Surgery, Gastroenterology and Oncology

|
|
Background: The Alvarado score is a widely used clinical tool for diagnosing acute appendicitis, especially in emergency settings. However, its diagnostic accuracy in patients with intermediate scores (5–7) remains uncertain. Aim: To assess the incidence of confirmed acute appendicitis in patients with Alvarado scores between 5 and 7 and to evaluate the reliability of the Alvarado scoring system in this diagnostic range.
Patients and Methods: A prospective observational study was conducted 228 patients
presenting with symptoms and signs of acute appendicitis to the emergency department at t Imam Hussain Medical City during the period from 1st January 2024 31st December 2024. All patients underwent clinical evaluation using the Alvarado scoring system and were subsequently treated surgically. Final diagnoses were confirmed through operative and histopathological findings. Sensitivity, specificity, and predictive values of the score were calculated.
Results: Of the 228 patients, 59 (25.88%) had Alvarado scores between 5 and 6, while 169 patients (74.12%) had a score of 7. According to operative findings, 198 patients (86.84%) were confirmed to have acute appendicitis, while 30 patients (13.16%) had other pathologies and appendicular mass. The overall sensitivity and specificity of the Alvarado score were 83.33% and 86.87%, respectively. However, in, the negative predictive value was notably lower at 45.72%, indicating limited reliability in excluding appendicitis in this subgroup.
Conclusion: Although the Alvarado score shows good overall diagnostic performance, its predictive accuracy in the 5–7 score range is limited. Patients with intermediate scores require further diagnostic evaluation using imaging and close clinical monitoring to avoid misdiagnosis or unnecessary surgery.
INTRODUCTION
Globally, acute appendicitis represents a prevalent surgical emergency, with an estimated lifetime incidence of 1 in 7, indicating that approximately 6% of individuals will experience an episode of this condition throughout their lives (1). The diagnosis of this ailment is particularly challenging, especially during the initial stages, when the classical clinical signs and symptoms tend to be rather insidious (2). Various pathological processes can simulate the clinical presentation of acute appendicitis, as there exists a multitude of etiologies resulting in discomfort localized to the right iliac fossa, particularly among female patients (3).
It has been documented that a considerable number of patients who undergo appendectomy exhibit negative findings upon histopathological examination of the resected appendix, which serves as the definitive diagnostic criterion for appendicitis (4). The removal of an intact appendix imposes significant burdens on both patients and healthcare resources (5). Nevertheless, the early identification of the condition coupled with timely surgical intervention has emerged as the most critical factors in mitigating morbidity, potential mortality, duration of hospitalization, and overall treatment expenditures (6).
Numerous scoring systems have been developed to facilitate the early diagnosis and timely management of acute appendicitis. These scoring systems are recognized as valuable and reliable tools for distinguishing between acute appendicitis and nonspecific abdominal discomfort (2). One notable example is the Alvarado scoring system, which integrates histopathological data, physical examination findings, and select laboratory tests, and is characterized by its ease of application (6). Nonetheless, a definitive diagnosis can ultimately be established during surgical intervention and subsequent histopathological evaluation (7).
The present study aimed to assess the incidence of confirmed acute appendicitis in patients with Alvarado scores between 5 and 7 and to evaluate the reliability of the Alvarado scoring system in this diagnostic range.
PATIENTS AND METHODS
Study Population
This is a prospective observational study including a total of 228 patients presenting with symptoms and signs of acute appendicitis to the emergency department at t Imam Hussain Medical City during the period from 1st January 2024 31st December 2024. These include acute onset abdominal pain mainly in the right lower quadrant, nausea, vomiting, anorexia, elevated temperature, and right lower quadrant tenderness and rebound tenderness (by physical examination). The study was approved by Arab Council for Health Specializations. The study included patients of any age group and both sexes that presenting to the emergency department sign and symptoms indicating acute appendicitis and operated with appendectomy. Patients with no documented Alvarado score, those who did not have an abdominal ultrasound, pregnant women, patients taking nonsteroidal anti-inflammatory drugs and those with Alvarado score <5 and >7 were excluded from the study.
A verbal consent from each participant was obtained prior to data collection after explaining the aim of study. The confidentiality of data throughout the study was guaranteed and the patients were assured that data will be used for research purpose only.
Data Collection
All included patients were admitted after initial assessment in the emergency department and demographic characteristics including age and sex, and baseline investigations including total white blood cell (WBC) count, neutrophil % and hemoglobin (Hb) concentration were reported.
Alvarado Score
The Alvarado score was calculated based on clinical symptoms (migration of pain, anorexia, nausea/vomiting), signs (tenderness in the right lower quadrant, rebound tenderness, elevated temperature), and laboratory findings (leukocytosis and left shift of neutrophils). The sum of the score was assigned to each patient.
