Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
Is Abdominal Drain Necessary after Laparoscopic Appendectomy for Complicated Appendicitis?
Background: Laparoscopic appendectomy is a safe and effective procedure for acute
appendicitis. But several researchers found that performing laparoscopic appendectomy for
complicated appendicitis may carry a risk of postoperative intraabdominal abscess development,
and that’s why some surgeons use the intraabdominal drain. In our study we aimed to
assess the effect of the drain in laparoscopic appendectomy for complicated appendicitis.
Methodology: This is a prospective comparative study which was performed at Ain Shams University Hospitals between September 2018 and September 2021. It included 80 patients who underwent laparoscopic appendectomy for complicated appendicitis. The patients were divided sequentially into two groups, Group A: drain group and Group B: no-drain group.
Results: We had a non-significant difference between group A and B regarding postoperative complication (37.5% versus 32.5% respectively) and postoperative intraabdominal abscess formation (15% versus 12.5%) respectively). The no-drain group showed significantly shorter hospital stay than the drain group. We had no mortality in our study.
Conclusion: In our study, we didn’t find considerable benefits for using the drain over intraperitoneal irrigation and lavage without drain after laparoscopic appendectomy for complicated appendicitis with significant longer hospital stay in the drain group.
INTRODUCTION
Acute appendicitis is the most common surgical cause of acute abdomen that requires surgical intervention for its management with lifetime risk of 7-8% (1,2). The incidence of complicated acute appendicitis ranges from 20% to 30% of all appendicitis patients (3). Complicated acute appendicitis includes perforated appendix, gangrenous appendicitis, intraabdominal abscess, and generalized peritonitis (4).
While uncomplicated acute appendicitis can be safely managed with low postoperative complication, complicated acute appendicitis is still associated with significant postoperative morbidity (5-7). Postoperative complications can occur in up to 0.8-1.7% of the patients with uncomplicated appendicitis, while in complicated appendicitis postoperative complications can occur in 14-18% of patients, especially postoperative development of intraabdominal abscess (8,9) Laparoscopic appendectomy is considered now to be the preferable surgical approach for acute appendicitis with better cosmesis, less postoperative pain, lower incidence of surgical site infection, faster recovery, and better postoperative quality of life in comparison to open approach (10-12).
But on the other side, laparoscopy in complicated appendicitis may be a predisposing factor for higher incidence of postoperative abscess formation because pneumoperitoneum mostly opens the intrabdominal spaces (13).
However, when it comes to the management of complicated appendicitis either open or laparoscopic, surgeons debate about the use of some intraoperative techniques as the irrigation or the use of intraabdominal drain (14). The later had long history with conflicting viewpoints, Wiliam Halsted stated, "No drainage at all is better than the ignorant employment of it" (15) while Robert Tait was against Halsted's opinion as he stated, “When in doubt drain!” (16). Placement of abdominal drain after different types of surgeries is still controversial, it was assumed that the drains help in prevention of collection of infected fluids and in early detection of bleeding and leakage, but this is questionable now (5). Recently, it was proved that the use of intraabdominal drains in liver and colorectal surgery are not always beneficial but may even be harmful. So, there is an evolving trend towards fast-track surgery without using of intraabdominal drain in different types of abdominal surgeries (17). We aimed in this study to evaluate the effect of abdominal drain placement after laparoscopic appendectomy for complicated acute appendicitis on the incidence of postoperative morbidities.
PATIENTS AND METHODS
This study was a prospective comparative study which was performed at Ain Shams University Hospitals between September 2018 and September 2021. It included 80 patients who underwent laparoscopic appendectomy for complicated appendicitis. All cases were operated by the same surgical team.
Ethical considerations
The study got approval from the ethical committee of general surgery department and a written informed consent was taken from all participants after receiving an explanation of the study.
Eligibility criteria for the study
The study included cases of complicated appendicitis defined as perforated appendix, gangrenous appendix and presence of pus or peri-appendicular abscess by preoperative pelviabdominal ultrasound (US) and confirmed by diagnostic laparoscopy (fig. 1). Patients presented with uncomplicated acute appendicitis or appendicular mass, aged < 14 years, unfit to pneumoperitoneum or converted to open were excluded from this study. Also, we excluded cases with intraoperative acute haemorrhage warranting drain applying. Then the included cases were divided sequentially into two groups, 40 patients in each, Group A in which an abdominal drain was used and Group B in which no drain was left in the abdomen with just irrigation and lavage with normal saline.

Preoperative workup
Detailed history, general and abdominal examination were done for all patients. Full blood tests including inflammatory markers and US were done. Pelviabdominal computerized tomography (CT) with contrast was done if doubtful diagnosis or for patients ? 50 years old. Diagnosis of acute appendicitis was stablished by clinical diagnosis and confirmed by image and if still doubtful, diagnosis by laparoscopy was done.
Surgical management (fig. 2)
All patients received intra-venous (IV) ceftriaxone 2 gm and metronidazole 500 mg at induction of anaesthesia. Left subcostal insertion of veress needle was done to establish the pneumoperitoneum then introducing a visiport trocar (5-12 mm) at the umbilicus, with 2 other trocars placed at suprapubic (10 mm) and left iliac fossa (5 mm).
