Surgery, Gastroenterology and Oncology

|
|
Calcified fibrous tumor (CFT), also known as calcified fibrous pseudotumor, is a rare benign mesenchymal lesion characterized by dense hyalinized fibrous tissue, lymphoplasmacytic inflammatory infiltrate, and distinctive calcifications. Although it can occur in various locations, the gastrointestinal tract is an increasingly recognized site. We present the case of a 29-year-old patient who developed intestinal obstruction. Imaging studies identified a calcified mesenteric lesion as the probable cause. An exploratory laparotomy was performed, revealing a mesenteric-dependent small bowel tumor, which was completely resected. Histopathology confirmed the diagnosis of calcified fibrous tumor. Intestinal obstruction is a rare clinical manifestation of this entity. Complete surgical resection is the treatment of choice and is usually curative. This case highlights the importance of considering CFT in the differential diagnosis of calcified mesenteric masses, especially when associated with obstructive symptoms.
INTRODUCTION
Calcified fibrous tumor (CFT), first described by Rosenthal and Abdul-Karim (1) and later named “calcified fibrous pseudotumor” by Fetsch et al. (2), is a rare benign mesenchymal lesion. Histologically, it is defined by a proliferation of spindle-shaped soft cells embedded in a densely hyalinized collagenous stroma, associated with a lymphoplasmacytic inflammatory infiltrate and the variable presence of dystrophic or psammomatous calcifications (3,4).
Although initially considered a deep soft tissue lesion, especially in children and young adults, its occurrence has been documented in a wide range of anatomical locations, such as the pleura, mediastinum, neck, and, increasingly, the gastrointestinal tract (stomach, small intestine, colon, appendix) and mesentery (5,6).
Clinically, gastrointestinal CFT are usually incidental findings. However, they can manifest symptoms such as abdominal pain, ulceration, bleeding, or, as in the present case, intussusception or intestinal obstruction (4,7). The definitive diagnosis is established by histopathological study, and complete surgical resection is usually the curative treatment (5,8).
The aim of this report is to present a case of intestinal obstruction secondary to a CFT located in the mesentery of the small intestine, a rare clinical manifestation, and to review the literature on the subject.
Figure 1 - Lateral abdominal X-ray showing air-fluid levels without significant dilation of the small intestine.

CASE REPORT
We present the case of a 29-year-old female patient from Sinaloa, Mexico, with no personal history of disease, occasional alcohol consumption, and no family history of cancer. She presented with abdominal pain that had been present for 24 hours, located in the mesogastrium, colicky in nature, with an intensity of 5/10 on the visual analog scale (VAS). The patient reported that she began self-medicating with NSAIDs (ketorolac), achieving partial improvement. However, the following day, the intensity of the pain increased to 10/10 and was associated with episodes of vomiting on seven occasions, which prompted her to present to the emergency department.
On physical examination, she was neurologically intact, without tachycardia, normotensive, afebrile, with hydrated mucous membranes, peristalsis present in the abdomen, without abdominal distension, and pain on deep palpation in the mesogastric region, without signs of peritoneal irritation.
Diagnostic studies were performed, including a lateral abdominal X-ray (April 10, 2025), which showed air-fluid levels without significant dilation of the intestinal loops (fig. 1). Subsequently, a plain abdominal computed tomography (CT) scan was performed, which identified a circumferential tumor lesion in the mesogastric region, presumably dependent on the mesentery, and containing heterogeneous material with areas of calcification inside (fig. 2). Given the suspicion of a mesenteric lesion, the patient was admitted for further diagnostic workup.
Figure 2 - Simple abdominal computed tomography. (a) Axial view, (b) Coronal view, and (c) Sagittal view. The blue arrow indicates a circumferential tumor lesion in the mesogastric region with internal calcifications.

During her hospital stay, the patient initially showed favorable progress, tolerating enteral feeding without nausea or vomiting. Antispasmodic treatment (butylhyoscine) was administered for pain control, adequate gas passage was maintained, and bowel movements were observed on the second day of hospitalization. A new abdominal-pelvic CT scan with contrast medium (04/11/2025) shows an oval lesion in the small intestine, with partially defined edges, heterogeneous density with areas of higher and lower density, and significant enhancement with the passage of contrast medium. A transition zone and dilation of the proximal intestinal loops are observed, as well as scant free fluid in the pelvic cavity (fig. 3).