Ultrasonography
US examination was performed using ultrasound device (Philips HD 11xe 2011), with 5-7.5 MHz probe. The criteria for positivity-included visualization of non- compressible tubular and blind-ended non-peristaltic structure with diameter of 6 mm or more in right lower quadrant, the demonstration of Appendicoliths, Probe tenderness, increased echogenicity of the periappendiceal fat and free intraperitoneal fluid particularly in right iliac fossa (RIF) or pelvis. The criteria of negativity were non-visualization of appendix or visualization of normal appendix with or without alternative diagnosis (8).
Surgical Technique
Open appendectomy was executed via a right lower quadrant incision (commonly utilizing either a McBurney or Lanz incision) under general anesthesia. Following the incision of the skin and fascial layers, access to the peritoneal cavity was achieved, wherein the appendix was located. In instances of inflammatory adhesions, they were meticulously dissected. The mesoappendix was ligated, after which the appendix was excised subsequent to the placement of a transfixing ligature at its base. Hemostasis was assured, and the peritoneal cavity was lavaged if any contamination was detected. The incision was sutured in layers, and the management of the wound was contingent upon intraoperative findings, with or without the use of drainage.
Laparoscopic appendectomy was conducted under general anesthesia utilizing the conventional three-port technique. Upon the establishment of pneumo-peritoneum, trocars were introduced through the umbilicus, the suprapubic region, and the left lower quadrant. The appendix was identified, followed by careful dissection and sealing of the mesoappendix employing either electrocautery or clips. The base of the appendix was ligated with the use of endoloops or staplers, and the appendix was extracted through the umbilical port. The abdominal cavity was irrigated in the event of encountering purulent fluid or other forms of contamination. Hemostasis was verified, and the ports were withdrawn under direct visualization. The incisions were subsequently closed in layers, and patients were monitored in the postoperative period for any complications that may arise. The definitive diagnosis was based on the histopathological assessment of the specimen
Statistical Analysis
All data were analyzed with statistical package for social sciences (SPSS) software (version 26). Descriptive statistics were used to present the data. Continuous variables are presented as mean± standard deviation (SD); categorical variables were presented as frequencies and percentages. The diagnostic value of Alvarado and ultrasound was calculated as follow considering the surgical finding as a gold standard:
Sensitivity in percentage: (TP/TP + FN) * 100;
Specificity in percentage: (TN/TN+FP) * 100;
Positive predictive value (PPV) in percentage: (TP/ TP + FP)* 100;
Negative predictive value (NPV) in percentage: (TN/ TN +FN) * 100;
Diagnostic accuracy in percentage: (TP + TN/ TP +TN + FP + FN) * 100.
RESULTS
Demographic Characteristics of the Patients
Table 1 - Demographic characteristics of the patients with acute appendicitis (n=228)
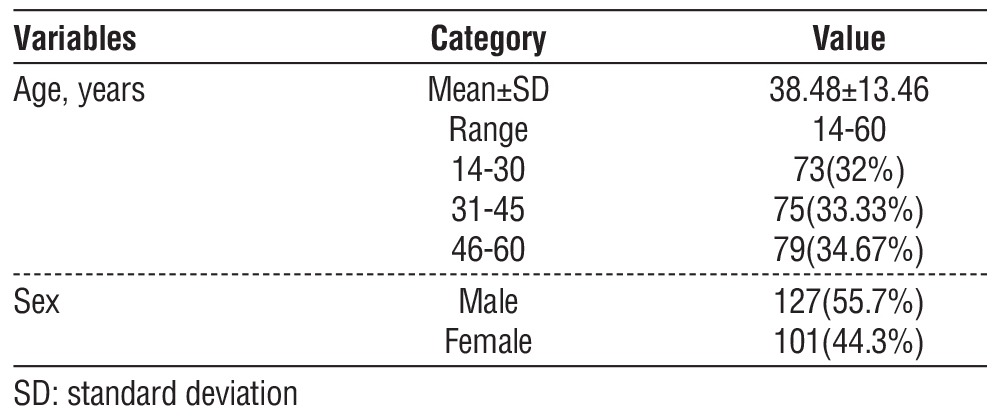
Table 1 presents the demographic characteristics of the 228 patients suspected to have acute appendicitis. The age distribution shows a mean age of 38.48±13.46 years, and the ages ranged from 14 to 60 years; of whom 32% were aged 14-30 years (n=73), 33.33% were 31-45 years (n=75), and 34.67% were 46-60 years (n=79). In terms of sex distribution, 127 patients (55.7%) were male, and 101 patients (44.3%) were female.