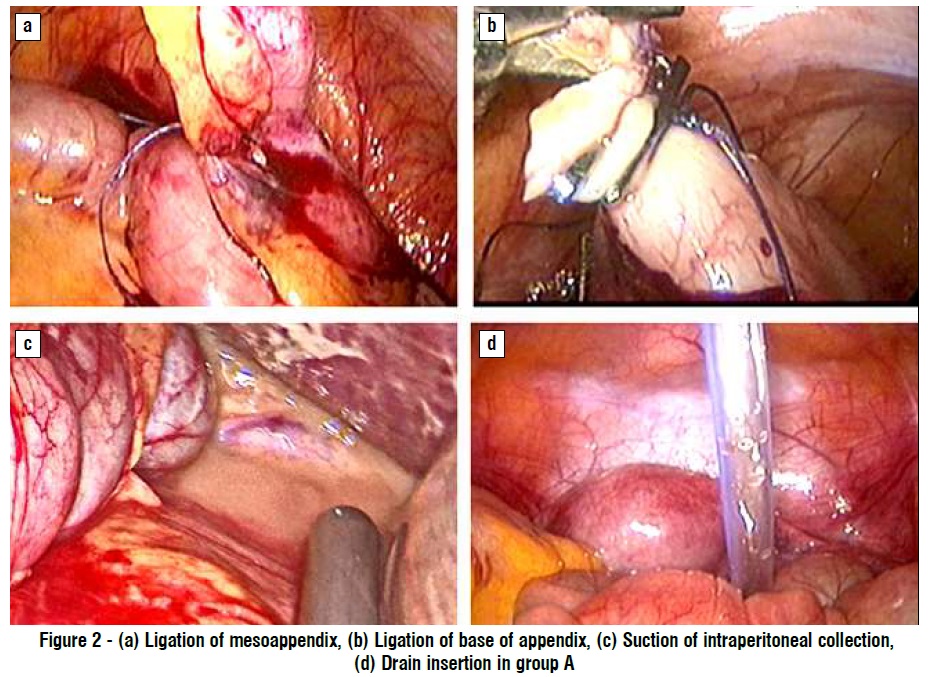
The procedure started with checking the site of veress needle, diagnostic laparoscopy was performed to identify the appendix and to confirm presence of complicated appendicitis as perforated appendix, gangrenous appendix and presence of pus or peri-appendicular abscess. The mesoappendix was ligated with 2/0 vicryl (Ethicon) suture then dissected using the electrocautery, the appendicular base was secured with 2/0 vicryl® (Ethicon) intracorporeal sutures and titanium clips. The specimen was removed through 10 mm port. Intraperitoneal lavage using saline 0.9% was done at the end of the operation. In group A, a tube drain was placed in the pelvic cavity.
Postoperative management
Follow up of the drain output and vital data was done together with parenteral administration of third generation cephalosporin and metronidazole. The drain was removed once the output was less than 50 ml/day of clear fluid. Patients started oral fluids intake once bowel sounds were audible and were discharged from hospital when oral intake was tolerated. Routine ultrasound was done for all patients to exclude postoperative collection either at the 5th postoperative day if the patient was not suspected clinically or at any time if the patient was suspected clinically by persistent fever, peritonitis and/or ileus. Follow up of the cases were planned at 10th and 21st postoperative days.
Data collection and surgical outcome
The patients demographic data and comorbidities in both groups were collected and compared. Both groups were compared as regard the following outcomes: - Primary outcome was the development of postoperative intraabdominal abscess or intraabdominal fluid collection (detected by US).
- Secondary outcomes were duration of operation, the length of hospital stay, other postoperative complications (atelectasis, wound infection, pneumonia, and ileus). we relied on Clavien- Dindo system (18) for the classification of surgical and non-surgical postoperative complications.
Data management and analysis
Data were revised, coded, entered on a computer and analysed using SPSS package version number 26. Student t-test was used for comparing quantitative variables between the two study groups. Chi-square and Fisher exact tests were used to test the association between qualitative variables. P-value ? 0.05 was considered significant and P-value ? 0.001 was considered highly significant.
RESULTS
Our study included 80 cases of laparoscopic appendectomy for complicated appendicitis. Patients were divided into two groups (40 patients in each), Group A (drain group) and Group B (no-drain group). There was a non-significant statistical difference in two groups regarding the demographics of the patients, comorbidities and preoperative investigations data as shown in table 1.
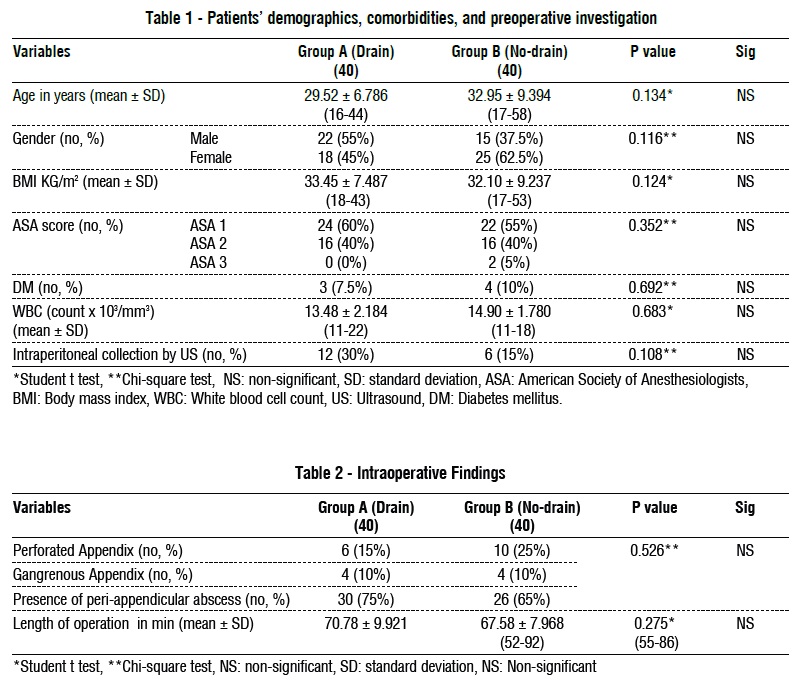
In our study, there was a non-significant difference between the two groups as regard length of operation and intraoperative finding of appendix as shown in table 2. We had no intraoperative morbidities in both groups.
