Surgery, Gastroenterology and Oncology

|
|
Methods: A comprehensive online search was done using Pubmed, Web of Science, and the Cochrane library databases (2015 to 2020). Completed trials were identified at ClinicalTrials.gov. Meta-analysis data were conducted using a random effects model. Subset analysis of adenocarcinoma ‘s location and the usage of either categorical or continuous variables were performed.
Results: Five studies were included in the review, four of them in the meta-analysis. Analysis showed that, though not statistically significant (HR=0.88; 95% CI:0.74-1.04, p=0.13), a higher extension of the lymphadenectomy was associated with better OS, with evidence of significant heterogeneity (I2 = 86%, p<0.001). Both subset analysis of categorical variables and adenocarcinoma’s location revealed a survival benefit of a high lymph node yield on OS (HR=0.82; 95% CI: 0.69-0.98, p<0.05; HR=0.77; 95% CI: 0.68-0.88, p<0.001, respectively).
Conclusions: A higher extension of lymphadenectomy in a multimodal therapy approach might be associated with improved OS in EAC patients. Despite advances in multimodal therapy, extended lymphadenectomy should be the standard of care and the extension of lymph node resection is crucial as it might be a true prognostic factor that affects patients’ OS.
Key words: lymph node excision, neoadjuvant therapy, esophageal neoplasms, adenocarcinoma, survival
INTRODUCTION
Esophageal cancer is the seventh most diagnosed cancer and the sixth most common cause of death related to cancer worldwide, one in every eighteen cancer deaths in 2020 (1). The two most common histologic subtypes, squamous cell carcinoma (SCC) and adenocarcinoma, have different etiologies, resulting in a geographic variation of their incidence. In recent years, we have seen a significant and rapid increase in esophageal adenocarcinoma (EAC) incidence. Reasons are not entirely understood. It is thought that the increased prevalence of excess body weight and obesity, as well as gastroesophageal reflux disease, and the simultaneous decline in chronic Helicobacter pylori infection, might be behind it (2,3).
EAC arise from glandular epithelioma and are mainly located in the lower thoracic esophagus and esophagogastric junction, being associated with Barrett's esophagus. Gastroesophageal (GEJ) adeno-carcinomas behavior and staging modalities are similar to pure esophageal tumors (4). Therefore, these cancers are treated as EAC.
Esophageal cancer (EC) staging is defined by the 7th edition of the AJCC Cancer Staging Manual for esophagus and esophagogastric junction cancers that establishes tumor-node-metastasis (TNM) sub-classifications (5). EC location does not affect the EAC stage, as opposed to SCC (6). At time of diagnosis,
disease is usually in an advanced stage, and most patients have a poor prognosis (7).
EAC treatment has evolved, particularly in cases of early-stage disease. Surgical resection continues to be the standard treatment for localized disease, ensuring both locoregional disease control and long-term survival (8). In locally advanced EAC, poor survival with surgery alone has prompted the use of neoadjuvant chemotherapy or chemoradiation therapy in addition to surgery (multimodal therapy). Compared to surgery alone, multimodal therapy is associated with higher rates of negative resection margins, lower recurrence rates, and improved survival. However, EAC patients’ survival has improved little over the past decades and the estimated 5?year OS ranges from 36%-47% of patients in multimodal therapy strategies (9).
Eng et al, a study involving 4679 patients who received multimodal therapy for EAC, concluded that higher stage, lymphovascular invasion, and positive surgical resection margins were associated with decreased OS (10). Due to esophageal extensive submucosal lymphatic drainage, nearly 60% of patients have positive lymph nodes even after neoadjuvant chemoradiation therapy (11). Additionally, ‘skip metastasis’ directly metastasing into the second or third lymph node groups, are frequently seen in EAC (12). Nodal involvement is the single most important prognostic factor in EC for locoregional and systemic recurrences after complete resection (8). High-quality lymphadenectomy provides more accurate staging and improves OS. However, its value and extent during esophagectomy, as part of the multimodal therapy for EAC, is debatable.
