Surgery, Gastroenterology and Oncology

|
|
Objective: to evaluate the outcomes of laparoscopic distal gastrectomy with D2 lymph node dissection as a treatment for advanced gastric cancer in three major hospitals in Hanoi, Vietnam.
Material and Methods: a retrospective study was conducted on patients with advanced gastric cancer who underwent laparoscopic distal gastrectomy with D2 lymph node dissection between January 2017 and December 2021.
Results: a total of 119 patients were included in the study, consisting of 85 males and 34 females. All patients had cancer located in the lower third of the stomach. The majority of patients were staged T3 (67.23%) and N1 (56.30%) before surgery. The surgical success rate was 97.48%, with four patients experiencing complications during the operation and three requiring conversion to open surgery. The average operation time was 221.58 minutes. The average number of dissected lymph nodes was 21.54, and the rate of patients with lymph node metastasis was 60.36%. Nine patients (7.76%) experienced postoperative complications, with four patients (4.45%) suffering from serious complications. The average postoperative hospital stay was 11.66 days. The average disease-free survival time was 53.26 months, with a disease-free survival rate of 77.7% at three years and 62.0% at five years. The overall survival time was 58.33 months, with an overall survival rate of 83.9% at three years and 69.9% at five years.
Conclusion: laparoscopic distal gastrectomy with D2 lymph node dissection can be performed safely with favorable outcomes at three major hospitals in Hanoi, Vietnam. This procedure contributes to improving the quality of cancer care for gastric cancer patients in Hanoi.
INTRODUCTION
According to GLOBOCAN 2020 statistics, stomach cancer ranks 6th among common cancers worldwide, with over one million new cases and an incidence rate of 11.1 per 100,000 people. The mortality rate from stomach cancer ranks 3rd, accounting for 768,793 deaths annually (1). In Vietnam, stomach cancer is quite common, ranking 4th in incidence and 3rd in mortality, following liver cancer and lung cancer. Surgery remains the most important treatment method for stomach cancer, especially at stages where tumors are resectable. Other treatment modalities, such as chemotherapy, radiation therapy, and targeted therapy, play significant roles at specific stages. These methods can help improve surgical outcomes, increase the complete resection rates - such as with adjuvant chemotherapy - or prolong survival after surgery, as seen with radiation therapy and targeted therapy (2).
Since 1994, Japanese surgeons have been performing laparoscopic gastrectomy, and the use of laparoscopic surgery in the treatment of gastric cancer has significantly progressed. Studies have demonstrated that laparoscopic gastrectomy presents more advantages over traditional open surgery, providing a safe approach with fewer complications while adhering to the principles of cancer treatment and achieving similar oncological outcomes (3-5).
However, the complexity of laparoscopic gastrectomy for treating stomach cancer necessitates skilled surgeons with extensive experience in gastric cancer surgery and proficient laparoscopic techniques. Additionally, many modern medical devices required for this procedure can be expensive and may exceed the financial capabilities of patients. Unfortunately, many health insurance policies do not cover these devices in hospitals. Consequently, laparoscopic gastrectomy is not widely promoted across the country but is implemented primarily in a few esteemed medical facilities.
Thanh Nhan Hospital, E Central Hospital, and Hanoi Medical University Hospital are the three major
hospitals in Hanoi, Vietnam, where hundreds of patients with stomach cancer receive treatment annually. All three hospitals have been utilizing this technology since 2014; however, it was not until 2017 that laparoscopic gastrectomy, along with D2 lymph node dissection for advanced gastric cancer, was standardized in accordance with the Japanese Gastric Cancer Association's guidelines (6,7). Therefore, this study aims to evaluate a cohort of patients with advanced gastric cancer who underwent laparoscopic distal gastrectomy with D2 lymph node dissection in accordance with the Japanese Gastric Cancer Association's guidelines at the three aforementioned hospitals from January 2017 to December 2021.
MATERIAL AND METHODS
This is a retrospective study conducted on a group of patients with non-metastatic gastric epithelial
cancer. The inclusion criteria required histologically confirmed gastric epithelial cancer patients who underwent laparoscopic distal gastrectomy and D2 lymphadenectomy at Hanoi Medical University Hospital, E Central Hospital, and Thanh Nhan Hospital from January 2017 to December 2021. The exclusion criteria consisted of patients with recurrent gastric cancer, non-epithelial cancers, and metastatic cancers from other sites.