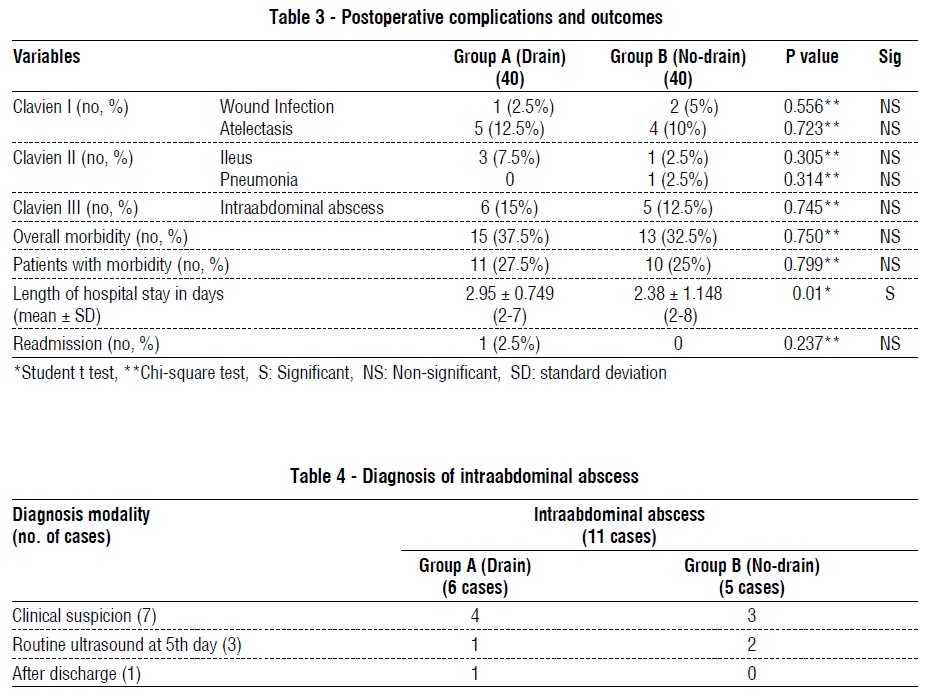
Postoperative pain was controlled by non-steroidal anti-inflammatory drugs and paracetamol in all cases with no need to opioids. In the analysis of the postoperative morbidity (whatever minor or major depending on Clavien-Dindo system), we had a nonsignificant statistical difference between the two groups (37.5% in group A versus 32.5% in group B). Major complications (Clavien III, postoperative intraabdominal abscess) were recorded in 6 cases (15%) in group A versus 5 cases (12.5%) in group B, with nonsignificant statistical difference between both. The no-drain group showed significantly shorter hospital stay than the drain group (2.38 days versus 2.95 days respectively) (table 3). There were no mortality cases or Clavien IV complications in either group.
Cases with postoperative wound infection were managed by antibiotics and bed side dressing, with no need for operative management, while cases with postoperative ileus required the insertion of naso-gastric tube in 2 patients, one in each group. The only case with post appendectomy pneumonia was managed with IV antibiotics and chest physiotherapy, but the patient required more than one week to be discharged from the hospital.
Of all cases with intraabdominal collection in both groups (11 cases), 4 patients were diabetic (two in each group), 7 patients were discovered by clinical suspicion (persistent abdominal pain and fever) in the postoperative course before the routine pelvi-abdominal ultrasound. Ultrasound was done and confirmed the diagnosis of intraabdominal collection. Another 3 cases were accidently discovered without any clinical suspicion on the 5th postoperative day with the routine pelvi-abdominal ultrasound. One case was discovered one week after discharge (10 days after the appendectomy) as the case presented with server abdominal pain and high-grade fever (table 4).
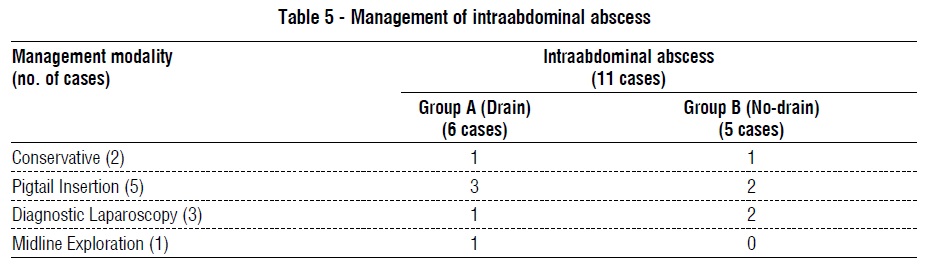
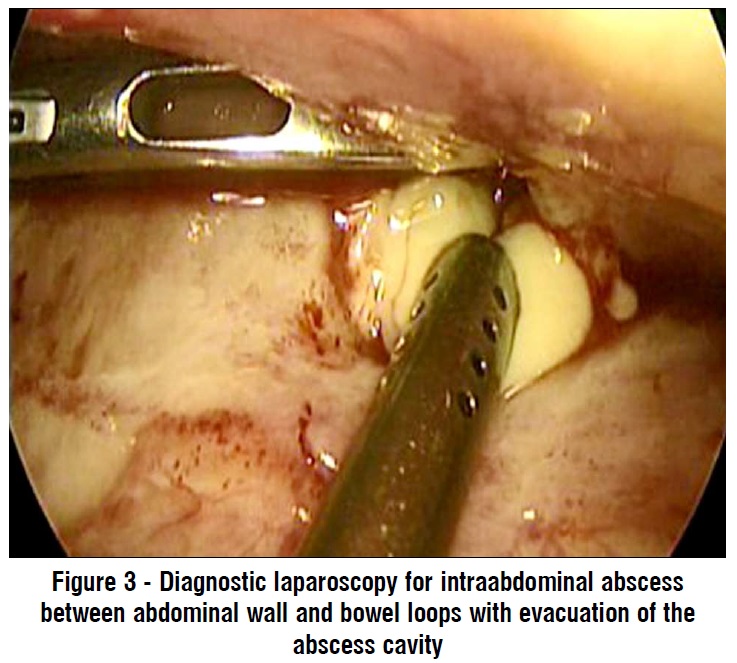
Regarding the management of these 11 cases of intraabdominal collection, 2 cases (one in each group) did not need intervention due to no clinical manifestation or sizable collection, 5 patients were manged using ultrasound guided insertion of pigtail in the collection with intravenous antibiotics, 3 cases were managed with diagnostic laparoscopy with irrigation and suction using normal saline (fig. 3) and one case required conversion to midline exploration for drainage (table 5).
