Surgery, Gastroenterology and Oncology

|
|
Liver transplantation is an option for patients with genetic metabolic diseases, including familial hypercholesterolemia. We report now the results of a domino liver transplantation (DLT) performed 23 years ago: the domino donor was a 25-year-old female with familial hypercholesterolemia (that had failed medical therapies for FH). She received the right hemiliver and segment I and IV from a cadaveric donor (segments II and III were transplanted to a child with type I glycogenosis), while the liver of the patient with familial hypercholesterolemia was transplanted to a 46-year-old patient with hepatocellular carcinoma (HCC), non responses at chemoembolization, and advance HBV cirrhosis. 23 years after the transplant, both patients are still alive. The domino recipient has no reccurence of hepatocellular carcinoma. She developed a less severe hypercholesterolemia and the medical treatment prevented the development of atheromas on the coronaries and carotides arteries. Ttherefore the patient had a postoperative normal life. DLT using a liver graft from a donor with FH coud be an option for selected marginal recipient.
Case report
Liver transplantation is the therapeutic option for patients with terminal liver disease, but also for patients with genetic metabolic diseases, including familial hypercholesterolemia.
The increasing demand for liver grafts is indeed a significant issue in the field of organ transplantation due to the large number of patients with terminal liver disease on the waiting list. This has led to a large shortage of organs for transplantation.
In order to overcome the discrepancy between the limited number of donors and the large number of patients waiting for a hepatic graft, marginal grafts are being used more and more.
Domino liver transplantation (DLT) means using the liver that has been explanted from one recipient as a graft for another recipient. The most common indication is familial amyloidosis while familial hyper-cholesterolemia is a very rare indication (1).
The underlying rationale for accepting marginal livers is that the recipients are gradually exposed to specific metabolic conditions (2,3) without immediate adverse effects. For instance, since the progression of the donor's disease may take years, it is believed that the recipient's life expectancy will likely not extend long enough for him to develop the complications associated with the donor’s metabolic disorder.
In our case the recipient had a long survival, without, however, developing a severe form of the donor’s disease.
The domino transplantation was performed in 2001 and reported in 2003 (4) and a follow up study was published in 2007(5).
We report now the result of the same patients, donor and recipient, after 23 year since the operation, which was, actually a combined split and domino liver transplantation. The child that received the segments 2-3 of a normal liver from a cadaveric donor died in the postoperative period due to septic complications, while the recipient of the rest of the normal liver, namely segments 1, 4 and 5-8 (a patient with familial hyper-cholesterolemia) survived in the long run; on the other hand, her liver was used for a patient with terminal liver cirrhosis and liver cancer with no response to chemo-embolization). The whole procedure was described in detail in the article previously published (4).
Briefly, a 25-year-old patient with familial hypercholesterolemia received the right hemiliver and segment I and IV from a cadaveric donor (segments II and III were transplanted to a child with type I glycogenosis), while the liver of the patient with familial hypercholesterolemia was transplanted to a 46-year-old patient with hepatocellular carcinoma (HCC) grafted on HBV cirrhosis.
The decision to have a domino transplant in the HCC patient was made understanding that, in the absence of transplantation, the patient's survival time would have been significantly reduced compared to the scenario in which the patient had received a liver from a patient with familial hypercholesterolemia. On the other hand, we reasoned that an HHC patient whose illness progressed after embolization would not have had enough post-transplant survival rate to develop serious cardiovascular disease after receiving a liver from the patient with familial hypercholesterolemia.
23 years after the transplant, both patients are still alive; therefore, we thought an update on this case was deemed highly pertinent by us.
Domino liver donor
Following transplantation, total and low-density lipoprotein cholesterol levels quickly returned to
normal and are still normal (172 mg/dL as of February 2024).
Following liver transplantation, right coronary artery stenting was necessary at one- and two-years post-transplantation due to cardiovascular disease - coronary atheromatosis. Furthermore, two years following liver transplantation, renal function kept declining until renal failure required renal replacement through dialysis. The patient had a kidney transplant in 2004. Both the hepatic and renal grafts are currently functioning (creatinine 1.7 mg/dL). Imaging reveals atrophic native kidneys. Renal graft: 118 mm long shaft, 21 mm renal parenchymal thickness, and greater cortical scarring. There are both excretory and secretory functions.
