Surgery, Gastroenterology and Oncology
|
|
Background: Hereditary factors play a major role in breast cancer development, making it a serious global health concern for women. This study aimed to determine if RAD51 gene polymorphism rs1801320 (135 G>C) increases breast cancer risk in women in Thi-Qar Province, Iraq.
Methods: Forty women with breast cancer and twenty healthy volunteers participated. Data from blood samples were analyzed using Chi-square tests and odds ratios for PCR-based genotyping.
Results: The RAD51 gene variant rs1801320 did not show a significant association with breast cancer risk in this group. Larger studies are needed to confirm these findings.
Conclusion: Both patients and controls commonly had the GG genotype. The GC and CC genotypes did not show a significant risk difference. Allele frequencies were also similar between groups.
Introduction
Breast cancer is a prevalent and serious malignancy among women worldwide. Epidemiological data show that about one in eight women may develop breast cancer in her lifetime (1). Early diagnosis improves treatment effectiveness and survival rates. In contrast, late detection allows malignancy to spread and increases mortality. Women diagnosed early have higher survival rates than those diagnosed later (2). RAD51, a conserved recombinase protein, is essential for homologous recombination (HR), which maintains genomic stability in breast, ovarian, and prostate tissues. Along with its paralogs—RAD51B, RAD51C, RAD51D, XRCC2, and XRCC3—RAD51 forms nucleoprotein filaments on single-stranded DNA, which facilitates the recognition of homologous sequences and the initiation of strand invasion, a key step in repairing DNA double-strand breaks (3–6). In addition to its central function in DNA repair, RAD51 also helps protect cells from oxidative stress, a major contributor to genomic instability in cancer (7). These roles suggest that RAD51 may be involved in cancer cell resistance to therapeutic inhibitors, making it a promising target for studies on treatment resistance and a potential biomarker for predicting response in breast cancer (8).
Research Gap
Results from the many studies that have looked at the link between RAD51 gene polymorphisms and the risk of breast cancer have been mixed at best. Furthermore, there is a dearth of studies that examine this correlation among Iraqi women, specifically in the Thi-Qar region. No studies have examined the possible use of RAD51 polymorphisms in this particular setting as biomarkers for early identification or predictors of therapy response.
Materials and methods
Samples Collection
Researchers in Thi-Qar Province took 40 blood samples from women who had been diagnosed with breast cancer at the Oncology Center at Al-Habboubi Hospital. These samples were taken from the same set of patients. Also, 20 women who were considered to be in good health had their blood drawn to serve as a control group. Patients and healthy persons were each given 4 ml of venous blood, which was then preserved at -20 °C in tubes that contained EDTA, an anticoagulant.
Statistical Analysis
Statistical analysis was performed using Chi-square, T-test, and ANOVA, with significance set at p < 0.05. Odds ratios were calculated for genotype distribution. All analyses used SPSS software (9).
Results
The Effect of Smoking
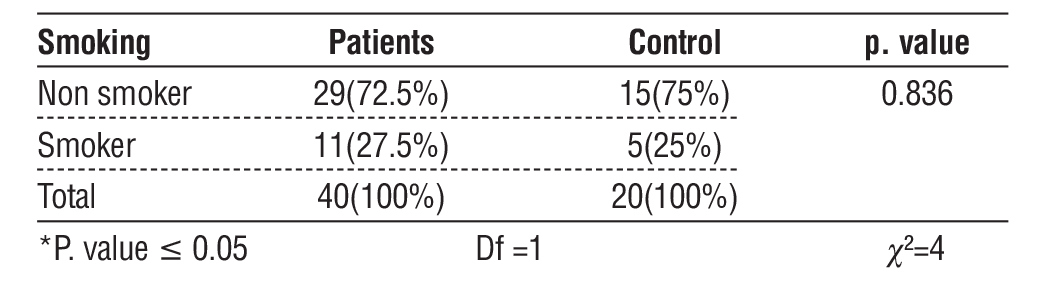
The patient and control groups were stratified based on smoking status. Among the breast cancer patients, 27.5% were smokers, while 72.5% were non-smokers. A similar distribution was observed in the control group, with 25% smokers and 75% non smokers. When comparing the patient and control groups according to their smoking status, no statistically significant differences were observed (p = 0.836).