Figure 3 - Contrast-enhanced abdominal computed tomography. (a) Axial view, (b) Coronal view, and (c) Sagittal view. The green arrow shows an oval lesion in the small intestine with significant enhancement, a transition zone, and dilation of the proximal loops.

On April 15, 2025, the patient presented a new episode of severe abdominal pain, accompanied by an inability to pass gas and absence of bowel movements. Due to the persistence of symptoms and imaging findings suggestive of a pseudo-obstructive process secondary to the tumor, the decision was made to proceed with an exploratory laparotomy.
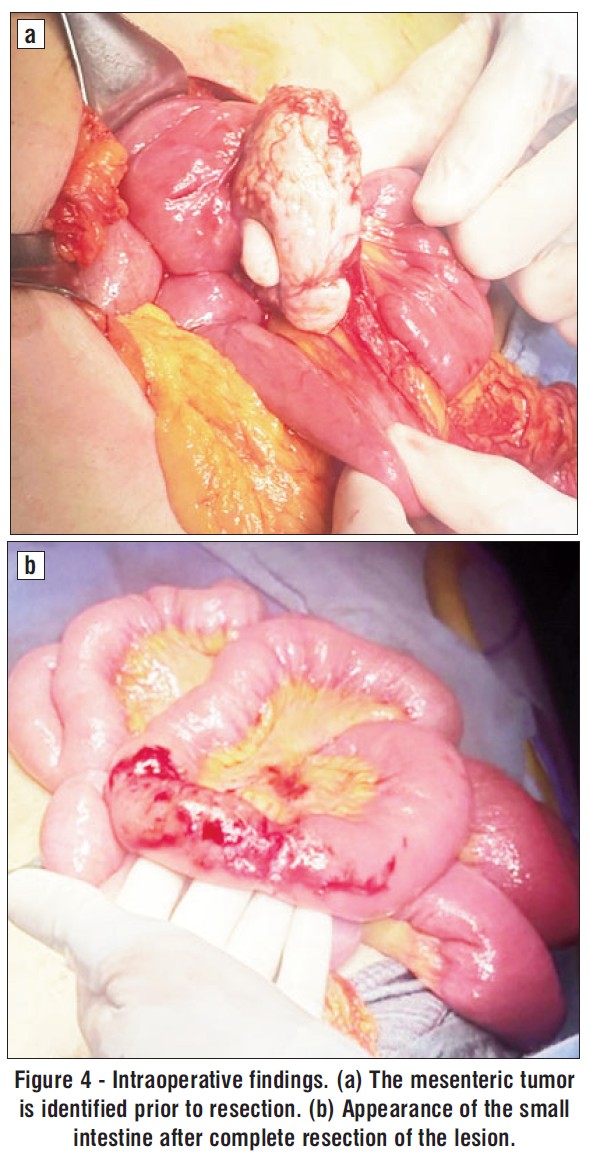
During the procedure, a mesenteric lesion of the small intestine was found, measuring 7 x 3 cm, with irregular edges, dense consistency, and whitish color. The lesion had a feeding vessel originating from the mesentery and was located 50 cm from the angle of Treitz, with loose adhesions to an intestinal loop 250 cm from the angle of Treitz. Complete resection of the tumor was achieved (fig. 4).
The surgical specimen was sent for histopathological diagnosis (fig. 5). Microscopic analysis revealed a hypocellular fibroblastic proliferation alternating with extensive chronic inflammatory infiltrate and areas of sclerosis. The myofibroblastic cells observed were spindle-shaped, with oval nuclei and elongated cytoplasm, without significant atypia. The inflammatory infiltrate consisted mainly of plasma cells, lymphocytes, and some histiocytes, with occasional formation of lymphoid aggregates. Numerous dystrophic and psammomatous calcifications were also identified. The final diagnosis was calcified fibrous tumor, with surgical margins free of lesion.
