Surgery, Gastroenterology and Oncology

|
|
Background. This study aimed to compare the efficacy of laparoscopically guided transversus abdominis plane (L-TAP) block and ultrasound-guided erector spinae plane (ESP) block in the alleviation of postoperative pain and need for postoperative narcotics in patients undergoing laparoscopic bariatric surgery.
Methods. In this randomized controlled trial, we included adult morbidly obese patients undergoing laparoscopic bariatric surgery. After induction of anesthesia, participants received either L-TAP block or ultrasound-guided ESP block. Postoperative analgesia was 1 gm paracetamol every 6h and 30 mg ketorolac every 12h. Postoperative pain was assessed at 1, 6, 12, and 24 h using the numeric rating scale (NRS), and breakthrough pain was treated with 5 mg nalbuphine bolus. The primary outcome was the NRS at 24 h. Secondary outcomes included NRS at 1, 6, and 12 h, postoperative nalbuphine consumption, number of patients needing postoperative nalbuphine, and incidence of nausea and vomiting.
Results. Ninety-six patients were available for the final analysis. Postoperative NRS, post-operative nalbuphine consumption, number of patients needing postoperative nalbuphine, and incidence of nausea and vomiting were not statistically different between the two groups.
Conclusion. In obese patients undergoing laparoscopic bariatric surgery, both L-TAP block and ultrasound-guided ESP block showed comparable postoperative analgesic profile.
INTRODUCTION
Postoperative pain relief is an imperative facet of postoperative patient care. Pain management not only improves patient satisfaction, but also plays a vital role in patients’ physiological and psychological recovery from surgery. Post-operative pain alleviation is of particular import in obese patients, a population plagued with a predisposition for poor postoperative ventilation and chest expansion, respiratory depression and obstructive sleep apnea (1).
While the use of narcotics in the relief of postoperative pain has stood the test of time, their employment in the postoperative pain management of the obese patient only increases the risk of these undesirable respiratory and cardiovascular complications (2).
Opioid-sparing regimens are therefore encouraged in this context. These rely on non-narcotic medications in addition to regional anesthetic techniques such as Transversus Abdominis Plane block and Erector Spinae Plane block (ESPB), in order to minimize the reliance on narcotic analgesia and mitigate their harmful effects (2).
The administration of TAP block through laparoscopic guidance (L-TAP) was first proposed in 2011and has shown favorable results in the form of improved pain relief and reduced overall cost (3). The ESPB was first described by Forero et al in 2016 (4). It has shown potential in postoperative pain alleviation across a
myriad of abdominal surgeries (5).
The two blocks showed good results in several abdominal surgeries; however, no study, to the best of our knowledge compared both blocks in bariatric surgery. This study aimed to compare the efficacy of laparoscopically guided TAP block and ultrasound-guided ESP block in the alleviation of postoperative pain and need for postoperative narcotics in patients undergoing laparoscopic bariatric surgery.
METHODS
This is a randomized clinical trial carried out over a period from August 2024 to January 2025 and included ninety-six morbidly obese patients undergoing laparoscopic bariatric surgery in Cairo University. The study was approved by the institutional research board (MD-292-2022) and registered at clinicaltrials.gov registry (identifier: NCT06564610). Informed consent was obtained from all patients prior to their inclusion in the study. The participants were randomized into two groups using computer-generated table sequence:
The study included patients with the following criteria:
Age above 18 and under 60 years at time of surgery;
Body mass index (BMI) ? 40 kg/m2 or BMI ? 35 kg/m2 and at least one obesity-related comorbidity such as: type II diabetes, hypertension, sleep apnea and other respiratory disorders, non-alcoholic fatty liver disease, osteoarthritis, lipid abnormalities, or heart disease.
Inability to achieve a healthy weight loss sustained for a period of time with prior weight loss efforts.
Patients with one or more of the following criteria were excluded from the study:
• Allergy to local anesthetic drugs.
• Bleeding disorders.
• Refusal to receive the intervention.
• Pregnancy or lactation.