DISCUSSION
Acute appendicitis is considered the most common cause of presentation to surgical emergency departments (1). Laparoscopic appendectomy was introduced by Semm in 1983 (19), and now it is considered a safe and effective surgical treatment of acute appendicitis (10). It has the advantage of lower incidence of wound infection, less postoperative pain, shorter hospital stay and time to return to work (12).
Laparoscopic appendectomy for complicated appendicitis has a high risk for the development of postoperative intraabdominal abscess (20). In these cases, surgeons prefer to use an intraabdominal drain inserted into the pelvis, claiming that it has a protective effect against postoperative intraabdominal abscess development (1). But this abdominal drain cannot drain all the abdominal cavity especially in laparoscopic approach which may facilitate the dissemination of the collection away from the surgical site to be missed within small cavities especially between the greater omentum (5).
In this study, our aim was to evaluate the effect of abdominal drain placement after laparoscopic appendectomy for complicated acute appendicitis on the incidence of postoperative morbidities. We had a nonsignificant difference between group A and B regarding postoperative complication (37.5% versus 32.5% respectively) and postoperative intraabdominal abscess formation (15% versus 12.5%) respectively). While we had a significantly statistical difference between both group as regard mean the hospital stay (2.95 days versus 2.38 days respectively).
Interestingly this was the conclusion of a systemic analysis comparing the placement of drain with nodrain in open appendectomy for complicated appendicitis, the study revealed that there is no difference between the two groups as regard the development of postoperative intraabdominal abscess (21). Also, a study by Cho et al. proved that not using a post appendectomy drain is not necessarily associated with postoperative intraabdominal abscess formation. (19) A study by Schlottmann et al. also confirmed the same conclusion, after studying the effect of using or not using the drain post laparoscopic appendectomy for 225 complicated appendicitis. Their study didn’t find any statistical difference between two groups as regard the operative time and minor or major complications including postoperative intrabdominal abscess formation (1). All these findings are compatible with our study although the big difference in the included participants (225 patient vs 80 patients).
Schlottmann et al. found that the mean hospital stay was significantly higher in the drain group (5.5 days) versus (2.9 days) in the no-drain group (p: 0.001), and this was postulated to the fact that abdominal drains act as foreign body and may induce ileus which delays the intestinal motility and thus the hospital discharge (1). In our study , the incidence of ileus was higher in the drain group than the no-drain one, although this difference was statistically nonsignificant, but it may prolong the hospital stay between both groups.
Allemann et al. conducted a case matched retrospective study to compare between drain or no-drain in laparoscopic appendectomy. They found a non-significant statistical difference between both groups in intraabdominal collection as in our study. But they had a statistically significant difference in overall complication and abdominal wall abscess in favor of the no-drain group. On the other hand, they had longer hospital stay in the patients with postoperative drain (statistically significant) as in our study (5).
On the other hand, Beek et al. studied retrospectively 199 patients with complicated appendicitis who underwent both open and laparoscopic appendectomy performed by 21 different surgeons with at least 3 of them who never use an intra-peritoneal drain after appendectomies to evaluate the effect of intraabdominal drain in both approaches for complicated appendicitis. They had a non-significant statistical difference between both groups in individual complications (which included: post-appendectomy intraabdominal abscess formation, stump leak, wound infections, or other non-surgical complications) but the overall complication rate was significantly higher in the drain group versus no drain one. Because they considered the postoperative pain (which was significantly higher in the drain group) as a postoperative complication (22).
We had many limitations in our study. Our sample size was relatively small, we need a randomized controlled study on a larger sample size for more statistically solid results.
CONCLUSION
In laparoscopic approach of complicated acute appendicitis, we didn’t find any benefits from applying intraabdominal drain as regard overall morbidity, minor complications (Clavien I-II) or major complications (Clavien III-IV). Besides, the drain may even lengthen the hospital stay.
Author contribution
(I) Conception and design: Hossam S Abdelrahim
(II) Administrative support: Ahmed F Amer
(III) Provision of study materials or patients: Hossam S Abdelrahim
(IV) Collection and assembly of data: Ehab Mohammed Ali Fadl
(V) Data analysis and interpretation: Ehab Mohammed Ali Fadl
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of interest
All authors have no related conflicts of interest to declare.
Funding and Financial support
This research did not receive any specific grant from funding agencies in the public, commercial or notfor- profit sectors.
REFERENCES
1. Schlottmann F, Reino R, Sadava EE, Campos Arbulú A, Rotholtz NA. Could an abdominal drainage be avoided in complicated acute appendicitis? Lessons learned after 1300 laparoscopic appendectomies. Int J Surg. 2016; 36:40-43.
2. Horn AE, Ufberg JW. Appendicitis, diverticulitis, and colitis. Emerg Med Clin N Am. 2011;29(2):347-368.
3. Moraitis D, Kini SU, Annamaneni RK, Zitsman JL. Laparoscopy in complicated pediatric appendicitis. JSLS. 2004; 8:310-313.