Clinical Characteristics of the Patients
Table 2 - Clinical characteristics of the patients with acute appendicitis (n=228)
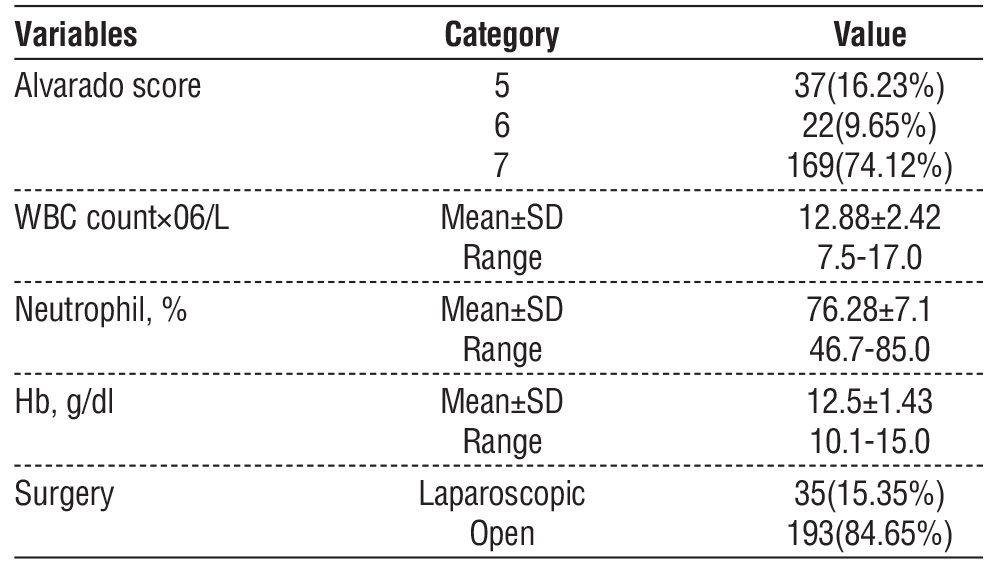
Table 2 summarizes the clinical characteristics of patients. Based on the Alvarado scoring system, 169 patients (74.12%) had a score of 7 , 37patients (16.23%) had a score 5 and 22 patients (9.65%) had score 6. The mean WBC count was 12.88 × 10?/L, with a range of 7.5 to 17.0, indicating a general trend of leukocytosis among patients. The mean neutrophil percentage was 76.28%, ranging from 46.7% to 85.0%. The mean Hb level was 12.5 g/dL, with values ranging from 10.1 to 15.0 g/d. Laparoscopic surgery was performed in 35 patients (15.35%) while 193 patients (84.65%) undergone open surgery.
Ultrasound Findings
According to US findings, 51 patients (22.37%) had normal appendix. Highly inflamed appendix was the most common findings account for 162 patients (71.11%) and finally perforated viscus (6.58%) as shown in fig. 1. Accordingly, acute appendicitis was detected in 177 patients based on US.
Figure 1 - Distribution of patients according to US findings Figure 2 - The proportion of acute appendicitis according to operative findings
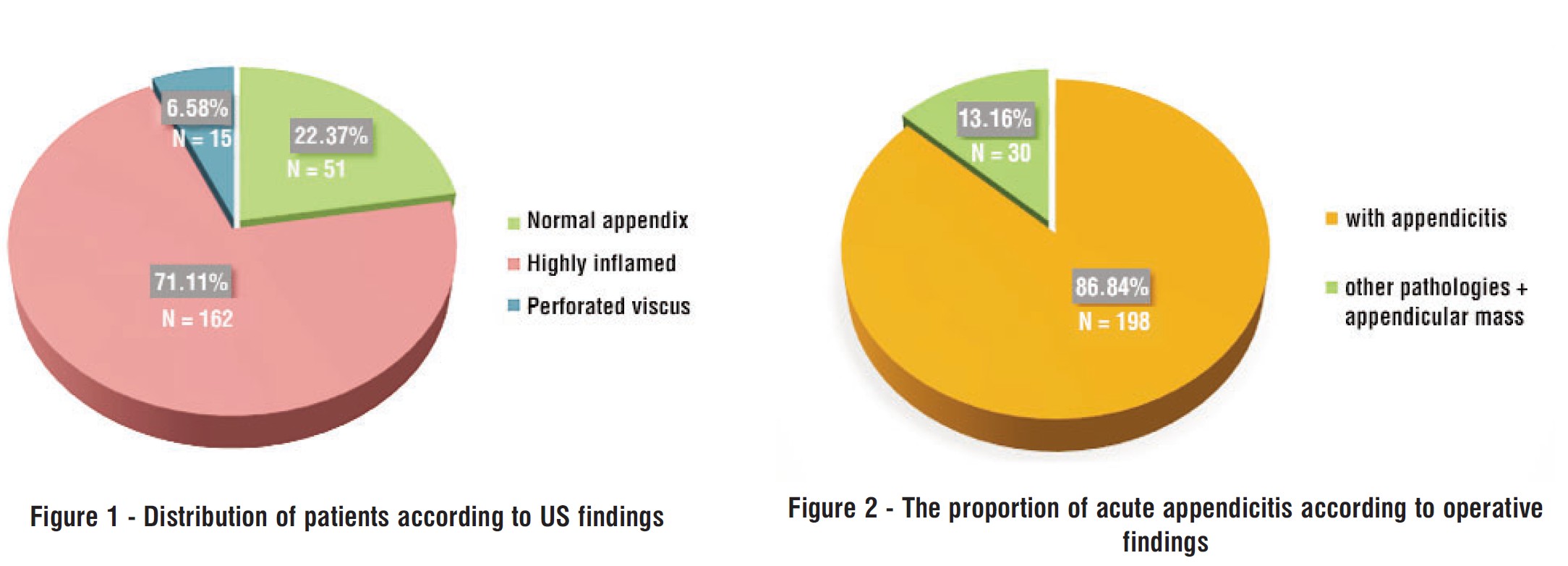
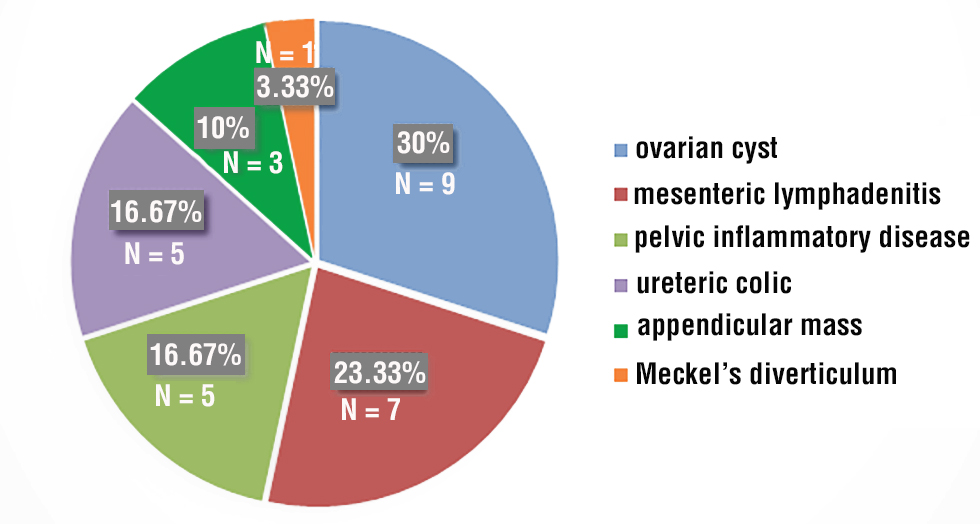