Cardiovascular disease has become worse. In 2003, the patient had minor aortic stenosis, but currently, the coronary CT angiography (CCTA) pre-transcatheter aortic valve implantation procedure identified severe aortic stenosis and concentric hypertrophic cardio-myopathy. Coronary arteries have a calcium score of 406; CCTA indicates right coronary dominance. There were no substantial stenoses, with a maximum of 30% at the right coronary artery origin and 5-10% at the left coronary trunk and anterior descending.
Currently she is in good condition and she lives a normal life.
Domino liver recipient
Cholesterol levels increased around 2 weeks after liver transplantation. The original hypocholesterolemic medication consisted of simvastatin 60 mg/day, which was later changed with atorvastatin 80 mg daily. The total cholesterol level remained over 300 mg/dl.
In the third year following the Domino liver transplant, an autologous stem cell transplant CD 34 was conducted to improve hypercholesterolemia management. Although the treatment went smoothly, there was no reduction in total or LDL cholesterol levels.
Ezetimibe 10 mg/day was used as hypocholesterolemic medication, resulting in partial control of total cholesterol and LDL levels.
The patient is currently taking 40 mg of rosuvastatin and 30 mg of ezetimibe daily. Despite inadequate medical monitoring of total and LDL cholesterol levels, even after 20 years of domino transplantation with a donor from a patient with essential hypercholesterolemia, minor cardiovascular alterations were observed.
Thus, in 2008, invasive coronarography was conducted, which revealed no coronary abnormalities.
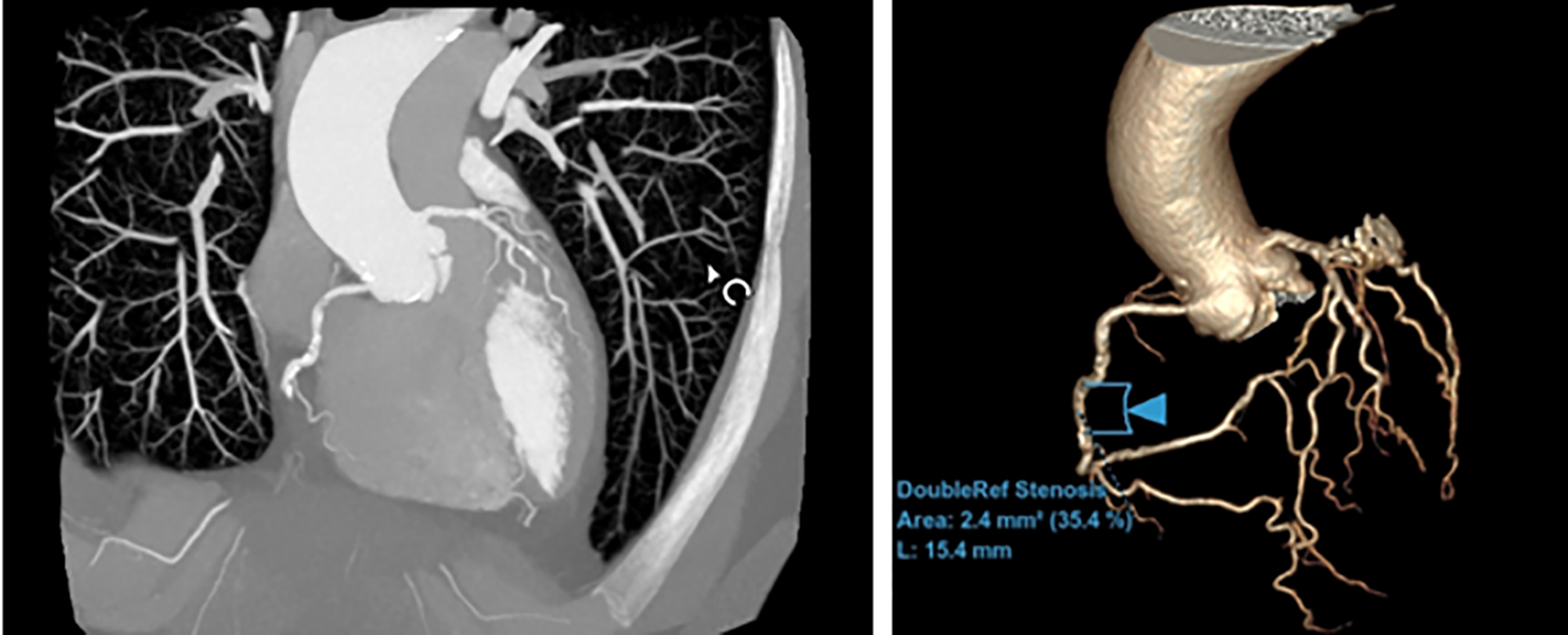
Due to the patient's lack of cardiovascular symptoms, coronary angiography was discontinued. Instead, CCTA scans of the coronary arteries were conducted in 2014, 2018, and April 2024. CCTA can evaluate coronary artery calcium score and rule out coronary arteries disease which showed insignificant coronary lesions.