In all patients, general anesthesia was induced using propofol 1-2 mg/kg over 20-30 seconds, fentanyl 2 mcg/kg, and rocuronium 0.6 mg/kg to facilitate endotracheal intubation. Anesthesia was maintained using isoflurane 1.5 %, and rocuronium top-up boluses as needed. For all patients, balanced crystalloid solution was infused at a rate of 4 mL/kg/h. Any additional fluid losses were replaced according to local protocols.
The patients were randomly allocated into one of the two study groups: Group A: received L-TAP block; and group B: received ESP block. The two blocks were performed after induction of general anesthesia and securing the tracheal tube in place. L-TAP block was performed by the surgeon at the beginning of the surgical procedure while ESPB was performed by the attending anesthesiologist in the lateral position before starting the surgery.
L-TAP Technique
Utilizing the laparoscopic camera, a subcostal injection of (10 mL lidocaine 2% + 10 mL bupivacaine 0.5%) is given just lateral to the rectus muscle on either side and another injection of (10 mL bupivacaine 0.5% + 10 mL saline 0.9%) at the anterior axillary line midway between costal margin and iliac crest on either side.
Effective site injection at the transversus abdominis plane is ensured using laparoscopic camera by observing the so-called “Doyle’s Bulge”, not to be confused with a peritoneal blister which would indicate erroneous injection into preperitoneal space.
Erector Spinae Plane Block Technique
The block is performed at the level of the T7 transverse process with the patient in the lateral position using a low frequency curved-array ultrasound probe. First, the T7 spinous process level is identified by palpation and downward counting from the C7 spinous process. The probe is positioned transversely to identify the tip of the T7 transverse process then rotated longitudinally to obtain a parasagittal view visualizing skin and subcutaneous tissue layers, trapezius muscle, and lastly the erector spinae muscle just superficial to the transverse processes. The rhomboid major muscle has its lower border at the T5-6 vertebral level and its absence is used as additional confirmation that the T7 transverse process is being viewed.
Using the in-plane approach, a 22-G needle was directed craniocaudally till it contacts the T7 transverse process and the needle tip is positioned in the fascial plane deep to the erector spinae muscle. The correct location is confirmed by injecting 0.5 to 1 mL saline causing lifting of the erector spinae muscle off the transverse process without muscle distention and observing the craniocaudal spread of injectate. A total of 20 mL bupivacaine 0.25% is then injected into the erector spinae plane, and the procedure is repeated on the other side.
Intraoperative Analgesic Management
If the patient developed intraoperative tachycardia and/or hypertension (defined as increased readings by 25% of the baseline readings), Fentanyl boluses were administered (0.5 mcg/kg). All patients received IV paracetamol (1 gm) and ketorolac (60 mg) by the end of the surgery.
Routine Postoperative Analgesia
Both groups received postoperative analgesia as per the surgery department guidelines in the form of: IV Paracetamol 1 mg every 6 hours and ketorolac (30 mg) every 12 h. Any breakthrough pain was managed by nalbuphine 5 mg bolus, unless the patient had obstructive airway pathology.
Primary Outcomes
Numerical Rating Scale (NRS) for pain assessment 24 hours postoperative. The Numerical Pain Rating Scale was taught to the patients in the preoperative visit as an eleven-point numerical scale. A score of 0 denoted that there is no pain al all while a score of 10 is considered the worst imaginable pain.
Secondary Outcomes
Numerical Rating Scale scores for pain at 1, 6, 12 and 24 hours postoperatively.
Cumulative 24-hour postoperative rescue narcotic consumption.
Intraoperative heart rate and blood pressure measurements (will be recorded every 15 min then the average will be calculated).
Postoperative blood pressure and heart rate every 6 hours.
Incidence of postoperative Nausea and vomiting.
Sample Size
Our primary outcome is the NRS 24 hours post-operative. In a previous study, the mean NRS in patients who received laparoscopic TAP block was 4±2. We calculated a sample size that could detect a mean difference of 30% (i.e., 1.2 point) between study groups. Using MedCalc Software version 14 (MedCalc Software bvba, Ostend, Belgium), a sample size of 90 patients (45 patients per group) was needed to have a study power of 80% and alpha error of 0.05. The number was increased by 10% to be 100 envelopes to compensate for possible dropouts.