Figure 3 - Distribution of patients according to non-appendicitis pathologies
Final Diagnosis
According to operative findings, 198 patients (86.84%) were confirmed to have acute appendicitis, while 30 patients (13.16%) had other pathologies and appendicular mass (fig. 2).
Non-Appendicitis Pathologies
Out of 30 patients without appendicitis, 9 (30%) were found to have ovarian cysts, 7(23.33%) had mesenteric lymphadenitis, 5(16.67%) had pelvic inflammatory disease, 5 (16.67%) had uretric colic, 3(10%) had appendicular mass, and one patients (3.33%) had Meckel’s diverticulum (fig. 3).
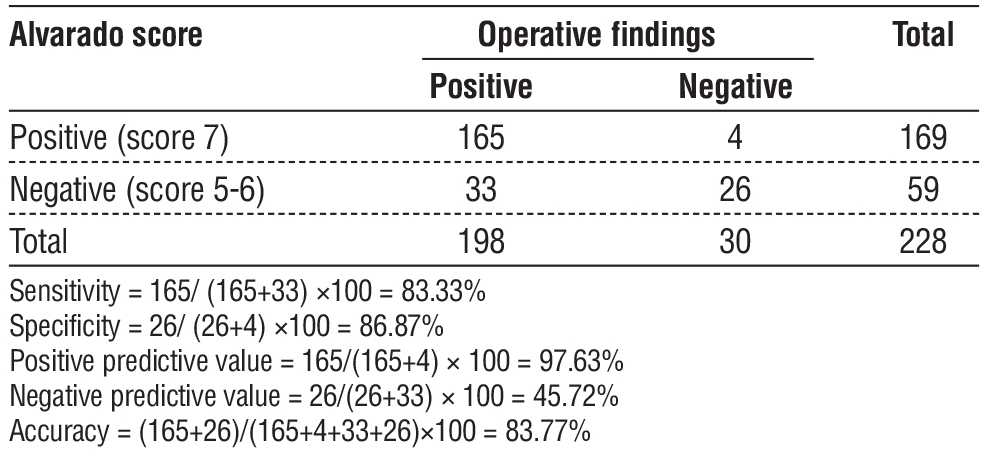
Table 3 - The overall diagnostic value of Alvarado score in detection of acute appendicitis
Diagnostic value of Alvarado Score
Overall diagnostic value
A total of 169 patients had Alvarado score ? 7 and were considered to have acute appendicitis. Among 198 patients confirmed to have acute appendicitis based on operative findings, 165 were also identified as positive for acute appendicitis using the Alvarado score. Conversely, of the 30 patients who were negative for acute appendicitis, 26 were similarly classified as negative by the Alvarado score. Accordingly, the sensitivity and specificity of Alvarado score in diagnosis of acute appendicitis will be 83.33% and 86.87%, respectively (table 3).
