli RP. Focal liver lesions in cirrhosis: value of contrast-enhanced ultrasonography compared with Doppler ultrasound and alpha-fetoprotein levels. Radiol Med. 2008 Oct;113(7):978-91.
6. Jain D. Tissue diagnosis of hepatocellular carcinoma. J Clin Exp Hepatol. 2014 Aug;4(Suppl 3):S67-73.
7. Roayaie S, Jibara G, Tabrizian P, Park JW, Yang J, Yan L, et al. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology. 2015;62(2):440-51.
8. Bruix J, Takayama T, Mazzaferro V, Chau GY, Yang J, Kudo M, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo- controlled trial. Lancet Oncol. 2015;16(13):1344-54.
9. Llovet JM, Mas X, Aponte JJ, Fuster J, Navasa M, Christensen E, et al. Cost effectiveness of adjuvant therapy for hepatocellular carcinoma during the waiting list for liver transplantation. Gut. 2002;50(1):123-8.
10. Germani G, Pleguezuelo M, Gurusamy K, Meyer T, Isgrò G, Burroughs AK. Clinical outcomes of radiofrequency ablation, percutaneous alcohol and acetic acid injection for hepatocelullar carcinoma: a meta-analysis. J Hepatol. 2010;52(3):380-8.
11. Bruix J, Sherman M., American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020-2.
12. Ha M, Kim VN. Regulation of microRNA biogenesis. Nature reviews Molecular cell biology. 2014;15(8):509-24.
13. Cui M, Wang H, Yao X, Zhang D, Xie Y, Cui R, et al. Circulating microRNAs in cancer: potential and challenge. Front Genet. 2019; 10:626.
14. Si W, Shen J, Zheng H, Fan W. The role and mechanisms of action of microRNAs in cancer drug resistance. Clin Epigenetics. 2019; 11(1):25.
15. Hsu S-H, Wang B, Kota J, Yu J, Costinean S, Kutay H, et al. Essential metabolic, anti-inflammatory, and anti-tumorigenic functions of miR-122 in liver. J Clin Invest. 2012;122(8):2871-83.
16. Tomimaru Y, Eguchi H, Nagano H, Wada H, Kobayashi S, Marubashi S, et al. Circulating microRNA-21 as a novel biomarker for hepatocellular carcinoma. J Hepatol. 2012;56(1):167-75.
17. Zhang T, Liu W, Zeng X-C, Jiang N, Fu B-S, Guo Y, et al. Down-regulation of microRNA-338-3p promoted angiogenesis in hepatocellular carcinoma. Biomed. Pharmacother. 2016;84:583-591.
18. Chang RM, Yang H, Fang F, Xu JF, Yang LY. MicroRNA-331-3p promotes proliferation and metastasis of hepatocellular carcinoma by targeting PH domain and leucine- rich repeat protein phosphatase. Hepatology. 2014;60(4):1251-63.
19. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6.
20. Yang N, Ekanem NR, Sakyi CA, Ray SD. Hepatocellular carcinoma and microRNA: new perspectives on therapeutics and diagnostics. Adv Drug Deliv Rev. 2015;81:62-74.
21. Everhart JE, Wright EC, Goodman ZD, Dienstag JL, Hoefs JC, Kleiner DE, et al. Prognostic value of Ishak fibrosis stage: findings from the hepatitis C antiviral long-term treatment against cirrhosis trial. Hepatology. 2010;51(2):585-94.
22. Mohamed B, Serag W, Abdelal R, Elsergany H. S100A14 protein as diagnostic and prognostic marker in hepatocellular carcinoma. Egyptian Liver Journal. 2019;9:9.
23. Sun Q, Li J, Jin B, Wang T. Evaluation of miR-331-3p and miR-23b-3p as serum biomarkers for hepatitis c virus-related hepatocellular carcinoma at early stage. Clin Res Hepatol Gastroenterol. 2020; 44(1):21-28.
24. Mohamed A, Ali-Eldin Z, Elbedewy T, El-Serafy M, Ali-Eldin F, and AbdelAziz H. MicroRNAs and clinical implications in hepatocellular carcinoma. World J Hepatol. 2017;9(23):1001–1007.
25. Sun Q, Li J, Jin B, Wang T, Gu J. Evaluation of miR-331-3p and miR-23b-3p as serum biomarkers for hepatitis c virus-related hepatocellular carcinoma at early stage. Clin Res Hepatol Gastroenterol. 2020;44(1):21–28.
26. Wu G, Wu J, Wang B, Zhu X, Shi X and Ding Y. Importance of tumor size at diagnosis as a prognostic factor for hepatocellular carcinoma survival: a population-based study. Cancer Manag Res. 2018;10: 4401-4410.
27. Aboelwafa RA, Ellakany WI, Gamaleldin MA Saad MA. The expression of microRNA-331-3p and microRNA-23b3 in Egyptian patients with early-stage hepatocellular carcinoma in hepatitis C-related liver cirrhosis. Egypt Liver Journal. 2021;11:49.
28. Chen L, Chu F, Cao Y, Shao J, Wang F. Serum miR-182 and miR-331-3p as diagnostic and prognostic markers in patients with hepatocellular carcinoma. Tumour Biol. 2015;36(10):7439–7447.
29. Cao J, Liu J, Long J, Fu J, Huang L, Li J, et al. microRNA-23b suppresses epithelial-mesenchymal transition (EMT) and metastasis in hepatocellular carcinoma via targeting Pyk2. Biomed Pharmacother. 2017;89:642-650.
30. Elgamala S, Ghafara A, Ghoneem E, Elshaerb M, Alrefaib H, Elemshaty W. Characterization of patients with hepatocellular carcinoma on the way for early detection: one center experience. The Egyptian Journal of Internal Medicine. 2018;30:231-238.
Full Text Sources:
Abstract:
Views: 2516

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.