Statistical Analysis
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA). Data was summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Mann-Whitney test. For comparing categorical data, Chi square (?2) test was performed. Exact test was used instead when the expected frequency is less than 5. P-values less than 0.05 were considered as statistically significant.
RESULTS
Ninety-six patients were available for the final analysis (fig. 1).
Figure 1 - CONSORT’s flowchart.
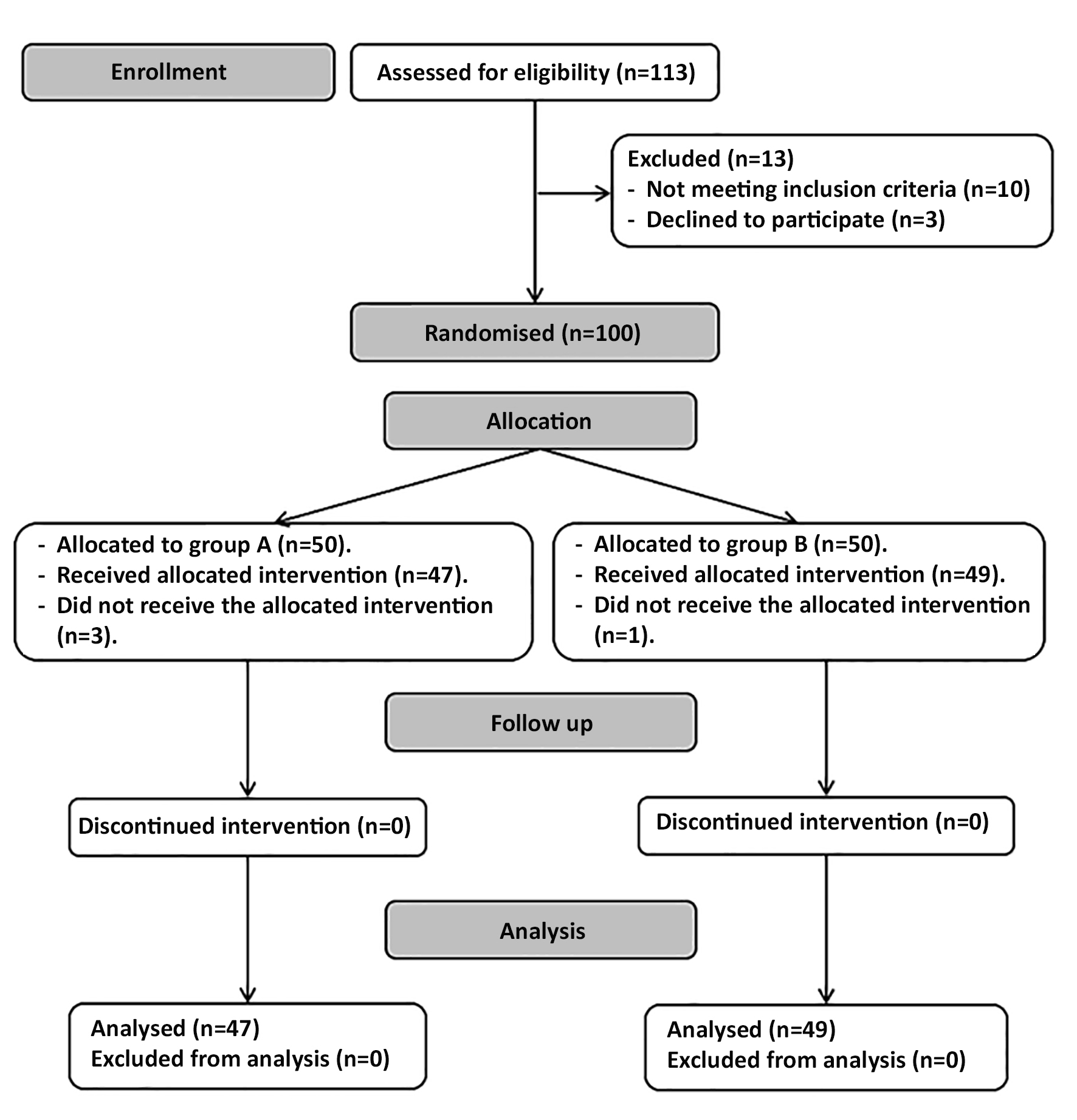
Table 1 - Demographic data. Data are presented as frequency, mean (standard deviation) and median (quartiles).