Table 4 - Diagnostic value of Alvarado score in detection of acute appendicitis in males
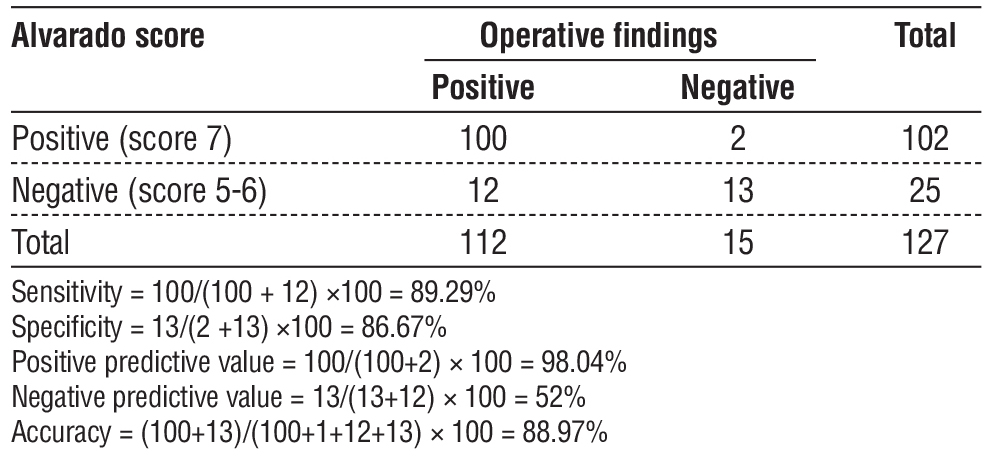
In male patients
The sensitivity and specificity of Alvarado score in diagnosis of acute appendicitis in males were 89.29% and 86.87%, respectively (table 4).
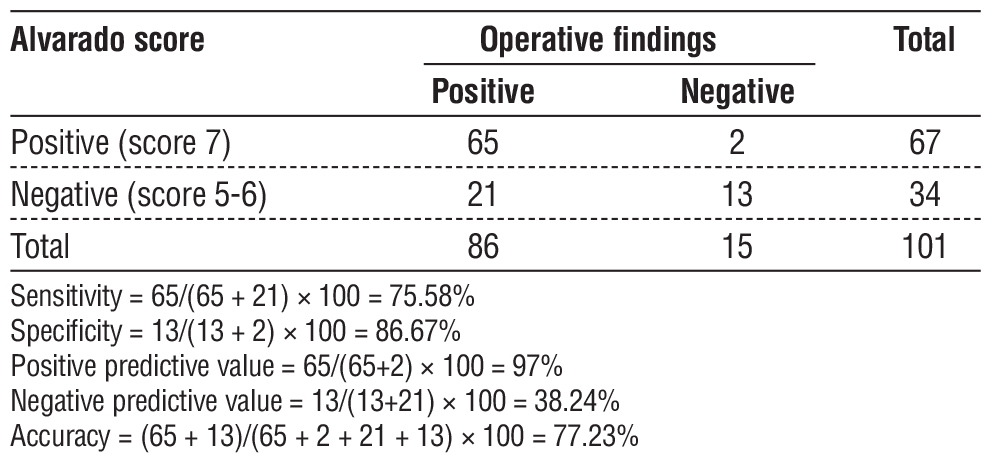
In female patients
the sensitivity and specificity of Alvarado score in diagnosis of acute appendicitis in males were 75.58% and 86.87%, respectively (table 5).
Table 5 - Diagnostic value of Alvarado score in detection of acute appendicitis in females
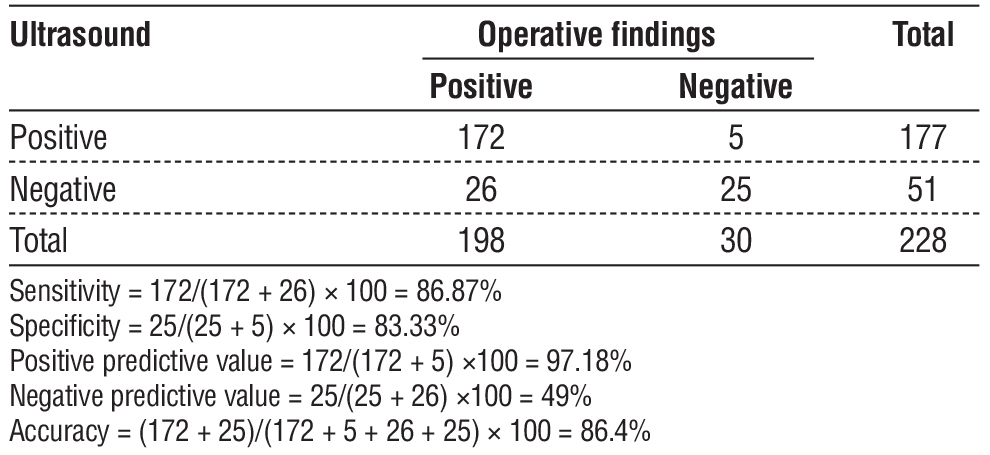
Diagnostic Value of Ultrasonography
According to US findings, 177 patients were found to have acute appendicitis. Of those, 172 patients were diagnosed operatively. Alternatively, 25 patients out of 30 had a negative result for acute appendicitis. As such, the sensitivity and specificity of US in diagnosis of acute appendicitis will be 86.87% and 83.33%, respectively (table 6).
