Surgery, Gastroenterology and Oncology

|
|
Left isomerism (IS), also known as polysplenic syndrome, is part of the category of heterotaxic syndromes. Heterotaxic syndrome is a general term that describes the abnormal positioning of the viscera in the chest and abdomen. Signs of polysplenic syndrome include: bilobed lungs, liver located on the median line, but also intestinal malrotation. The prevalence of this condition is 1.4 patients per 10,000 children. The clinical aspect is closely correlated with the specific pathology of polysplenism. Apparently, incidental signs and symptoms are encountered, unexplained and unassociated from the etiopathogenic point of view, until the imaging examination that elucidates the causes of the observed clinical picture. As such, polysplenism, i.e., left isomerism, is the result of the abnormal development of the asymmetry of the laterality of the organs having the effect of situs ambiguus.
INTRODUCTION
The first anatomical-clinical description of this type of pathology was made by Helwig EB in 1929 as a type of situs ambiguus characterized by left isomerism, associated with a group of visceral anomalies of unknown etiology, which includes the presence of splenic nodules outliers (1). The term left isomerism (IS) would include a group of morphological variations that cause part of the internal organs to be located to the right side of the midline with their tendency to adopt characteristics of those of the same name on the left side (2). The anomalies considered part of the ubiquitous polysplenism syndrome (PSS) in almost all cases, in addition to the splenic ones, are those of cardiac malformations, thickening and interruption of the vena cava with continuity to the azygos vein, and abdominal heterotaxy. With inconsistency of cases, however, pancreatic abnormalities are also reported, such as shortening of the length of the body of the pancreas, accompanied by hypoplasia associated with preduodenal transposed portal vein and pulmonary and genitourinary malformations (3).
CASE REPORT
We present the case of a 3-year-old patient who presented to the medical unit with a two-day history of abdominal pain. We did not have the medical history available at the time of the imaging examination. The blood tests revealed an important increase in leukocytes. The imaging investigations were required to mainly eliminate the diagnosis of appendicitis.
RESULTS
In the CT (computed tomograph) examination with contrast material, the following can be observed: the absence of the horizontal cleft in the right lung with the appearance of a bilobed lung, the liver located on the median line with an asymmetrical appearance and with the left lobe more voluminous than the right one, cholecyst located on the median line, multiple round-oval structures with tissue densities are highlighted in the left hypochondrium, having a morphology and uptake of contrast substance compatible with the splenic parenchyma. (figs. 1-4). What should be noted, however, is the interruption of the continuity of the inferior vena cava, its lower portion being continued by the azygos vein but also intestinal malrotation. We mention that in the absence of specific investigations, we did not fully evaluate the changes at the cardiac level.
Figure 1 - Liver aspects

Figure 2 - Splenunculi

Figure 3 - Abdominal aspects
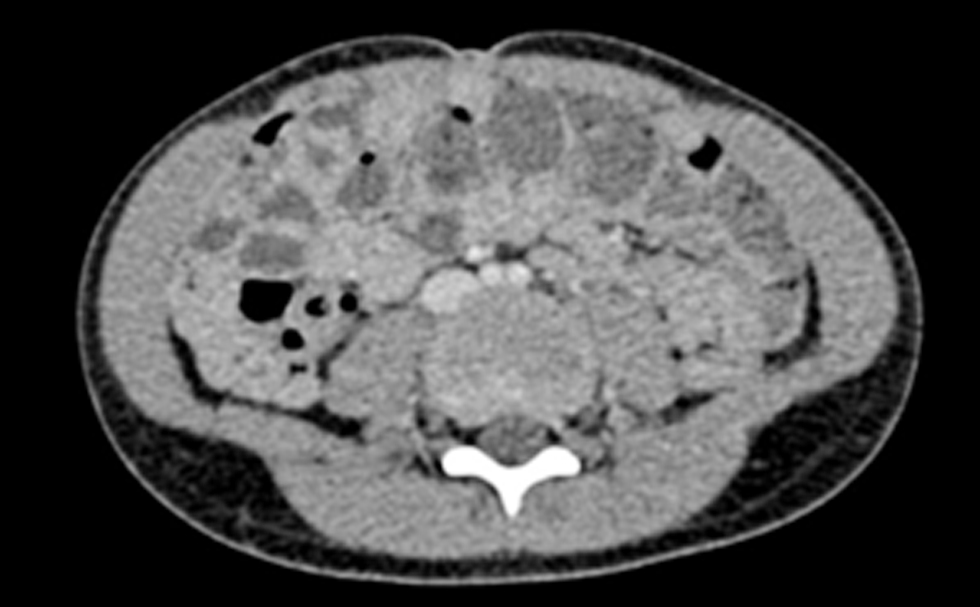
Figure 4 - Pulmonary aspects