CCTA images performed in April 2024
In 2014 the first Doppler ultrasound evaluation revealed carotid stenosis of less than 50% and right
vertebral artery occlusion, which clinically has no hemodynamic repercussions, as it means there are no substantial restrictions in blood flow. Recent Doppler evaluations show that the degree of carotid stenosis has remained stable, indicating that there have been no changes or worsening in the condition over time.
From a liver graft standpoint, we mention biliary anastomosis stenosis, for which a Roux-en-Y hepaticojejunostomy was performed in 2015 (14 years after liver transplant). Currently, immunosuppressive therapy consists of tacrolimus extended-release pills.
Twenty years after the liver transplant, the patient developed type II diabetes, which is treated with glicazidum 60 mg daily.
The patient currently has no recurrence of hepatocellular carcinoma, and liver function tests are normal.
Figure 1 - Maximum intensity projection (MIP) image of the coronary arteries (left panel). 3D reconstruction of the coronary arteries (right panel).
Discussion
Familial hypercholesterolemia (FH) is an autosomal dominant metabolic disorder caused by defects in the LDL receptor (LDLR) gene, which is the most common; mutations in the APOB (Apolipoprotein B) or PCSK 9 (proprotein convertase subtilisin/kexin type 9) gene are less common (6). It is a rare disorder, with an incidence of approximately 1 in 1 million for the homozygous type and 1 in 500 to 1 in 200 for the hetherozygous variant.
In the homozygous variant, cholesterol levels can exceed 800mg/dL, resulting in severe atherosclerotic disease from childhood (7). Current pharmaceutical treatment and repeated plasmapheresis procedures are insufficient to control the condition.
Given that the liver contains approximately 75% of all LDL receptors, liver transplantation has been proposed as a unique therapeutic option for familial hypercholesterolemia patients, particularly for children with homozygous familial hypercholesterolemia who do not respond to maximal lipid-lowering therapy, despite the fact that this is not included in most hypercholesterolemia treatment guidelines (8-12).
Domino Liver Transplantation is an option for expanding the donor pool in certain instances, such as people with familial hypercholesterolemia.
According to the Domino Liver Registry (http://www.fapwtr.org/index.htm), 1254 domino transplants were done in 1234 patients in 66 transplant centers in 21 countries (including Romania) until December 31, 2017 (11).
Our domino transplant case was the first one published in 2003, and was followed by a few more (12-16).
The donor for the domino transplant had hyper-cholesterolemia and coronary heart disease prior to liver transplantation. Cardiovascular disease has advanced, however slowly.
Our donor for the domino transplant with hyper-cholesterolemia already had coronary heart disease when she underwent liver transplantation. Cardio-vascular disease has progressed, but more slowly.
Regarding the domino recipient, it developed atherosclerotic cardiovascular disease caused by hypercholesterolemia, but much slower.
The pathophysiological basis of this technique is that patients with familial hypercholesterolemia have a deficiency of LDL receptors. These receptors are present mostly in the liver, but also in the rest of the body's tissues and organs. A patient with the condition will have a shortage of receptors in both the liver and the rest of the organs and tissues, necessitating a liver transplant. On the other hand, the recipient of a poor liver would develop the condition, but not of the same extent as the donor, because to peripheral tissue receptors. The rule is to choose cancer patients as recipients because the projected survival of these individuals does not exceed 4-5 years.
These theoretical assumptions were proven valid in our circumstance. Except for the recipient's survival, the cancer did not reoccur allowing us to track her for 23 years.
The donor of the hypercholesterolemic liver is likewise still alive, so we could study her for the same amount of time.
Even though the donor's cholesterol corrected after getting a normal liver, the atheromas did not go away, and she needed a kidney transplant and a coronary stent.
Although the recipient's cholesterol levels stay high while on medication, the vascular implications may be judged "acceptable".