Table 6 - Diagnostic value of ultrasound in detection of acute appendicitis
DISCUSSION
In spite of being the most common cause of acute abdomen, acute appendicitis remains a challenging diagnosis because it is basically a clinical diagnosis which has many clinical pictures. Thus, atypical cases present a diagnostic dilemma. Therefore, clinical diagnosis should be complemented with other diagnostic modalities. According to the result of the study, the mean age of the patients was 38.48 ± 13.46 years, with slight predominant of males over females (55.7% vs 44.3%). These results are in accordance with several pervious studies worldwide.
In an Iraqi study including, 400 patients acute appendicitis was more common in males (n=224, 56%) than females (n=176, 44%) with male to female ratio of 1.27:1. However, the highest rates of appendicitis was found in the age group of 10 to 19 years ( 39.5%) and the lowest was 50 and more (2.75%) (9). In an Egyptian study including 50 patients, acute Appendicitis existed more frequently in males than females (60% versus 40%). The age of patients ranged from 9 to 62 years, with the mean age was about 28 years old (10). Suboti´c et al. (11) in their study on 48 patients, 52,09% were males, and 23 (47,91%) were female.
Sex variation was attributed to the fact that female patients with right iliac fossa pain have a wide range of differential diagnoses. As a result, acute appendicitis may be over diagnosed in this gender group.
In the present study, US findings revealed highly inflamed in162 patients (71.11%,) and perforated viscus (6.58%). These findings suggest that most patients presented during the active inflammatory phase, while a smaller proportion had progressed to complicated appendicitis such as perforation. When compared with other studies, variability in sonographic findings has been reported, reflecting differences in the timing of presentation, disease progression, and patient characteristics. Al Awayshih et al. (12) included 100 Jordanian patients with acute appendicitis. The perforate viscus accounted for 4% of the patients which very close to the present study. Memon et al. (13) reported a perforation rate of 9.2% Kong et al. (14) studied 1000 patients (54% male, median age 21yrs.). Forty percent had inflamed, non-perforated appendices, and 60% had perforated appendices.
The relatively lower detection of perforation (6.58%) in the current study may indicate that most patients were diagnosed and treated before perforation occurred, or that subtle signs of perforation were difficult to visualize with ultrasound.
In the present study, the negative appendectomy rate was 13.16% which with the context of global rate which was rates reported in the literature of 8 to 33% (15). In an Iraqi a prospective study of 225 patients, the negative appendectomy rate was 27 cases (12.0%) (16). Moreover our results is are agreement with Nasiri S et al, when he reported that the negative finding were found in rates about (11%) of the patients included in their study (17).
A much higher rate of negative appendectomy was reported in a Pakistani study (28.7%) (13). Tekeli M et al, in his study found that the incidence of negative appendectomy was more than in our study (25.3 %) (18), while In Al Hashemy AM, revealed that the incidence rate of false positive appendectomy was 27.3% (19).
In contrast, a Moroccan study including 80 patients with acute appendicitis, negative appendectomy rate was 4.8% (44). Furthermore, Akhnokh et al. (10) demonstrated that thee negative appendectomy rate in the current study was 10% which are lower than ours.
In the present study, in patients with no acute appendicitis, ovarian cysts was reported in 9 patients, mesenteric lymphadenitis in 7 patients, pelvic inflammatory disease in 5 patients, uretric colic in 5 patients, appendicular mass in 3 patients, one patients had Meckel’s diverticulum. Almost similar findings were reported in the Pakistani study, where the right ovarian cysts was reported in 12.9%, mesenteric lymphadenitis in 9.6%, pelvic inflammatory disease in 9.6%, and right ureteric colic in 9.6% of the patients with non-appendicitis (13).
In the present study, the overall the sensitivity and specificity of Alvarado score in diagnosis of acute appendicitis will be 83.33% and 86.87%, respectively. the PPV and NPV were 97.63% and 45.72%, respectively. Furthermore, Alvarado score had higher sensitivity, PPV, NPV and accuracy in males (89.29%, 98.04%, 52% and 88.97%, respectively) than females (75.58%, 97%, 38.24% and 77.23%, respectively). These findings are in accordance with most previous international studies.