The Effect of Age
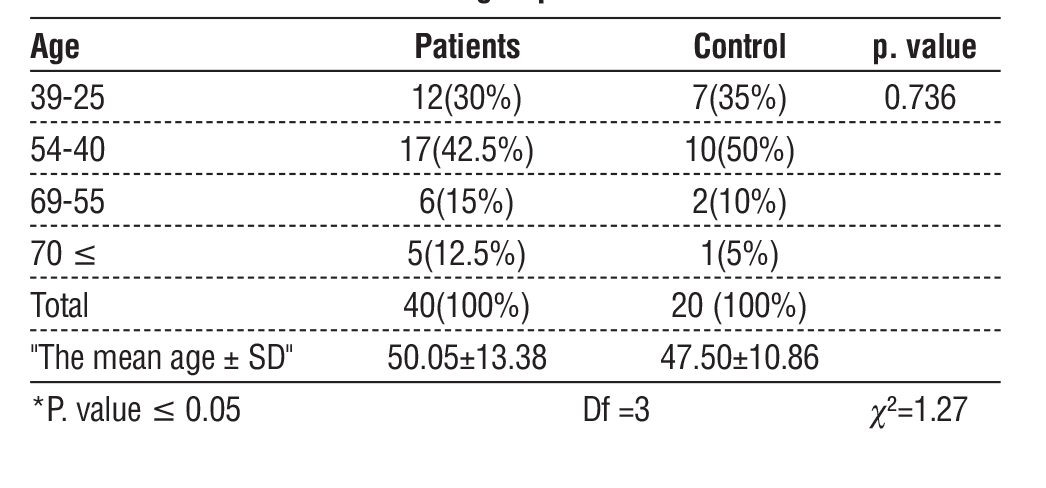
At a significance level of p < 0.05, the present investigation did not find any statistically significant differences between the control and patient groups. People in the age bracket of 40-54 made up the largest percentage of both the sick group (42.5%) and the control group (50%). Among the age groups studied, 30% were patients and 35% were controls in the 25–39 age bracket, while 15% were patients and 10% were controls in the 55–69 age bracket. The lowest proportion of participants was in the >70 years category (12.5% of patients versus 5% of controls). Furthermore, the mean age of breast cancer patients was 50.05 ± 13.38 years, slightly higher than that of the control group (47.50 ± 10.86 years).
RAD51 gene polymorphism rs1801320 (135 G>C)
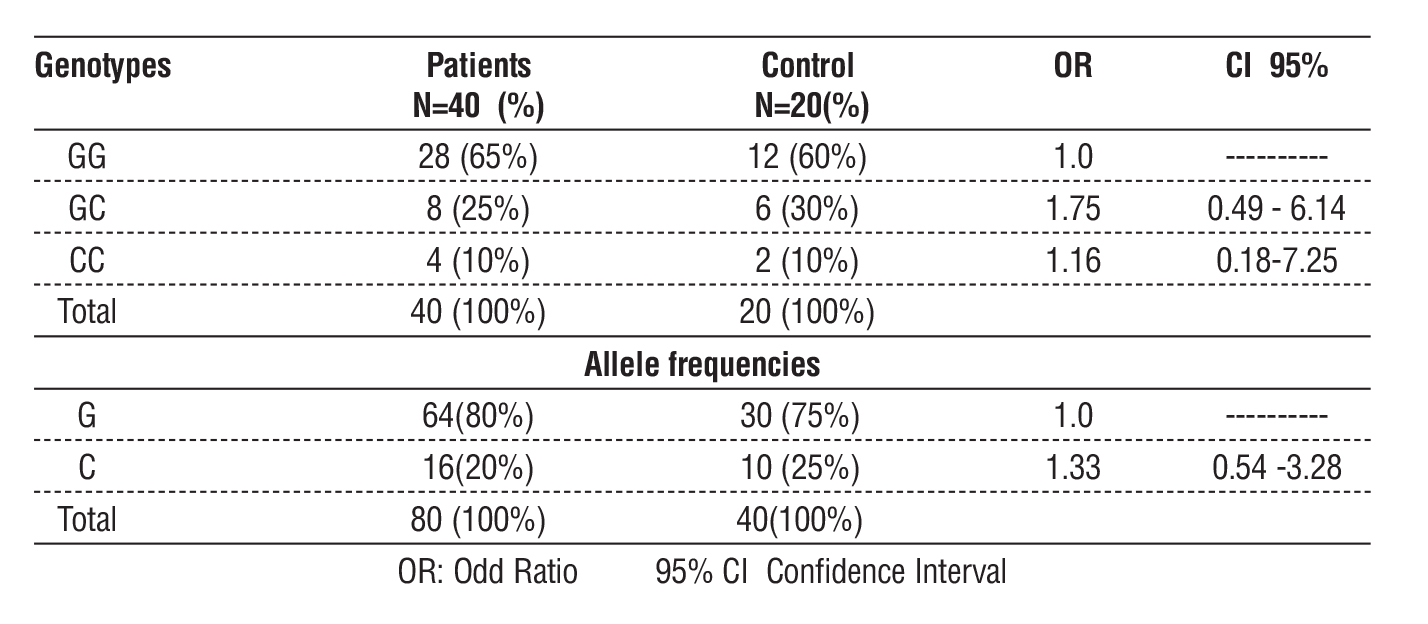
With 65% of patients and 60% of the control group carrying the GG genotype, it was determined to be the most frequent in the current research. With a lower frequency of 25% in patients and 30% in controls, the heterozygous genotype GC had an odds ratio of 1.75 compared to the reference genotype GG (OR = 1.75, 95% CI = 0.49-6.14). The homozygous genotype CC was the least common, observed in 10% of both patients and controls, with no significant risk of disease when compared to the reference GG genotype (OR = 1.16, 95% CI = 0.18–7.25).
Table 1 - Distribution of patients and healthy individuals according to smoking status
Regarding allele frequencies, the G allele was more prevalent among patients (80%) compared to the control group (60%). In contrast, the C allele was lower in patients (20%) than in controls (25%), with no significant risk observed when compared to the reference G allele (OR = 1.33, 95% CI = 0.54–3.28).
Discussion
In line with previous research that found no statistically significant increase in risk among smokers, the current investigation found no association between smoking and breast cancer (table 1) (10). In contrast, more recent research, such as that by (11), suggests that the effect of smoking may vary depending on menopausal status, with premenopausal smoking - particularly when started after age 18 or continued for 30 years or more - being linked to a higher risk of breast cancer. Furthermore, analysis of our current data (table 2) indicates that breast cancer is most prevalent in middle-aged women, which corresponds