Extending the surgical resection yield is considered reasonable to improve outcomes. Proponents of en bloc esophagectomy with extended lymphadenectomy claim lower recurrence rates and increased survival in patients with locally advanced tumors (13,14). The National Comprehensive Cancer Network recommends lymphadenectomy of at least 15 lymph nodes, with several studies demonstrating survival benefit with resections of up to 20-25 lymph nodes (15).
It has been suggested that a more extensive lymphadenectomy has higher post-operative morbidity with no survival advantage. Lack of statistical power in published studies together with heterogeneous cohorts of EC patients (EAC and SCC) contributes to ongoing debate (16).
Some studies reported a survival benefit of lymphadenectomy in EAC compared to SCC, potentially because the former is less likely to respond to neoadjuvant therapy. For this reason, the extension of
lymphadenectomy might have a more important effect in EAC patients OS (17).
This systematic review and meta-analysis was conducted to evaluate the impact of the extension of lymphadenectomy in OS of EAC patients submitted to esophagectomy preceded by neoadjuvant therapy.
MATERIALS AND METHODS
Literature search strategy
This study is reported in line with current PRISMA guidelines (18). However, the review was not registered, and a protocol was not elaborated.
To identify studies, a systematic literature search in electronic databases PubMed, Web of Science and Cochrane library was conducted. Searches were limited by language and publication date in order to meet inclusion criteria. The search terms included “esophageal”, “cancer”, “adenocarcinoma”, “esophagectomy”, “lymphadenectomy”, “neoadjuvant”, “survival” and “prognosis”. Search strategies were adapted to specific vocabulary in each database. Reference lists of previous reviews were scanned to track additional studies. Completed trials were identified at ClinicalTrials.gov. A full description of the search strategy is provided in supplementary table 1.
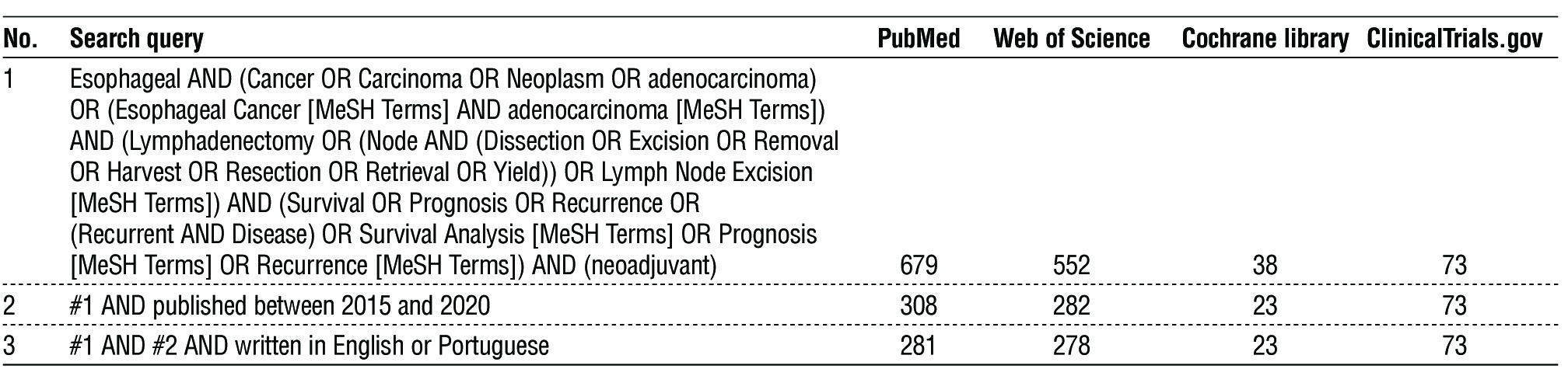
Supplementary Table 1 - Summary of search strategy and results as of March 9th , 2021. The query represented is an example based on the specifications required to Pubmed search. Adapted queries were used in the other databases mentioned taking into account their specific research criteria
Studies selection
After eliminating duplicates, each article’s title and abstract were independently reviewed by two authors to assess eligibility and full text of all potentially relevant articles was reviewed for inclusion. Any disagreement regarding study inclusion was solved by consensus or with a third reviewer consultation. Original articles included were randomized controlled trials or observational studies comparing the extent of lymphadenectomy in EAC patients submitted to esophagectomy preceded by neoadjuvant therapy. Only studies reporting patients’ survival as an outcome were included. Study results including other tumor types rather than EAC were included only when they allowed for a EAC patients subgroup analysis. Studies reporting combined results of EAC and GEJ adenocarcinomas were included as they have a similar treatment strategy. Case reports, opinion articles, non-human research articles, letters, abstracts, reviews, unpublished studies between 2015 and 2020, and studies in languages other than English or Portuguese were excluded.