Gupta et al. (21) studied 50 Indian patients with acute appendicitis. The sensitivity of Alvarado score was 96.29%, specificity was 66.66%, and the positive predictive value was 92.85%, while in women group, the sensitivity was 81.8%, specificity was 66%, and positive predictive value was 81.8%.
In the study by Memon et al, the Alvarado scoring system exhibited high sensitivity and specificity at 93.5% and 80.6%, with PPV and NPV at 92.3% and 83.3%, respectively, and an accuracy of 89.8% (13). Kanumba et al (22) reported Alvarado score sensitivity, specificity, PPV, NPV, and accuracy of 94.1%, 90.4%, 95.2%, and 88.4%, respectively.
In a Moroccan stud, the sensitivity was 94.9%, the specificity was 72.7%, the positive predictive value was 98.4% and the negative predictive value was 44.4% (20). Additionally, the Alvarado score has been noted to overestimate the probability of appendicitis in females (23), and poorly identify complicated appendicitis in the elderly population (24).
However, in the Egyptian study reported much lower diagnostic value with an overall sensitivity of 68.9% (75% for male individuals and 58.8% for female individuals). Overall specificity was 40% (50% for male individuals and 33.3% for female individuals), PPV was 90.2%, and the negative predictive value was 11.1% (10). Furthermore, Al Awayshihet al. (12) reported a PPVof 89%. The sensitivity was 54% and specificity 75%. The authors concluded that Alvarado score is not a sensitive tool for aiding diagnosis of acute appendicitis.
The lower overall sensitivity of the score in females is expected. Premenopausal females have several gynecological conditions with presentations similar to appendicitis. The common misdiagnoses include pelvic inflammatory disease, gastroenteritis, urinary tract infection, ruptured ovarian follicle, and ectopic pregnancy. For their group of women with normal appendices who underwent an operation, alternative diagnoses included pelvic inflammatory disease, ruptured follicular cysts, twisted ovarian cysts, and ruptured ectopic pregnancy (25).
In the present study, US had a sensitivity, specificity, PPV, NPP and accuracy of 86.87%, 83.33%, 97.18%, 49% and 86.4%, respectively.
There is a notable variation in the sensitivity and specificity of abdominal US reported in the literature. For instance, Hosseini et al. (26) reported a sensitivity and specificity of 58% and 68%, respectively. Conversely, Abu-Yousef et al. (27) reported higher sensitivity (80%) and specificity (95%). A meta-analysis by Orr et al. (28) showed a sensitivity and specificity of 84.7% and 92.1%, respectively. The authors concluded that US should not be used to exclude appendicitis given the poor NPV. Conversely, a recent meta-analysis that included 21 studies reported a pooled sensitivity and specificity of 81% and 87%, respectively (29).
These findings, when taken together, might indicate methodological differences attributed to study settings and radiological expertise.
Study Limitations
This study has several limitations that should be acknowledged.
It was conducted at a single center, which
may limit the generalizability of the findings to broader populations.
The reliance on intraoperative findings without histopathological confirmation in all cases may introduce variability in defining true appendicitis, especially in atypical presentations.
CONCLUSIONS
The Alvarado score can be used effectively in our setup to reduce the incidence of negative appendectomies. It helps to make prompt decision in suspected cases. However, the negative predictive value was low (45.72%) in the 5–7 score group, limiting its reliability in excluding appendicitis in this range. Alvarado score has better sensitivity, PPV, NPV and accuracy in males than females. Future research with larger and multicenter cohorts is recommended to validate findings and enhance diagnostic protocol
Authors’ Contributions
Asawer Zain Al-Abideen Abdul-Razzaq: conceptuali-zation; data curation; investigation; methodology; project administration; resources; software; writing – original draft and writing – review & editing Alaa Jameel Hassan: conceptualization; data curation; investigation; methodology; project administration; writing – original draft and writing – review & editing.
Conflicts of Interest
The authors declare no conflict of interest regarding this article.
Funding: None.
Ethical Approval
The Medical Ethical Committee of The Department of surgery, College of Medicine, University of Thi-Qar approved this study (no. 15 on 8/10/2024).
REFERENCES
1. Kanumba ES, Mabula JB, Rambau P, Chalya PL. Modified Alvarado scoring system as a diagnostic tool for acute appendicitis at Bugando Medical Centre, Mwanza, Tanzania. BMC Surg. 2011;11:4.
2. Singh K, Gupta S, Parga P. Application of Alvarado scoring system in the diagnosis of acute appendicitis. JK Sci. 2008;10:84-86.
3. Yegane R, Peyvandi H, Hajinasrollah, Salehei N, Ahmadei M. Evaluation of modified Alvarado score in acute appendicitis among Iranian patients. Acta Medica Iranica. 2008;46:501-506.
4. Munir K, Iqbal J, Mushtaq U, Ishaque I, Mudassar J, Khalid A. Modified Alvarado scoring system in the diagnosis of acute appendicitis. APMC. 2008;2:91-94.
5. Khan I, Rehman AU. Application of Alvarado scoring system in diagnosis of acute appendicitis. J Ayub Med Coll Abbotabad. 2005; 17:41-44.