The study parameters encompassed general characteristics, including patient numbers, age, gender, BMI, ASA score, TNM staging before surgery, tumor location, anemia status, and CEA levels. Surgical results included surgical technique, anastomotic technique, blood loss during surgery, operation time, intra-operative complications, cases of conversion to open surgery, postoperative recovery time, postoperative complications, and any chemotherapeutic treatment following surgery. Pathological results consisted of the number of lymph nodes examined, the number of metastatic lymph nodes, postoperative TNM classification, post-operative cancer stage, histological differentiation, and the width of resected margins. Follow-up results included the number of remaining patients, the length of the disease-free period, and survival rates. All patients in our study provided written informed consent, and the study was approved by the Ethics Committee of Hanoi Medical University, Vietnam (Decision No. 4889/QD-DHYHN, dated October 21, 2022).
Statistical Analysis
Data were analyzed using SPSS version 26.0 (IBM, New York, USA). Mean values are presented as mean ± standard deviation, and proportions are expressed as percentages. Time and survival rates after surgery were calculated using the Kaplan-Meier curve. Appropriate statistical tests were employed for each type of variable to examine relationships between research variables.
RESULTS
A total of 119 stomach cancer patients met the selection criteria for the study and were selected from three medical centers. The characteristics of the patients before surgery are detailed in table 1.
All 119 patients were scheduled to undergo laparoscopic distal gastrectomy and D2 lymph node dissection. Among them, 116 patients (97.48%) successfully underwent the procedure. However, 4 patients (3.36%) experienced complications during surgery. Specifically, one patient had a minor complication involving damage to the large bowel muscle, which was sutured laparoscopically. Three patients faced serious complications that necessitated conversion to open surgery for further treatment. One patient required open colectomy due to an injury to the middle colonic artery, another underwent open splenectomy following a splenic injury, and the third patient experienced bleeding from the left gastric artery during lympha-denectomy, requiring open surgery to control the hemorrhage. The surgical outcomes for the 116 patients who successfully underwent laparoscopic distal gastrectomy are described in detail in table 2.