4. Sahbaz NA, Bat O, Kaya B, Ulukent SC, Ilkgül Ö, Özgün MY, et al. The clinical value of leucocyte count and neutrophil percentage in diagnosing uncomplicated (simple) appendicitis and predicting complicated appendicitis. Ulus Travma Acil Cerrahi Derg. 2014; 20(6):423-426.
5. Allemann P, Probst H, Demartines N, Schäfer M. Prevention of infectious complications after laparoscopic appendectomy for complicated acute appendicitis--the role of routine abdominal drainage. Langenbecks Arch Surg. 2011 Jan;396(1):63-8.
6. Cueto J, Dallemagne B, Vázquez-Frias JA, Gomez S, Delgado F, Trullenque L, et al. Morbidity of laparoscopic surgery for complicated appendicitis: an international study. Surg Endosc. 2006; 20(5):717–720.
7. Ming PC, Yan TY, Tat LH. Risk factors of postoperative infections in adults with complicated appendicitis. Surg Laparosc Endosc Percutan Tech. 2009;19(3):244–248.
8. Newman K, Ponsky T, Kittle K, Dyk L, Throop C, Gieseker K, et al. Appendicitis 2000: variability in practice, outcomes, and resource utilization at thirty pediatric hospitals. J Pediatr Surg. 2003;38(3): 372-9; discussion 372-9.
9. David VL, Ciornei B, Popoiu MC, Iacob RE, Boia ES. Is there a role for prophylactic drainage of the abdominal cavity after laparoscopic appendectomy for non-complicated appendicitis in children? J Ped Endosc Surg. 2019; 1:71–74.
10. Di Saverio S, Podda M, De Simone B, Ceresoli M, Augustin G, Gori, A, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020; 15(1):27.
11. Jaschinski T, Mosch C, Eikermann M, Neugebauer EA. Laparoscopic versus open appendectomy in patients with suspected appendicitis: a systematic review of meta-analyses of randomized controlled trials. BMC Gastroenterol. 2015;15:48.
12. Yu MC, Feng YJ, Wang W, Fan W, Cheng HT, Xu J. Is laparoscopic appendectomy feasible for complicated appendicitis ?A systematic review and meta-analysis. Int J Surg. 2017;40:187-197.
13. Piskun G, Kozik D, Rajpal S, Shaftan G, Fogler R. Comparison of laparoscopic, open, and converted appendectomy for perforated appendicitis. Surg Endosc 2001;15(7):660-662.
14. Sridhar M, Guerrero M, Miller J, Hanna P, Haghshenas J, Zuberi J. Analysis of Outcomes Using Intraoperative Irrigation and Drainage for Complicated Appendicitis. J Curr Surg. 2019;9(2-3):17-21
15. Smith SR, Gilmore OJ. Surgical drainage. Br J Hosp Med. 1985; 33(6):308-315.
16. Schein M. To drain or not to drain? The role of drainage in the contaminated and infected abdomen: an international and personal perspective. World J Surg. 2008;32(2):312-321.
17. Petrowsky H, Demartines N, Clavien PA. Evidence-based values of prophylactic drainage in gastrointestinal surgery. Ann Surg. 2004; 240:1074–1085.
18. Katayama H, Kurokawa Y, Nakamura K, Ito H, Kanemitsu Y, Masuda N, et al. Extended Clavien-Dindo classification of surgical complications: Japan Clinical Oncology Group postoperative complications criteria. Surg Today. 2016 Jun;46(6):668-85.
19. Cho J, Park I, Lee D, Sung K, Baek J, Lee J. Risk factors for postoperative intraabdominal abscess after laparoscopic appendectomy: analysis for consecutive 1817 experiences. Dig. Surg. 2015;32: 375-381.
20. Markides G, Subar D, Riyad K. Laparoscopic versus open appendectomy in adults with complicated appendicitis: systematic review and meta-analysis, World J. Surg. 2010;34(9):2026-2040.
21. Cheng Y, Zhou S, Zhou R, Lu J, Wu S, Xiong X, et al. Abdominal drainage to prevent intra-peritoneal abscess after open appendectomy for complicated appendicitis. Cochrane Database Syst Rev. 2015;(2):CD010168.
22. Beek MA, Jansen TS, Raats JW, Twiss EL, Gobardhan PD, van Rhede van der Kloot EJ. The utility of peritoneal drains in patients with perforated appendicitis. Springer plus. 2015;4:371.
Full Text Sources:
Abstract:
Views: 16276

Methodology: This is a prospective comparative study which was performed at Ain Shams University Hospitals between September 2018 and September 2021. It included 80 patients who underwent laparoscopic appendectomy for complicated appendicitis. The patients were divided sequentially into two groups, Group A: drain group and Group B: no-drain group.
Results: We had a non-significant difference between group A and B regarding postoperative complication (37.5% versus 32.5% respectively) and postoperative intraabdominal abscess formation (15% versus 12.5%) respectively). The no-drain group showed significantly shorter hospital stay than the drain group. We had no mortality in our study.
Conclusion: In our study, we didn’t find considerable benefits for using the drain over intraperitoneal irrigation and lavage without drain after laparoscopic appendectomy for complicated appendicitis with significant longer hospital stay in the drain group.
INTRODUCTION
Acute appendicitis is the most common surgical cause of acute abdomen that requires surgical intervention for its management with lifetime risk of 7-8% (1,2). The incidence of complicated acute appendicitis ranges from 20% to 30% of all appendicitis patients (3). Complicated acute appendicitis includes perforated appendix, gangrenous appendicitis, intraabdominal abscess, and generalized peritonitis (4).