with several international reports identifying this age range as the period of peak disease incidence, for instance, (12) reported that the highest propor tion of breast cancer cases occurred in the 40-49 age group (27.6%), highlighting midlife as the peak period of incidence. However, in the present study, the peak age range was broader, covering the 40-54 age group, which accounted for 42.5% of cases, followed by the 25-39 age group at 30%. In contrast, an Omani study showed that the next highest proportion of cases was observed in the 50-59 age group, repre senting 25.3%.
Table 2 - Age distribution of breast cancer patients and the control group
Although the GC genotype was not linked to an elevated risk of breast cancer, the current findings were consistent with those of the most recent research by (13) in that the GG genotype was the most prevalent. When comparing GG and CC carriers for breast cancer risk, the two studies found different results. CC carriers were shown to have a much higher risk. At the allelic level, in the present study (table 3), the G allele was more frequent in both patients (80%) and controls (60%), whereas the C allele was less frequent in patients (20%) compared with controls (25%), with no increased risk when compared with the reference G allele. Both investigations agreed that the G allele was the most prevalent and was deemed the reference allele, however the C allele was found to be related with a higher risk of breast cancer (OR = 1.37, 95% CI = 1.04-1.80) in instead (13).
Table 3 - Distribution of genotypes and allele frequencies of the RAD51 gene among patient and control groups
Other studies have shown a high association between this polymorphism and breast cancer susceptibility, however they have reported inconsistent results. An elevated risk of breast cancer was shown to be substantially linked with the GC genotype, as shown in (14) (OR = 1.72, 95% CI = 1.13-2.62, p = 0.012). In addition, there was a statistically significant association between the risk of breast cancer and the combination of the GC and CC gene types (OR = 1.70, 95% CI = 1.14-2.53, p = 0.009). Additionally, carriers of the GC + CC geno types were found to have larger tumor sizes, and tumor aggressiveness was associated with RAD51 rs1801320 polymorphism, as patients with grade III tumors were more likely to carry the GC + CC geno types compared with those with grade I tumors.