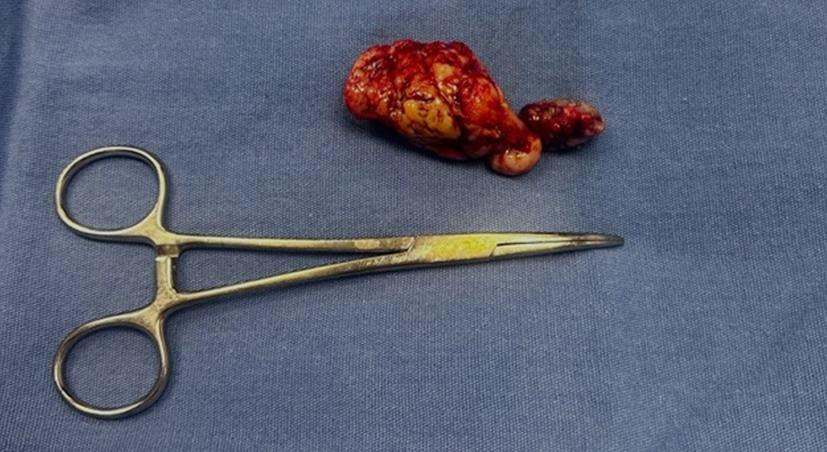
Figure 5 - Gross surgical specimen. The resected tumor measures 7 x 3 cm and presents a solid, fibrous, and multinodular appearance with a cerebriform surface.
After surgery, the patient had a favorable clinical outcome without complications. Four days after surgery, it was decided that she could be discharged home, with follow-up through outpatient consultations and a return to daily activities two weeks after surgery.
DISCUSSION
Calcified fibrous tumor (CFT) is a rare benign mesenchymal entity. Although it can arise in various locations, its presentation in the gastrointestinal tract or mesentery, as in this case, is increasingly recognized (5,6). The age of presentation occurs in three peaks: early childhood, mid-20s, and mid-30s. Our patient (29 years old) is within the reported range for adults (5). A slight female predisposition can be observed in CFTs, as in our case, although no explanation for this has been found to date (4).
Clinical presentation as intestinal obstruction, although uncommon, has been documented (7,8). The symptoms of CFTs are variable due to their hetero-geneous distribution of location. Thirty-five percent of cases present with various symptoms, characterized by being nonspecific, local, or systemic. Most are detected incidentally, and few present with local symptoms due to their mass effects (6). In our case, the mesenteric tumor caused an area of stenosis secondary to adhesion of the lesion with proximal dilation of the small intestine, which explains the patient's obstructive symptoms. The size of the tumor (7 x 3 cm) is within the variable range described in the literature, which ranges from small lesions to larger masses (4,5).
The histopathological findings reported for CFT in the literature are: paucicellular proliferation of spindle cells in a densely hyalinized collagenous stroma, accompanied by a chronic inflammatory infiltrate (predominantly lymphocytes and plasma cells) and the presence of psammomatous and dystrophic calcifications (4,7,10). The absence of significant cellular atypia and a low mitotic index are consistent with its benign nature.
The differential diagnosis of intra-abdominal GIST includes several mesenchymal entities. Gastro-intestinal stromal tumor (GIST) is more cellular, lacks the prominent hyalinization and calcifications of CFT, and is positive for CD117 and DOG-1 (4,8). Inflammatory myofibroblastic tumor (IMT) may be more cellular and present with atypia and ALK-1 positivity in a subset of cases (10,11). Other distinguishing features are solitary fibrous tumor (positive for CD34 and STAT6) and sclerosing mesenteritis (which infiltrates mesenteric fat and may lack prominent calcifications) (8,12). Immunohistochemistry is crucial; CFTs are usually positive for vimentin and variably positive for CD34 and factor XIIIa, while they are usually negative for c-kit (CD117), DOG-1, ALK-1, S100, and smooth muscle actin (4,9,10).
The pathogenesis of CFT remains unclear. It has been speculated that it may represent a final sclerosing stage of IMT (9,11) or be related to trauma or chronic inflammatory processes (12,13). Some studies suggest a possible association with IgG4-related disease, although this finding is not consistent (5,8). In our case, no specific traumatic or inflammatory history was identified that could explain its origin.
The treatment of choice for calcified fibrous tumors, regardless of their location, is complete surgical resection with clear margins (5,6,8,10). Given the benign nature of the lesion, adjuvant treatment such as chemotherapy or radiotherapy is not necessary.
In the case presented, an exploratory laparotomy was performed with complete resection of the mesenteric tumor. This approach allowed not only the removal of the lesion but also the resolution of the occlusive condition. Postoperative management included analgesia and antibiotic therapy, which are standard for this type of surgery.