While uncomplicated acute appendicitis can be safely managed with low postoperative complication, complicated acute appendicitis is still associated with significant postoperative morbidity (5-7). Postoperative complications can occur in up to 0.8-1.7% of the patients with uncomplicated appendicitis, while in complicated appendicitis postoperative complications can occur in 14-18% of patients, especially postoperative development of intraabdominal abscess (8,9) Laparoscopic appendectomy is considered now to be the preferable surgical approach for acute appendicitis with better cosmesis, less postoperative pain, lower incidence of surgical site infection, faster recovery, and better postoperative quality of life in comparison to open approach (10-12).
But on the other side, laparoscopy in complicated appendicitis may be a predisposing factor for higher incidence of postoperative abscess formation because pneumoperitoneum mostly opens the intrabdominal spaces (13).
However, when it comes to the management of complicated appendicitis either open or laparoscopic, surgeons debate about the use of some intraoperative techniques as the irrigation or the use of intraabdominal drain (14). The later had long history with conflicting viewpoints, Wiliam Halsted stated, "No drainage at all is better than the ignorant employment of it" (15) while Robert Tait was against Halsted's opinion as he stated, “When in doubt drain!” (16). Placement of abdominal drain after different types of surgeries is still controversial, it was assumed that the drains help in prevention of collection of infected fluids and in early detection of bleeding and leakage, but this is questionable now (5). Recently, it was proved that the use of intraabdominal drains in liver and colorectal surgery are not always beneficial but may even be harmful. So, there is an evolving trend towards fast-track surgery without using of intraabdominal drain in different types of abdominal surgeries (17). We aimed in this study to evaluate the effect of abdominal drain placement after laparoscopic appendectomy for complicated acute appendicitis on the incidence of postoperative morbidities.
PATIENTS AND METHODS
This study was a prospective comparative study which was performed at Ain Shams University Hospitals between September 2018 and September 2021. It included 80 patients who underwent laparoscopic appendectomy for complicated appendicitis. All cases were operated by the same surgical team.
Ethical considerations
The study got approval from the ethical committee of general surgery department and a written informed consent was taken from all participants after receiving an explanation of the study.
Eligibility criteria for the study
The study included cases of complicated appendicitis defined as perforated appendix, gangrenous appendix and presence of pus or peri-appendicular abscess by preoperative pelviabdominal ultrasound (US) and confirmed by diagnostic laparoscopy (fig. 1). Patients presented with uncomplicated acute appendicitis or appendicular mass, aged < 14 years, unfit to pneumoperitoneum or converted to open were excluded from this study. Also, we excluded cases with intraoperative acute haemorrhage warranting drain applying. Then the included cases were divided sequentially into two groups, 40 patients in each, Group A in which an abdominal drain was used and Group B in which no drain was left in the abdomen with just irrigation and lavage with normal saline.
Preoperative workup
Detailed history, general and abdominal examination were done for all patients. Full blood tests including inflammatory markers and US were done. Pelviabdominal computerized tomography (CT) with contrast was done if doubtful diagnosis or for patients ? 50 years old. Diagnosis of acute appendicitis was stablished by clinical diagnosis and confirmed by image and if still doubtful, diagnosis by laparoscopy was done.
Surgical management (fig. 2)
All patients received intra-venous (IV) ceftriaxone 2 gm and metronidazole 500 mg at induction of anaesthesia. Left subcostal insertion of veress needle was done to establish the pneumoperitoneum then introducing a visiport trocar (5-12 mm) at the umbilicus, with 2 other trocars placed at suprapubic (10 mm) and left iliac fossa (5 mm).
The procedure started with checking the site of veress needle, diagnostic laparoscopy was performed to identify the appendix and to confirm presence of complicated appendicitis as perforated appendix, gangrenous appendix and presence of pus or peri-appendicular abscess. The mesoappendix was ligated with 2/0 vicryl (Ethicon) suture then dissected using the electrocautery, the appendicular base was secured with 2/0 vicryl® (Ethicon) intracorporeal sutures and titanium clips. The specimen was removed through 10 mm port. Intraperitoneal lavage using saline 0.9% was done at the end of the operation. In group A, a tube drain was placed in the pelvic cavity.
Postoperative management
Follow up of the drain output and vital data was done together with parenteral administration of third generation cephalosporin and metronidazole. The drain was removed once the output was less than 50 ml/day of clear fluid. Patients started oral fluids intake once bowel sounds were audible and were discharged from hospital when oral intake was tolerated. Routine ultrasound was done for all patients to exclude postoperative collection either at the 5th postoperative day if the patient was not suspected clinically or at any time if the patient was suspected clinically by persistent fever, peritonitis and/or ileus. Follow up of the cases were planned at 10th and 21st postoperative days.
Data collection and surgical outcome
The patients demographic data and comorbidities in both groups were collected and compared. Both groups were compared as regard the following outcomes: - Primary outcome was the development of postoperative intraabdominal abscess or intraabdominal fluid collection (detected by US).
- Secondary outcomes were duration of operation, the length of hospital stay, other postoperative complications (atelectasis, wound infection, pneumonia, and ileus). we relied on Clavien- Dindo system (18) for the classification of surgical and non-surgical postoperative complications.
Data management and analysis
Data were revised, coded, entered on a computer and analysed using SPSS package version number 26. Student t-test was used for comparing quantitative variables between the two study groups. Chi-square and Fisher exact tests were used to test the association between qualitative variables. P-value ? 0.05 was considered significant and P-value ? 0.001 was considered highly significant.
RESULTS
Our study included 80 cases of laparoscopic appendectomy for complicated appendicitis. Patients were divided into two groups (40 patients in each), Group A (drain group) and Group B (no-drain group). There was a non-significant statistical difference in two groups regarding the demographics of the patients, comorbidities and preoperative investigations data as shown in table 1.
In our study, there was a non-significant difference between the two groups as regard length of operation and intraoperative finding of appendix as shown in table 2. We had no intraoperative morbidities in both groups.