Data extraction and quality assessment
Once chosen the studies to be included, relevant data were extracted from each article by two independent reviewers using previously defined criteria about study design, participants’ characteristics, interventions’ characteristics and outcome measures. Data not reported in the study were indicated as “NR” (not reported). In cases of more than one effect’s estimate presented, the most adjusted one was considered.
Concerning bias risk, a quality score was assigned to each included study by two reviewers using The Newcastle-Ottawa Quality Assessment Scale for Cohort Studies (19), as described in other studies (20,21). It consists of eight questions, distributed through three categories (selection, comparability and outcome), with a possible maximum score of nine points. Higher scores indicate higher methodological quality. We considered scores of 0-3, 4-6 and 7-9 to represent low, medium and high-quality studies, respectively. Disagreements of ratings were discussed, and final scores were established by consensus. Scale items and total score for each study can be found in supplementary table 2.
Supplementary Table 2 - Newcastle-Ottawa Quality Assessment Scale for Cohort Studies

Study endpoints and data analysis
The main outcome of interest was the therapeutic value of lymphadenectomy extension based on OS. Data were summarized using hazard ratio (HR) with 95% confidence intervals (95% CIs) and a random-effects meta-analysis was performed using Review Manager software (RevMan version 5.4, The Cochrane Collaboration, 2020). HR and its CI estimative were extracted directly from the study or calculated using Kaplan-Meier curves data whenever possible (22,23). There was some variation in the thresholds of lymphadenectomy extension among studies. When several cutoffs were available, we considered the most adjusted value, and when no lymph nodes cutoff numbers were defined, we considered the median number of nodes resected.
Studies’ heterogeneity was statistically assessed using Cochran’s Q test with significance set at p<0.10 (24), and Higgins I-squared statistic to evaluate the variation degree not accountable by chance. I2 values of 25%, 50% and 75% correspond to low, moderate and high heterogeneity, respectively (24, 25). Adenocarcinoma location and the use of either categorical or continuous variables were further explored using subgroup analysis as they were expected to be potential causes for inter-study heterogeneity. A funnel plot analysis was performed to account for publication bias. Statistical significance level was set at p <0.05.
RESULTS
Selection of studies and study characteristics
Study inclusion process flow-chart is shown in fig. 1. The systematic electronic search in the literature identified 655 articles. Six additional articles were identified through reference searching. Duplicates elimination resulted in 513 articles, of which 27 were retrieved to full-text screening. Five retrospective cohort studies were eligible for review and included in the qualitative analysis (16,17,26,27,28). One article was not included in the meta-analysis as it has insufficient data for determining an estimate of HR (28). A total of 10385 patients were included. Included studies characteristics are described in table 1 and table 2. Included studies were published between 2017 and 2020, with sample sizes ranging from 215 to 3953 patients. One study was single-center and four were multicenter studies. Median number of resected lymph nodes was reported in four studies, ranging from 14 to 33 nodes. Threshold variations defining low and high volume LNY groups are summarized in table 2. The quality score was 7 in three studies and 8 in two, pointing to the high quality of these studies.