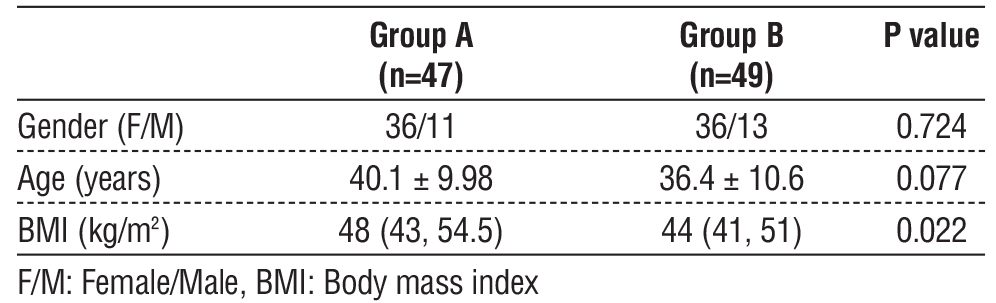
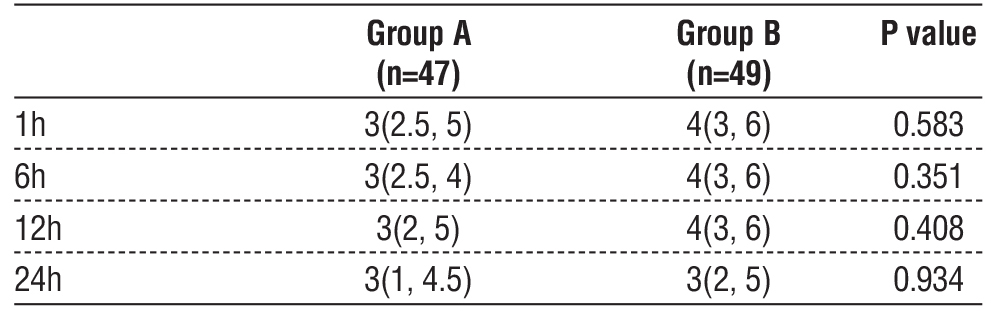
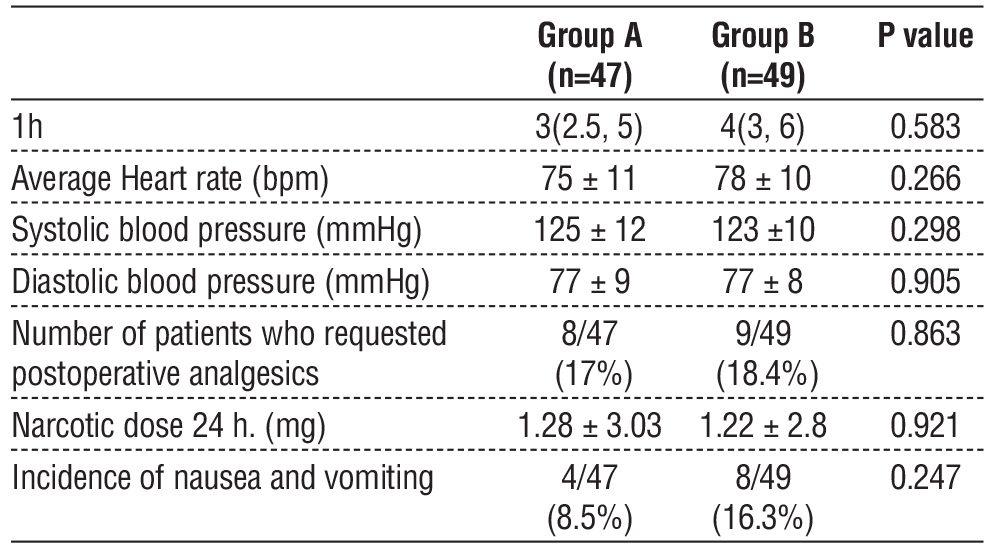
The two study groups were comparable in the demographic data (gender – age). The BMI was slightly higher in group 1 compared to group 2 (P=0.02) (table 1). None of the two groups were superior in the postoperative pain scores (table 2). Hemodynamic measurements showed comparable heart rate and blood pressure readings (table 3). The number of patients who requested postoperative analgesia, incidence of nausea or vomiting, and total postoperative analgesic consumption was also comparable in the two groups (table 3).