6. Limpawattanasiri C. Alvarado score for the acute appendicitis in a provincial hospital. J Med Assoc Thai. 2011;94:441-448.
7. Lotfollahzadeh S, Lopez RA, Deppen JG. Appendicitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan.
8. Sutton D, Robinson PJA, Jenkins JPR, Whitehouse R and WALLANP L(eds) Textbook of Radiology and Imaging 7th ed. Churchill Livingstone 2003; p. 680-83
9. Albahadili AM. Study of the effect of age, gender and seasonal variation on appendicitis in Azizyah-Iraq. Al-Kufa Univ J Biol. 2016; 8(2):55-62.
10. Akhnokh SG, Wahab RM, Kamel AS. Evaluation of Alvarado score in the diagnosis of acute appendicitis. Med. J. Cairo Univ. 2020;88(4): 1663-1672
11. Subotic AM, Sijacki AD, Dugalic VD, Antic AA, Vukovic GM, Vukojevic VS, et al. Evaluation of the Alvarado score in the diagnosis of acute appendicitis. Acta Chir Iugosl. 2008;55(1):55-61.
12. Awayshih MMA, Nofal MN, Yousef AJ. Evaluation of Alvarado score in diagnosing acute appendicitis. Pan Afr Med J. 2019;34:15.
13. Memon ZA, Irfan S, Fatima K, Iqbal MS, Sami W. Acute appendicitis: diagnostic accuracy of Alvarado scoring system. Asian J Surg. 2013;36(4):144-149.
14. Kong VY, van der Linde S, Aldous C, Handley JJ, Clarke DL. The accuracy of the Alvarado score in predicting acute appendicitis in the black South African population needs to be validated. Can J Surg. 2014;57(4):121–5.
15. Singh K, Gupta S, Parga P. Application of Alvarado scoring system in the diagnosis of acute appendicitis. JK Sci. 2008;10: 84-86.
16. Amiri MH, Abdulkhaliq MF. Correlation between Alvarado score and intra-operative findings in acute appendicitis. J Madenat Alelem College, 2021;13(1):319-326
17. Limpawattanasiri C. Alvarado score for the acute appendicitis in a provincial hospital. J Med Assoc Thai. 2011;94(4):441-9.
18. Tekeli MT, Ilhan E, Ureyen O, Senlikci A, Yeldan E, Ozturk M, et al. How much Reliable Is Alvarado Scoring System in Reducing Negative Appendectomy? Indian J Surg. 2017;79(2):106-110.
19. Al-Hashemy AM, Seleem MI. Appraisal of the modified Alvarado score for acute appendicitis in adults. Saudi Med J. 2004;25(9): 1229-31.
20. Bouali M, El Berni Y, Moufakkir A, El Bakouri A, El Hattabi K, Bensardi F, et al. Value of Alvarado scoring system in diagnosis of acute appendicitis. Ann Med Surg (Lond). 2022;77:103642.
21. Gupta M, Virdi VS, Agnihotri L, Mandial V. Evaluation of modified Alvarado score and ultrasonography for the diagnosis of acute appendicitis. Int J Sci Res. 2016;5(3):2166-8.
22. Kanumba ES, Mabula JB, Rambau P, Chalya PL. Modified Alvarado scoring system as a diagnostic tool for acute appendicitis at Bugando Medical Centre, Mwanza, Tanzania. BMC Surg. 2011;11(1):4
23. Al-Shuwayman AA, Aldawsari HF, Al-Shahri, SBS et al. Appendicitis: A medical serious condition - An updated review. Int J Health Scie. 2023;7(1):3624-3639
24. Deiters A, Drozd A, Parikh P, Markert R, Shim JK. Use of the Alvarado Score in Elderly Patients with Complicated and Uncomplicated Appendicitis. Am Surg. 2019;85(4):397-402.
25. Bhattacharjee PK, Chowdhury T, Roy D. Prospective evaluation of modified Alvarado score for diagnosis of acute appendicitis. J Indian Med Assoc. 2002;100(5):310-1.
26. Hosseini A, Omidian J, Nazarzadeh R. Investigating diagnostic value of ultrasonography in acute appendicitis. Adv Biomed Res. 2018;7(1):113.
27. Abu-Yousef MM, Bleicher JJ, Maher JW, Urdaneta LF, Franken EA, Metcalf AM. High-resolution sonography of acute appendicitis. AJR Am J Roentgenol. 1987;149(1):53–58.
28. Orr RK, Porter D, Hartman D. Ultrasonography to evaluate adults for appendicitis: decision making based on meta-analysis and probabilistic reasoning. Acad Emerg Med. 1995;2(7):644–650
29. Cho SU, Oh SK. Accuracy of ultrasound for the diagnosis of acute appendicitis in the emergency department: a systematic review. Medicine. 2023;102(13):e33397
Full Text Sources:
Abstract:
Views: 3061

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.