We consider that the domino liver recipient's metabolic syndrome and mild cardiovascular illness are consistent with the expected progression of a liver transplant recipient 20 years after transplant. The patient acquired hypercholesterolemia problems, although these can still be managed with medication.
Our domino receptor lives 23 years after transplant, considerably beyond the projected survival time for a donor graft patient with hereditary hypercholesterolemia.
This supports the concept that the loss of LDL receptors in the liver is compensated for by peripheral LDL receptors, bringing atherosclerotic disease under control.
Conflict of interest
All authors declare that they have no conflict of interest.
References
1. Geyer ED, Burrier C, Tumin D, Hayes Jr D, Black SM, Washburn WK, et al. Outcomes of domino liver transplantation compared to deceased donor liver transplantation: a propensity-matching approach. Transpl Int. 2018;31(11):1200-1206.
2. Herlenius G, Wilczek HR, Larsson M, Ericzon BG, on behalf of reporting members of the familial amyloidotic polyneuropathy world transplant registry. Ten years of international experience with liver transplantation for familial amyloidotic polyneuropathy: results from the familial amyloidotic polyneuropathy world transplant registry. Transplantation. 2004;77(1):64-71.
3. Kitchens WH. Domino-liver transplantation: indications, techniques, and outcomes. Transplant Rev (Orlando). 2011;25(4):167-77.
4. Popescu I, Simionescu M, Tulbure D, Sima A, Catana C, Niculescu L, et al. Homozygous familial hypercholesterolemia: specific indication for domino liver transplantation. Transplantation. 2003;76(9): 1345-50.
5. Popescu I, Habib N, Dima S, Hancu N, Gheorghe L, Iacob S, et al. Domino liver transplantation using a graft from a donor with familial hypercholesterolemia: seven-yr follow-up. Clin Transplant. 2009;23(4):565-70.
6. Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science. 1986;232(4746):34-47.
7. Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32): 2459-2472.
8. Martinez M, Brodlie S, Griesemer A, Kato T, Harren P, Gordon B, et al. Effects of liver transplantation on lipids and cardiovascular disease in children with homozygous familial hypercholesterolemia. Am J Cardiol. 2016;118(4):504-10.
9. Mansoorian M, Kazemi K, Nikeghbalian S, Shamsaeefar A, Mokhtari M, Dehghani SM, et al. Liver transplantation as a definitive treatment for familial hypercholesterolemia: a series of 36 cases. Pediatr Transplant. 2015;19(6):605-11.
10. Alim A, Tokat Y, Erdogan Y, Gokkaya Z, Dayangac M, Yildiray Y, et al. Liver transplantation for homozygote familial hypercholesterolemia: the only curative treatment. Pediatr Transplant. 2016;20(8):1060-1064.
11. Mlinaric M, Bratanic N, Dragos V, Skarlovnik A, Cevc M, Battelino U. Liver transplantation in homozygous Familial Hypercholesterolemia (HoFH) - Long term Follow -Up of a Patient and Literature Review. Front Pediatr. 2020;8:567895.
12. Dubayee MA, Kayikcioglu M, Roeters van Lennep J, Hergl N, Mata P. Is Liver Transplant Curative in Homozygous Familial Hypercholesterolemia ? A Review of Nine Global Cases. Adv Ther. 2022; 39(6):3042-3057.
13. Zhou GP, Sun LY, Zhu ZJ. The concept of “domino” in liver and hepatocyte transplantation. Therap Adv Gastroenterol. 2020;13: 1756284820968755.
14. Liu C, Niu D-M, Loong C-C, Hsia C-Y, Tsou M-Y, Tsai H-L, et al. Domino liver graft from a patient with homozygous familial hyper-cholesterolemia. Pediatr Transplant. 2010;14(3):E30-3.
15. Golbus J R, Farhat L, Fontana RJ, Rubenfire M. Rapidly progressive atherosclerosis after domino liver transplantation from a teenage donor with homozygous familial hypercholesterolemia. J Clin Lipidol. 2017;11(5):1284-1288.
16. Sambommatsua Y, Brunoa DA, Imaia D, Leea SD, Khana AA, Sharmaa A, et al. Domino Liver Transplantation for Unresectable Colon Cancer Liver Metastasis From a Donor With Heterozygous Familial Hyperlipidemia: A Case Report. Transplant Proc. 2023; 55(8):1930-1933.
Full Text Sources:
Abstract:
Views: 2579

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.