Table 2 - Pain scores. Data are presented as median (quartiles).
DISCUSSION
In morbidly obese patients, excess adipose tissue and elevated intra-abdominal pressure can influence block dynamics and pain pathways. The TAP block relies on predictable spread within the neurofascial plane; however, increased adiposity may restrict lateral diffusion and predominantly provides somatic analgesia, which may be insufficient given the heightened visceral nociception associated with bariatric surgery. In contrast, the erector spinae block facilitates more reliable longitudinal spread within the paraspinal compartment and engages both dorsal and ventral rami, offering partial visceral analgesia that may be particularly advantageous in this population. Laparoscopic sleeve gastrectomy generally involves less extensive mesenteric traction and shorter operative duration, with pain predominantly arising from somatic abdominal wall structures. In contrast, Roux-en-Y gastric bypass requires greater visceral manipulation and multiple anastomoses, leading to a more substantial visceral pain component. These procedural differences may influence the relative performance of somatic versus mixed-visceral regional techniques.
This research has shown that both blocks have comparable analgesic profiles as evidenced by the comparable results with regard to rescue analgesia, pain scores, incidence of postoperative nausea and vomiting, and intraoperative hemodynamics. The number of doses of rescue analgesia, when required, were also comparable in the two groups.
To the best of our knowledge, this is the first study to test ESP block and L-TAP block in a head-to-head comparison in bariatric population. Elshazly et al, carried out an RCT comparing the effects of ultrasound-guided TAP block with that of Erector Spinae block over 60 patients undergoing laparoscopic bariatric surgeries. The results reported higher pain scores in the first 24h in the TAP group with time to first rescue analgesia being greater with the ESP block. These results differed from ours and the difference between the two studies could be explained by the larger sample size in our study (96 Vs 60 patients). Another explanation could be the broader tissue infiltration in the laparoscopic-guided TAP approach compared to the ultrasound-guided counterpart (8).
Previous reports comparing the two blocks in other surgical procedures showed that erector spinae plane block was superior to TAP block in laparoscopic hysterectomy (9), laparoscopic cholecystectomy (10), open ovarian surgery (11); this differed from our results; however all the available data used the ultrasound-guided approach in the two blocks and this might explain the different results between our study and all previous studies.
Table 3 - Other outcomes. Data are presented as mean (standard deviation), median (quartiles), and frequency (%).
Postoperative pain management in obese population undergoing bariatric surgery remains a daunting challenge. Being more prone to respiratory depression and obstructive sleep apnea, the employment of the conventionally-used opioid analgesia increases the risk of complications in these patients. Other non-opioid systemic analgesics are also not devoid of complication such as renal impairment (with NSAIDs), cardiovascular depression (with dexmedetomidine). Nonetheless, poor postoperative pain control impairs adequate chest expansion in these patients, exposing them to another spectrum of postoperative pulmonary complications such as infection and atelectasis (2). Multi-modal analgesia regimens that employ regional anesthetic block techniques and rely less on narcotic analgesia become an indispensable addition to post-operative patient care. Our results showed that neither of the two blocks, namely laparoscopic TAP and erector spinae plane blocks, was superior in patients with obesity. Thus, we suggest that the choice of the appropriate block should be individualized according to the preference and expertise of the surgical and anesthetic team as well as the logistic facilities in the operating theatre.