All cases successfully re-established gastrointestinal flow via a Billroth II anastomosis, with immediate biopsies performed on the specimens prior to the anastomosis. The results revealed no malignant cells in either the upper or lower sections of the gastric specimens. Subsequently, all specimens were sent to the pathology department for examination by pathology technicians. The pathological results for the 116 patients who successfully underwent laparoscopic distal gastrectomy with D2 lymphadenectomy are detailed in table 3.
Table 3 - Histopathological outcomes

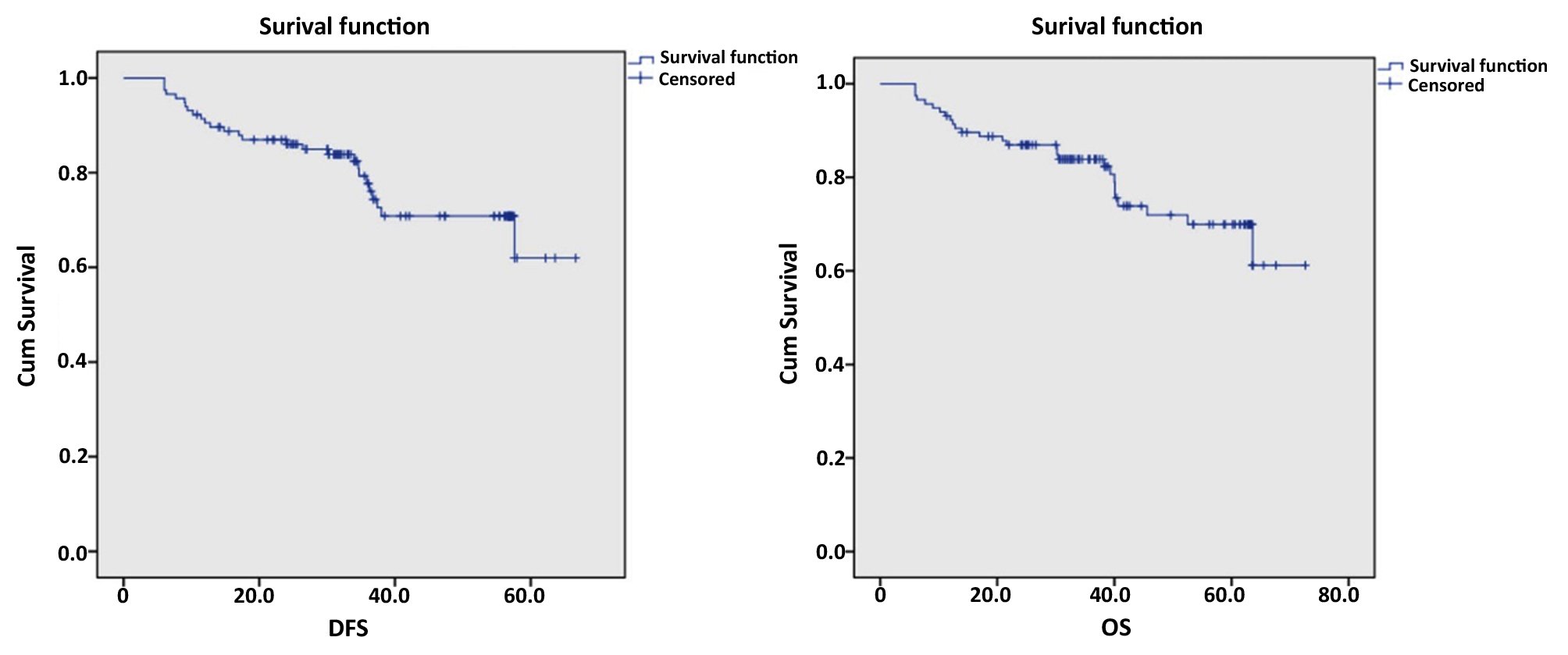
Among the 116 patients who underwent successful laparoscopic surgery, 89 were still alive at the end of the study, while 27 had died. Utilizing methods to calculate survival rates at different time points and establishing the Kaplan-Meier survival curve, we determined that the average disease-free survival time was 53.26 ± 2.21 months. The cumulative disease-free survival rates were 90.5% at 1 year, 87.0% at 2 years, 77.7% at 3 years, 70.7% at 4 years, and 62.0% at 5 years.
The average overall survival time was 58.33 ± 2.36 months, with overall survival rates of 92.2% at 1 year, 86.9% at 2 years, 83.9% at 3 years, 71.9% at 4 years, and 69.9% at 5 years. Through statistical hypothesis testing, we found that the rates of recurrence and mortality during the follow-up period after surgery were closely related to lymph node metastasis and the post-operative disease stage (p < 0.0001).
Figure 1 - Disease-free survival and overall survival
DISCUSSION
In recent years, scientists have established that stomach cancer is a pathological condition primarily linked to infection, with H. pylori being identified as a significant causative agent. However, this hypothesis is not yet universally accepted. Additional factors that may contribute to the promotion of stomach cancer include smoking, alcohol consumption, and the intake of salt-preserved foods. Diets low in fresh fruits and vegetables and high in smoked fish, salted meats, and pickled vegetables are believed to elevate the risk of stomach cancer (2,8,9).
Vietnam ranks as one of the countries with a high incidence of stomach cancer within the Asian region. According to statistics from the World Health Organization, stomach cancer in Vietnam is the fourth most common cancer in terms of incidence and the third leading cause of cancer-related deaths for both genders (1,10). Recent reports indicate that the prevalence of H. pylori infection among the Vietnamese population is alarmingly high, especially within school environments, ranging from 65.6% to 87.7% (11-13). This, combined with smoking habits, alcohol consumption, and a diet rich in salt and fermented foods, has contributed to the elevated incidence of stomach cancer in Vietnam. In 2020, the World Health Organization reported 17,906 new cases of stomach cancer and 14,615 deaths out of a total population of 97.58 million (1,10,14).