Conclusion
This research found no statistically significant link between the rs1801320 (135 G>C) RAD51 gene polymorphism and breast cancer risk in the population that was investigated. Patients and controls alike were more likely to have the GG genotype, but those with the GC or CC genotypes were not at significantly higher risk of illness. Furthermore, the allele frequencies of the two groups did not vary significantly from one another. Although the middle-aged women had the greatest incidence of breast cancer, neither smoking status nor age had a statistically significant influence on the risk of the disease. These results raise concerns that this polymorphism could not be a standalone risk factor for breast cancer; thus, additional research with bigger and more varied populations is needed to confirm these findings.
Conflict of Interest
Authors declared no any conflict.
Funding
The University of Thi Qar College of Education of Pure Science in Iraq provided financial support for this research.
Ethical Statement
Approved by IRB of Thi-Qar University (no. 55 in 2022).
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33.
3. Park JY, Singh TR, Nassar N, Zhang F, Freund M, Hanenberg H, et al. Breast cancer-associated missense mutants of the PALB2 WD40 domain, which directly binds RAD51C, RAD51 and BRCA2, disrupt DNA repair. Oncogene. 2014;33:4803–12.
4. Lang SH, Swift SL, White H, Misso K, Kleijnen J, Quek RG. A systematic review of the prevalence of DNA damage response gene mutations in prostate cancer. Int J Oncol. 2019;55:597–616.
5. Foo TK, Xia B. BRCA1-dependent and independent recruitment of PALB2-BRCA2-RAD51 in the DNA damage response and cancer. Cancer Res. 2022;82:3191–7.
6. Bonilla B, Hengel SR, Grundy MK, Bernstein KA. RAD51 gene family structure and function. Annu Rev Genet. 2020;54:25–46.
7. Wang Z, Jia R, Wang L, Yang Q, Hu X, Fu Q, et al. The emerging roles of RAD51 in cancer and its potential as a therapeutic target. Front Oncol. 2022;12:935593.
8. Zhao Q, Guan J, Zhang Z, Lv J, Wang Y, Liu L, et al. Inhibition of Rad51 sensitizes breast cancer cells with wild-type PTEN to olaparib. Biomed Pharmacother. 2017;94:165–8.
9. Okab HF, Salih MB, Jarulla BA. Evaluation of CXCL 10 and IL-10 in COVID-19 pneumonia. Pneumologia. 2024;71(4):175–80
10. White AJ, D’Aloisio AA, Nichols HB, DeRoo LA, Sandler DP. Breast cancer and exposure to tobacco smoke during potential windows of susceptibility. Cancer Causes Control. 2017;28(7):667–75.
11. Peñalver-Argüeso B, García-Esquinas E, Castelló A, Fernández de Larrea-Baz N, Castaño-Vinyals G, Fernández-Villa T, et al. Smoking history and breast cancer risk by pathological subtype: MCC–Spain study. Tob Induc Dis. 2023;21:157.
12. Mehdi I, Abdul Monem E, Al Bahrani BJ, Al Kharusi S, Nada AM, Al Lawati J, et al. Age at diagnosis of female breast cancer in Oman: issues and implications. South Asian J Cancer. 2014;3(2): 101–6.
13. Ullah Khan N, Alqarni SS, Yousuf A, Shehzad I, Khan W, Gu W, Chen T. The influence of RAD51 (rs1801320) on breast cancer risk: an updated meta-analysis. Discov Oncol. 2025;16:289.
14. Parvin S, Islam MS, Al-Mamun MMA, Islam MS, Ahmed MU, Kabir ER, Hasnat A. Association of BRCA1, BRCA2, RAD51, and HER2 gene polymorphisms with the breast cancer risk in the Bangladeshi population. Breast Cancer. 2017;24(2):229-37.
Full Text Sources:
Abstract:
Views: 221

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.