DISCUSSIONS
Polysplenia (IS) can lead to pathogenic abnormalities of internal organs, in some cases a large number of accessory spleens and splenic nodules being reported, with apparently inexplicable clinical presentation and pseudo-chaotic association of semiological phenomena (4). This fact can be a factor of unpredictability in the case of emergency surgery, especially due to the association of gastric dextroposition, a liver located medially or in the left hypochondrium; at the same time, the agenesis of the celiac trunk, the origin of the hepatic artery at the level of the superior mesenteric artery, the swelling of the hepatic veins at the level of the right atrium, but also cardiac abnormalities such as hypertrophy and lipomatosis of the interatrial septum can predispose these patients to organ pathologies at an early age (5). Usually, most cases (40%) are discovered by adulthood, they manage to pass the age of 2 years this majority dying before 5 years. Only a small proportion of patients (5-10%) without clinically and prognostically significant cardiac lesions reach adulthood (6). Due to the non-specificity of the clinical picture, the radiological examination becomes a gold standard for diagnosis. Thus, it is unanimously accepted that to confirm a diagnosis of PS the presence, in addition to the defining one, i.e., polysplenia, of at least one anomaly of the situs ambiguus or situs inversus type. In most cases, nodular and accessory spleens are located along the greater gastric curvature to the right of the midline, being the only explanation for intestinal malrotation. In the case described by us, the arrangement of the accessory spleens was made atypical with a predominantly medial orientation. However, our case is placed in a group of other situations described in the literature with the hepatobiliary system located on the midline, hypoplasia of the inferior vena cava that continues with the azygos or hemiazygos vein (7).It seems that all these types of abnormalities, alone or grouped, are representative of PS, but none of them are pathognomonic. Extra-abdominal anatomical anomalies include cardiac defects, disappearance of pulmonary clefts with bilobation of the lungs and agenesis - renal hypoplasia, duplication of the pyelocaliceal system (8). Possible intraoperative accidents of the preduodenal portal vein in certain intercurrent surgical interventions are to be expected, as this type of interventional incident has already been reported in the literature.
CONCLUSIONS
The final diagnosis has been made by using imaging methods: polypsplenism syndrom – left isomerism, which associates: intestinal malrotation, bilobed lung, the liver and the gall bladder are lying on the midline and interruption of the inferior vena cava.
Conflict of interest
All authors declare that they have no conflict ofinterest.
Funding
No funding sources.
Ethical statement
Written informed consent was obtained from the patient of this case report.
REFFERENCES
1. Vaughan TI, Hawkins LP, Elliot LP. Diagnosis of polysplenia syndrome. 1971;101(3):511-8.
2. Gayer G, Apter S, Jonas T, Amitai M, Zissin R, Sella T, et al. Polyspenia syndrome detected in adulthood. Report of eight cases with review of the literature. Abdom Imaging. 1999;24(2):178-84.
3. McIlhenny J, Campbell SE, Raible RJ, Antaki GM. Pediatric case of the day. Biliary atresia and polysplenia syndrome. AJR Am J Roentgenol. 1996;167(1):269, 271-3.
4. Yoon S. Fischer's Mastery of Surgery, Sixth Edition. Ann Surg. 2012;4(256):669.
5. Latha GA, Kagali NA, Shridhar M, Prasad BSS. Preduodenal portal vein in adult with polysplenia syndrome revisited with a case report. Indian J Surg. 2014;76(2):137-42.
6. Abramson SJ, Berdon WE, Altman RP, Amodio JB, Levy J. Biliary atresia and non cardiac polisplenic syndrome: US and surgical considerations. Radiology. 1987;163(2):377-9.
7. Sener RN, Alper H. Polysplenia syndrome: a case associated with transhepatic portal vein, short pancreas anf left inferior vena cava with hemiazygous continuation. Abdom Imaging. 1994;19(1):64-6.
8. Plata-Muñoz JJ, Hernández-Ramírez D, Anthón FJ, Podgaetz E, Avila-Flores F, Chan C. Polysplenia syndrome in the adult patient. Case report with review of the literature. Ann Hepatol. 2004;3(3): 114-7.
Full Text Sources:
Abstract:
Views: 6411

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.