As a developing country in Southeast Asia, Vietnam has seen significant improvements in social life, resulting in a notable enhancement in community health awareness. Scientific and technological advancements from developed countries, including breakthroughs in medicine, have been rapidly integrated. Recent years have witnessed extensive studies on gastric cancer, focusing on microbiological characteristics, causative factors, histopathology, and genetic aspects conducted by major research centers (11,13-16). These studies indicate that gastric cancer patients in Vietnam tend to be over 50 years old, with male patients exhibiting twice the incidence rate compared to female patients. In our study, conducted on 119 patients, the average age was 59.77 years, with male patients outnumbering female patients by more than twofold (85/34), reflecting similar trends seen in other studies within Vietnam and the region (17-19).
Noteworthy advancements in gastric cancer treatment in Vietnam include a shift from solely relying on surgical removal of the stomach to incorporating improved radiation therapy and targeted therapies. There is a strong emphasis on achieving complete resection during surgery. The use of laparoscopic surgery for gastric cancer treatment has rapidly advanced, with several studies published in international journals highlighting its efficacy (20).
In our study, the success rate of laparoscopic distal gastrectomy and D2 lymph node dissection was 97.48% (116/119 cases), with an average surgical time of 221.85 minutes, average blood loss of 98.81 ml, and an average of 21.54 lymph nodes removed. Among the 119 study participants, one case (0.92%) involved a minor complication treated laparoscopically, while three cases (2.75%) were serious complications that necessitated conversion to open surgery. Nine patients (7.76%) experienced postoperative complications, including four (3.45%) with serious complications requiring prolonged hospitalization through conversion to open surgery. Nevertheless, the surgeries were performed safely, with no postoperative deaths reported. These results align with recent reports on laparoscopic distal gastrectomy for gastric cancer (21,22). Although laparoscopic distal gastrectomy is a common surgical procedure in many countries, it remains complex and carries inherent risks of complications. With advancements in surgeons’ technical skills and continuous modernization of laparoscopic surgical instruments, the efficacy and safety of laparoscopic distal gastrectomy continue to improve.
Our study stands out as one of the few in Vietnam evaluating laparoscopic gastric resection for stomach cancer with a long enough follow-up period to provide insight into survival outcomes. A study assessing survival rates for 18 common cancers across 71 countries, encompassing 37,513,025 patients, revealed that the number of gastric cancer patients included in the report was 2,019,382 adults from 294 health facilities in 62 countries. The findings indicated considerable variation in 5-year survival rates for gastric cancer patients between countries and regions. Between 2010 and 2014, the 5-year survival rate was notably high in South Korea (69%) and Japan (60%), followed by Jordan (56%) and Costa Rica. In contrast, the 5-year survival rates ranged from 30-40% in 16 countries, including Canada, the USA, and several Asian and European nations, while survival rates below 20% were noted in countries like Chile, Ecuador, Thailand, and Bulgaria (23).
In our study, the disease-free survival rate was 77.7% after 3 years and 62.0% after 5 years. The overall survival rates were 83.9% and 69.9% after 3 and 5 years, respectively. When compared to survival rates from higher-performing countries, our findings appear comparable. However, given that our study was conducted after 2014, these conclusions should be interpreted with caution.
CONCLUSION
This multicenter study was conducted at three major hospitals in Hanoi, Vietnam. Our findings indicate that the long-term outcomes for patients with advanced stomach cancer who underwent laparoscopic distal gastrectomy are favorable. The results demonstrate that laparoscopic gastrectomy for advanced stomach cancer is effective regarding both surgical and oncological outcomes. This study provides valuable insights for readers and researchers regarding the outcomes of laparoscopic distal gastrectomy for advanced gastric cancer in a major city in Vietnam.
Conflict of interest: none.
REFERENCES
-
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249.
-
Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396(10251):635-648.
-
Ueda Y, Shiraishi N, Fujishima H, Kawasaki T, Ninomiya S, Shiroshita H, et al. Technical and oncological safety of laparoscopic gastrectomy for gastric cancer in elderly patients ≥ 80 years old. BMC Geriatr. 2022;22(1):475.
-
Zeng F, Chen L, Liao M, Chen B, Long J, Wu W, et al. Laparoscopic versus open gastrectomy for gastric cancer. World J Surg Oncol. 2020;18(1):20.