Our study had a few limitations: it was performed in a single center. We included a case-mix of sleeve
gastrectomy and bypass surgeries. Research for each subgroup of patients is warranted in the future. The study focused on the obese population and the comparison in other groups of patients might produce different results.
CONCLUSION
In conclusion, the two blocks, L-TAP and ESP block showed comparable analgesic and hemodynamic
profile in obese population undergoing laparoscopic bariatric surgery.
Author’s Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ahmed S Abdallah, Ahmed Khaled Abdelaziem, Ahmed Fahmy Omar and Mohannad Aly Fayed. The first draft of the manuscript was written by Ahmed Hasanin and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest and Source of Funding
The authors have no relevant financial or non-financial interests to disclose. No funding was received for conducting this study.
Ethics Approval
Approved by the Research Ethics Committee, Faculty of Medicine, Cairo University. Code: MD-292-2022.
REFERENCES
1. Garimella V, Cellini C. Postoperative pain control. Clin Colon Rectal Surg. 2013;26(3):191-6.
2. Alvarez A, Singh PM, Sinha AC. Postoperative analgesia in morbid obesity. Obes Surg. 2014;24(4):652-9.
3. Magee C, Clarke C, Lewis A. Laparoscopic TAP block for laparoscopic cholecystectomy: description of a novel technique. Surgeon. 2011;9(6):352-3.
4. Forero M, Ayala A, Vega MF, et al. Erector spinae plane block: a new ultrasound-guided regional anesthesia technique for post-thoracotomy pain. Reg Anesth Pain Med. 2016;41(2):159-68.
5. Huang J, Liu JC. Ultrasound-guided erector spinae plane block for postoperative analgesia: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020;20(1):83.
6. Chan YH. Biostatistics 102: quantitative data--parametric & non-parametric tests. Singapore Med J. 2003;44(8):391-6.
7. Chan YH. Biostatistics 103: qualitative data - tests of independence. Singapore Med J. 2003;44(10):498-503.
8. Elshazly M, El-Halafawy YM, Mohamed DZ, Wahab KAE, Mohamed TMK. Feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial. Korean J Anesthesiol. 2022; 75(6):502-509.
9. Warner M, Yeap YL, Rigueiro G, Zhang P, Kasper K. Erector spinae plane block versus transversus abdominis plane block in laparoscopic hysterectomy. Pain Manag. 2022;12(8):907-916.
10. Ozdemir H, Araz C, Karaca O, Turk E. Comparison of Ultrasound-Guided Erector Spinae Plane Block and Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia after Laparoscopic Cholecystectomy: A Randomized, Controlled Trial. J Invest Surg. 2022;35(4):870-877.
11. Abdullah S, Elshalakany N, Farrag Y, Abed S. The use of erector spinae versus transversus abdominis blocks in ovarian surgery: A randomized, comparative study. Colomb. J. Anesthesiol. 2022;50:e1025.
12. Huang J, Liu JC. Ultrasound-guided erector spinae plane block for postoperative analgesia: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020;20(1):83.
13. Ruiz-Tovar J, Gonzalez G, Sarmiento A, Carbajo MA, Ortiz-de-Solorzano J, Castro MJ, et al. Analgesic effect of postoperative laparoscopic-guided transversus abdominis plane (TAP) block, associated with preoperative port-site infiltration, within an enhanced recovery after surgery protocol in one-anastomosis gastric bypass: a randomized clinical trial. Surg Endosc. 2020; 34(12):5455-5460.
14. Zaghiyan KN, Mendelson BJ, Eng MR, Ovsepyan G, Mirocha JM, Fleshner P. Randomized clinical trial comparing laparoscopic versus ultrasound-guided transversus abdominis plane block in minimally invasive colorectal surgery. Dis Colon Rectum. 2019;62(2):203-210.
Full Text Sources:
Abstract:
Views: 1162

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.