The prognosis for CFT is excellent after complete surgical resection, with a low risk of recurrence (5,6).
The favorable outcome and absence of postoperative complications, followed by early hospital discharge, highlight the efficacy and safety of surgical treatment for this condition. Long-term follow-up is important to detect recurrences, although these are rare (5,6).
CONCLUSION
Calcified fibrous tumor is a rare benign mesenchymal lesion that can occur in the mesentery of the small intestine and cause intestinal obstruction. Diagnosis is based on characteristic histopathological findings, including hyalinized fibrous tissue, lymphoplasmacytic infiltrate, and calcifications. Complete surgical resection is the treatment of choice and offers an excellent prognosis with a low risk of recurrence. Considering CFT in the differential diagnosis of calcified mesenteric lesions is essential for appropriate management and to avoid unnecessarily aggressive treatments.
Acknowledgements
The authors express their gratitude to the Instituto Mexicano del Seguro Social for permitting access to facilities during this research.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
REFERENCES
1. Rosenthal NS, Abdul-Karim FW. Childhood fibrous tumor with psammoma bodies. Clinicopathologic features in two cases. Arch Pathol Lab Med. 1988;112(8):798-800.
2. Fetsch JF, Montgomery EA, Meis JM. Calcifying fibrous pseudotumor. Am J Surg Pathol. 1993;17(5):502-8.
3. Nascimento AF, Ruiz R, Hornick JL, Fletcher CD. Calcifying fibrous 'pseudotumor': clinicopathologic study of 15 cases and analysis of its relationship to inflammatory myofibroblastic tumor. Int J Surg Pathol. 2002;10(3):189-96.
4. Turbiville D, Zhang X. Calcifying fibrous tumor of the gastrointestinal tract: A clinicopathologic review and update. World J Gastroenterol. 2020;26(37):5597-5605.
5. Chorti A, Papavramidis TS, Michalopoulos A. Calcifying Fibrous Tumor: Review of 157 Patients Reported in International Literature. Medicine (Baltimore). 2016;95(20):e3690.
6. Zhou J, Zhou L, Wu S, Li R, Yang X, Xu H, et al. Clinicopathologic Study of Calcifying Fibrous Tumor Emphasizing Different Anatomical Distribution and Favorable Prognosis. Biomed Res Int. 2019;2019: 5026860.
7. Dwivedi D, Inturi R, Jayakar S, Nichkaode P. Calcified Fibrous Tumor of Jejunum: A Rare Case Report. Cureus. 2023;15(4):e38230.
8. Ben-Izhak O, Itin L, Feuchtwanger Z, Lifschitz-Mercer B, Czernobilsky B. Calcifying fibrous pseudotumor of mesentery presenting with acute peritonitis. Case report with immunohistochemical study and review of literature. Int J Surg Pathol. 2001;9(3):249-53.
9. Pezhouh MK, Rezaei MK, Shabihkhani M, Ghosh A, Belchis D, Montgomery EA, Voltaggio L. Clinicopathologic study of calcifying fibrous tumor of the gastrointestinal tract: a case series. Hum Pathol. 2017;62:199-205.
10. Hill KA, Gonzalez-Crussi F, Chou PM. Calcifying fibrous pseudo-tumor versus inflammatory myofibroblastic tumor: a histological and immunohistochemical comparison. Mod Pathol. 2001;14(8): 784-90.
11. Sigel JE, Smith TA, Reith JD, Goldblum JR. Immunohistochemical analysis of anaplastic lymphoma kinase expression in deep soft tissue calcifying fibrous pseudotumor: evidence of a late sclerosing stage of inflammatory myofibroblastic tumor? Ann Diagn Pathol. 2001;5(1):10-14.
12. Prucker J, Salaheddin-Nassr Y, Leidl S. Calcifying fibrous tumor of the terminal ileum mesentery: Case report. Medicine (Baltimore). 2018;97(51):e13351.
13. Marbaniang E, Khonglah Y, Dey B, Shunyu B, Gogoi B. Castleman's disease associated with calcifying fibrous tumor: A rare association with review of literature. J Lab Physicians. 2019;11(2):171-173.
Full Text Sources:
Abstract:
Views: 899

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.