-
Yu J, Huang C, Sun Y, Su X, Cao H, Hu J, et al. Effect of Laparoscopic vs Open Distal Gastrectomy on 3-Year Disease-Free Survival in Patients With Locally Advanced Gastric Cancer: The CLASS-01 Randomized Clinical Trial. JAMA. 2019;321(20):1983-1992.
-
Japanese Gastric Cancer A. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20(1):1-19.
-
Japanese Gastric Cancer A. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. 2021;24(1):1-21.
-
Sano T. Gastric cancer: Asia and the world. Gastric Cancer. 2017; 20(Suppl 1):1-2.
-
Asaka M, Mabe K. Strategies for eliminating death from gastric cancer in Japan. Proc Jpn Acad Ser B Phys Biol Sci. 2014;90(7): 251-8.
-
International Agency for Research on Cancer. Population fact sheets. Available at: http://gco.iarc.fr/today/fact-sheets-populations.
-
Nguyen TL, Uchida T, Tsukamoto Y, Trinh DT, Ta L, Mai BH, et al. Helicobacter pylori infection and gastroduodenal diseases in Vietnam: a cross-sectional, hospital-based study. BMC Gastroenterol. 2010;10:114.
-
Che TH, Nguyen TC, Ngo DTT, Nguyen HT, Vo KT, Ngo XM, et al. High prevalence of Helicobacter pylori infection among school-aged children in Ho Chi Minh City, Vietnam. Int J Public Health. 2022; 67:1605354.
-
Binh TT, Tuan VP, Dung HDQ, Tung PH, Tri TD, Thuan NPM, et al. Advanced non-cardia gastric cancer and Helicobacter pylori infection in Vietnam. Gut Pathog. 2017;9:46.
-
Le HX, Truong DTT, Tran LB, Le PH, Duong Pham BU, Wada K, et al. A prospective cohort study on the association between waterpipe tobacco smoking and gastric cancer mortality in Northern Vietnam. BMC Cancer. 2022;22(1):803.
-
Nguyen NT, Dang NT, Dang QH, Tran VC, Vo HL, Masamitsu Yamaguchi, et al. Polymorphism of MUC1 gene in Vietnamese gastric cancer patients: A multicenter case-control study. Front Oncol. 2021;11:694977.
-
Phan DAT, Nguyen VT, Hua TNH, Ngo QD, Doan TPT, Nguyen ST, et al. HER2 Status and Its Heterogeneity in Gastric Carcinoma of Vietnamese Patients. J Pathol Transl Med. 2017;51(4):396-402.
-
Jin G, Lv J, Yang M, Wang M, Zhu M, Wang T, et al. Genetic risk, incident gastric cancer, and healthy lifestyle: a meta-analysis of genome-wide association studies and prospective cohort study. Lancet Oncol. 2020;21(10):1378-1386.
-
Sekiguchi M, Oda I, Matsuda T, Saito Y. Epidemiological trends and future perspectives of gastric cancer in Eastern Asia. Digestion. 2022;103(1):22-28.
-
Zhang CD, Yamashita H, Zhang S, Seto Y. Reevaluation of laparoscopic versus open distal gastrectomy for early gastric cancer in Asia: A meta-analysis of randomized controlled trials. Int J Surg. 2018;56:31-43.
-
Dang QA, Pham VT, Pham VD, Ha VQ, Dinh VC, Nguyen VH. Result of applying laparoscopic total gastrectomy with D2 lymph node dissection with left-site surgeon and final resection and closure of the duodenal stump in gastric cancer treatment. Surg Gastroenterol Oncol. 2020;25(4):199-205.
-
Zhang YX, Wu YJ, Lu GW, Xia MM. Systematic review and meta-analysis of totally laparoscopic versus laparoscopic assisted distal gastrectomy for gastric cancer. World J Surg Oncol. 2015;13:116.
-
Chittawadagi B, Nayak SK, Ramakrishnan P, Kumar S, Cumar B, Natarajan R, et al. Laparoscopic D2 gastrectomy in advanced gastric cancer: Postoperative outcomes and long-term survival analysis. Asian J Endosc Surg. 2021;14(4):707-716.
-
Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikši? M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018; 391(10125):1023-1075.
Full Text Sources:
Abstract:
Views: 3813

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.