Postoperative pain was controlled by non-steroidal anti-inflammatory drugs and paracetamol in all cases with no need to opioids. In the analysis of the postoperative morbidity (whatever minor or major depending on Clavien-Dindo system), we had a nonsignificant statistical difference between the two groups (37.5% in group A versus 32.5% in group B). Major complications (Clavien III, postoperative intraabdominal abscess) were recorded in 6 cases (15%) in group A versus 5 cases (12.5%) in group B, with nonsignificant statistical difference between both. The no-drain group showed significantly shorter hospital stay than the drain group (2.38 days versus 2.95 days respectively) (table 3). There were no mortality cases or Clavien IV complications in either group.
Cases with postoperative wound infection were managed by antibiotics and bed side dressing, with no need for operative management, while cases with postoperative ileus required the insertion of naso-gastric tube in 2 patients, one in each group. The only case with post appendectomy pneumonia was managed with IV antibiotics and chest physiotherapy, but the patient required more than one week to be discharged from the hospital.
Of all cases with intraabdominal collection in both groups (11 cases), 4 patients were diabetic (two in each group), 7 patients were discovered by clinical suspicion (persistent abdominal pain and fever) in the postoperative course before the routine pelvi-abdominal ultrasound. Ultrasound was done and confirmed the diagnosis of intraabdominal collection. Another 3 cases were accidently discovered without any clinical suspicion on the 5th postoperative day with the routine pelvi-abdominal ultrasound. One case was discovered one week after discharge (10 days after the appendectomy) as the case presented with server abdominal pain and high-grade fever (table 4).
Regarding the management of these 11 cases of intraabdominal collection, 2 cases (one in each group) did not need intervention due to no clinical manifestation or sizable collection, 5 patients were manged using ultrasound guided insertion of pigtail in the collection with intravenous antibiotics, 3 cases were managed with diagnostic laparoscopy with irrigation and suction using normal saline (fig. 3) and one case required conversion to midline exploration for drainage (table 5).
DISCUSSION
Acute appendicitis is considered the most common cause of presentation to surgical emergency departments (1). Laparoscopic appendectomy was introduced by Semm in 1983 (19), and now it is considered a safe and effective surgical treatment of acute appendicitis (10). It has the advantage of lower incidence of wound infection, less postoperative pain, shorter hospital stay and time to return to work (12).
Laparoscopic appendectomy for complicated appendicitis has a high risk for the development of postoperative intraabdominal abscess (20). In these cases, surgeons prefer to use an intraabdominal drain inserted into the pelvis, claiming that it has a protective effect against postoperative intraabdominal abscess development (1). But this abdominal drain cannot drain all the abdominal cavity especially in laparoscopic approach which may facilitate the dissemination of the collection away from the surgical site to be missed within small cavities especially between the greater omentum (5).
In this study, our aim was to evaluate the effect of abdominal drain placement after laparoscopic appendectomy for complicated acute appendicitis on the incidence of postoperative morbidities. We had a nonsignificant difference between group A and B regarding postoperative complication (37.5% versus 32.5% respectively) and postoperative intraabdominal abscess formation (15% versus 12.5%) respectively). While we had a significantly statistical difference between both group as regard mean the hospital stay (2.95 days versus 2.38 days respectively).
Interestingly this was the conclusion of a systemic analysis comparing the placement of drain with nodrain in open appendectomy for complicated appendicitis, the study revealed that there is no difference between the two groups as regard the development of postoperative intraabdominal abscess (21). Also, a study by Cho et al. proved that not using a post appendectomy drain is not necessarily associated with postoperative intraabdominal abscess formation. (19) A study by Schlottmann et al. also confirmed the same conclusion, after studying the effect of using or not using the drain post laparoscopic appendectomy for 225 complicated appendicitis. Their study didn’t find any statistical difference between two groups as regard the operative time and minor or major complications including postoperative intrabdominal abscess formation (1). All these findings are compatible with our study although the big difference in the included participants (225 patient vs 80 patients).
Schlottmann et al. found that the mean hospital stay was significantly higher in the drain group (5.5 days) versus (2.9 days) in the no-drain group (p: 0.001), and this was postulated to the fact that abdominal drains act as foreign body and may induce ileus which delays the intestinal motility and thus the hospital discharge (1). In our study , the incidence of ileus was higher in the drain group than the no-drain one, although this difference was statistically nonsignificant, but it may prolong the hospital stay between both groups.
Allemann et al. conducted a case matched retrospective study to compare between drain or no-drain in laparoscopic appendectomy. They found a non-significant statistical difference between both groups in intraabdominal collection as in our study. But they had a statistically significant difference in overall complication and abdominal wall abscess in favor of the no-drain group. On the other hand, they had longer hospital stay in the patients with postoperative drain (statistically significant) as in our study (5).
On the other hand, Beek et al. studied retrospectively 199 patients with complicated appendicitis who underwent both open and laparoscopic appendectomy performed by 21 different surgeons with at least 3 of them who never use an intra-peritoneal drain after appendectomies to evaluate the effect of intraabdominal drain in both approaches for complicated appendicitis. They had a non-significant statistical difference between both groups in individual complications (which included: post-appendectomy intraabdominal abscess formation, stump leak, wound infections, or other non-surgical complications) but the overall complication rate was significantly higher in the drain group versus no drain one. Because they considered the postoperative pain (which was significantly higher in the drain group) as a postoperative complication (22).
We had many limitations in our study. Our sample size was relatively small, we need a randomized controlled study on a larger sample size for more statistically solid results.
CONCLUSION
In laparoscopic approach of complicated acute appendicitis, we didn’t find any benefits from applying intraabdominal drain as regard overall morbidity, minor complications (Clavien I-II) or major complications (Clavien III-IV). Besides, the drain may even lengthen the hospital stay.
Author contribution
(I) Conception and design: Hossam S Abdelrahim
(II) Administrative support: Ahmed F Amer
(III) Provision of study materials or patients: Hossam S Abdelrahim
(IV) Collection and assembly of data: Ehab Mohammed Ali Fadl
(V) Data analysis and interpretation: Ehab Mohammed Ali Fadl
(VI) Manuscript writing: All authors
(VII) Final approval of manuscript: All authors
Conflict of interest
All authors have no related conflicts of interest to declare.
Funding and Financial support
This research did not receive any specific grant from funding agencies in the public, commercial or notfor- profit sectors.
REFERENCES
1. Schlottmann F, Reino R, Sadava EE, Campos Arbulú A, Rotholtz NA. Could an abdominal drainage be avoided in complicated acute appendicitis? Lessons learned after 1300 laparoscopic appendectomies. Int J Surg. 2016; 36:40-43.
2. Horn AE, Ufberg JW. Appendicitis, diverticulitis, and colitis. Emerg Med Clin N Am. 2011;29(2):347-368.
3. Moraitis D, Kini SU, Annamaneni RK, Zitsman JL. Laparoscopy in complicated pediatric appendicitis. JSLS. 2004; 8:310-313.
4. Sahbaz NA, Bat O, Kaya B, Ulukent SC, Ilkgül Ö, Özgün MY, et al. The clinical value of leucocyte count and neutrophil percentage in diagnosing uncomplicated (simple) appendicitis and predicting complicated appendicitis. Ulus Travma Acil Cerrahi Derg. 2014; 20(6):423-426.
5. Allemann P, Probst H, Demartines N, Schäfer M. Prevention of infectious complications after laparoscopic appendectomy for complicated acute appendicitis--the role of routine abdominal drainage. Langenbecks Arch Surg. 2011 Jan;396(1):63-8.
6. Cueto J, Dallemagne B, Vázquez-Frias JA, Gomez S, Delgado F, Trullenque L, et al. Morbidity of laparoscopic surgery for complicated appendicitis: an international study. Surg Endosc. 2006; 20(5):717–720.
7. Ming PC, Yan TY, Tat LH. Risk factors of postoperative infections in adults with complicated appendicitis. Surg Laparosc Endosc Percutan Tech. 2009;19(3):244–248.
8. Newman K, Ponsky T, Kittle K, Dyk L, Throop C, Gieseker K, et al. Appendicitis 2000: variability in practice, outcomes, and resource utilization at thirty pediatric hospitals. J Pediatr Surg. 2003;38(3): 372-9; discussion 372-9.
9. David VL, Ciornei B, Popoiu MC, Iacob RE, Boia ES. Is there a role for prophylactic drainage of the abdominal cavity after laparoscopic appendectomy for non-complicated appendicitis in children? J Ped Endosc Surg. 2019; 1:71–74.
10. Di Saverio S, Podda M, De Simone B, Ceresoli M, Augustin G, Gori, A, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020; 15(1):27.
11. Jaschinski T, Mosch C, Eikermann M, Neugebauer EA. Laparoscopic versus open appendectomy in patients with suspected appendicitis: a systematic review of meta-analyses of randomized controlled trials. BMC Gastroenterol. 2015;15:48.
12. Yu MC, Feng YJ, Wang W, Fan W, Cheng HT, Xu J. Is laparoscopic appendectomy feasible for complicated appendicitis ?A systematic review and meta-analysis. Int J Surg. 2017;40:187-197.
13. Piskun G, Kozik D, Rajpal S, Shaftan G, Fogler R. Comparison of laparoscopic, open, and converted appendectomy for perforated appendicitis. Surg Endosc 2001;15(7):660-662.
14. Sridhar M, Guerrero M, Miller J, Hanna P, Haghshenas J, Zuberi J. Analysis of Outcomes Using Intraoperative Irrigation and Drainage for Complicated Appendicitis. J Curr Surg. 2019;9(2-3):17-21
15. Smith SR, Gilmore OJ. Surgical drainage. Br J Hosp Med. 1985; 33(6):308-315.
16. Schein M. To drain or not to drain? The role of drainage in the contaminated and infected abdomen: an international and personal perspective. World J Surg. 2008;32(2):312-321.
17. Petrowsky H, Demartines N, Clavien PA. Evidence-based values of prophylactic drainage in gastrointestinal surgery. Ann Surg. 2004; 240:1074–1085.
18. Katayama H, Kurokawa Y, Nakamura K, Ito H, Kanemitsu Y, Masuda N, et al. Extended Clavien-Dindo classification of surgical complications: Japan Clinical Oncology Group postoperative complications criteria. Surg Today. 2016 Jun;46(6):668-85.
19. Cho J, Park I, Lee D, Sung K, Baek J, Lee J. Risk factors for postoperative intraabdominal abscess after laparoscopic appendectomy: analysis for consecutive 1817 experiences. Dig. Surg. 2015;32: 375-381.
20. Markides G, Subar D, Riyad K. Laparoscopic versus open appendectomy in adults with complicated appendicitis: systematic review and meta-analysis, World J. Surg. 2010;34(9):2026-2040.
21. Cheng Y, Zhou S, Zhou R, Lu J, Wu S, Xiong X, et al. Abdominal drainage to prevent intra-peritoneal abscess after open appendectomy for complicated appendicitis. Cochrane Database Syst Rev. 2015;(2):CD010168.
22. Beek MA, Jansen TS, Raats JW, Twiss EL, Gobardhan PD, van Rhede van der Kloot EJ. The utility of peritoneal drains in patients with perforated appendicitis. Springer plus. 2015;4:371.
Full Text Sources:
Abstract:
Views: 16276
Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Dec 2025
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.