Figure 1 - Flow-chart of literature search of eligible studies
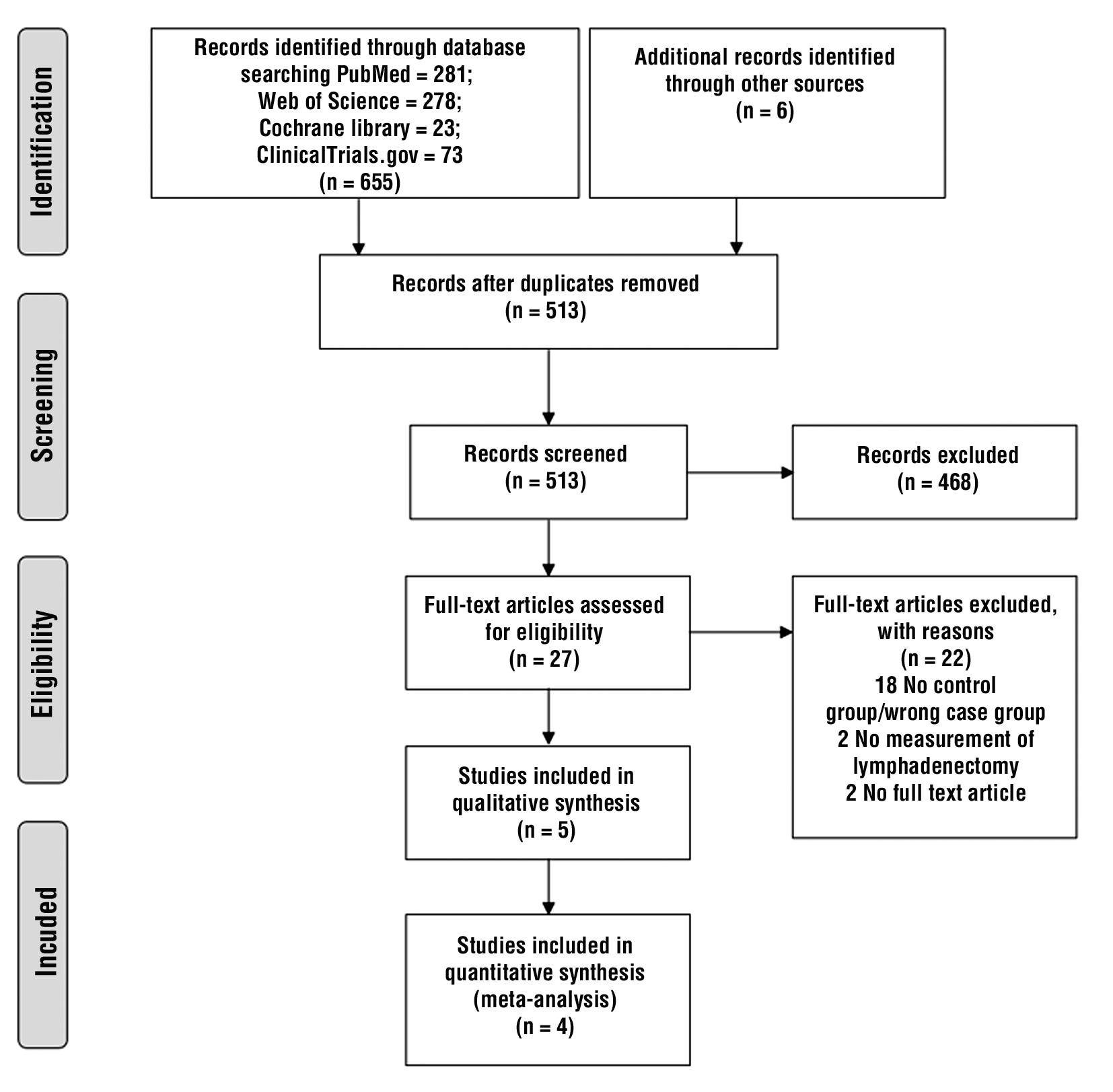
Table 1 - Baseline characteristics of Included Studies

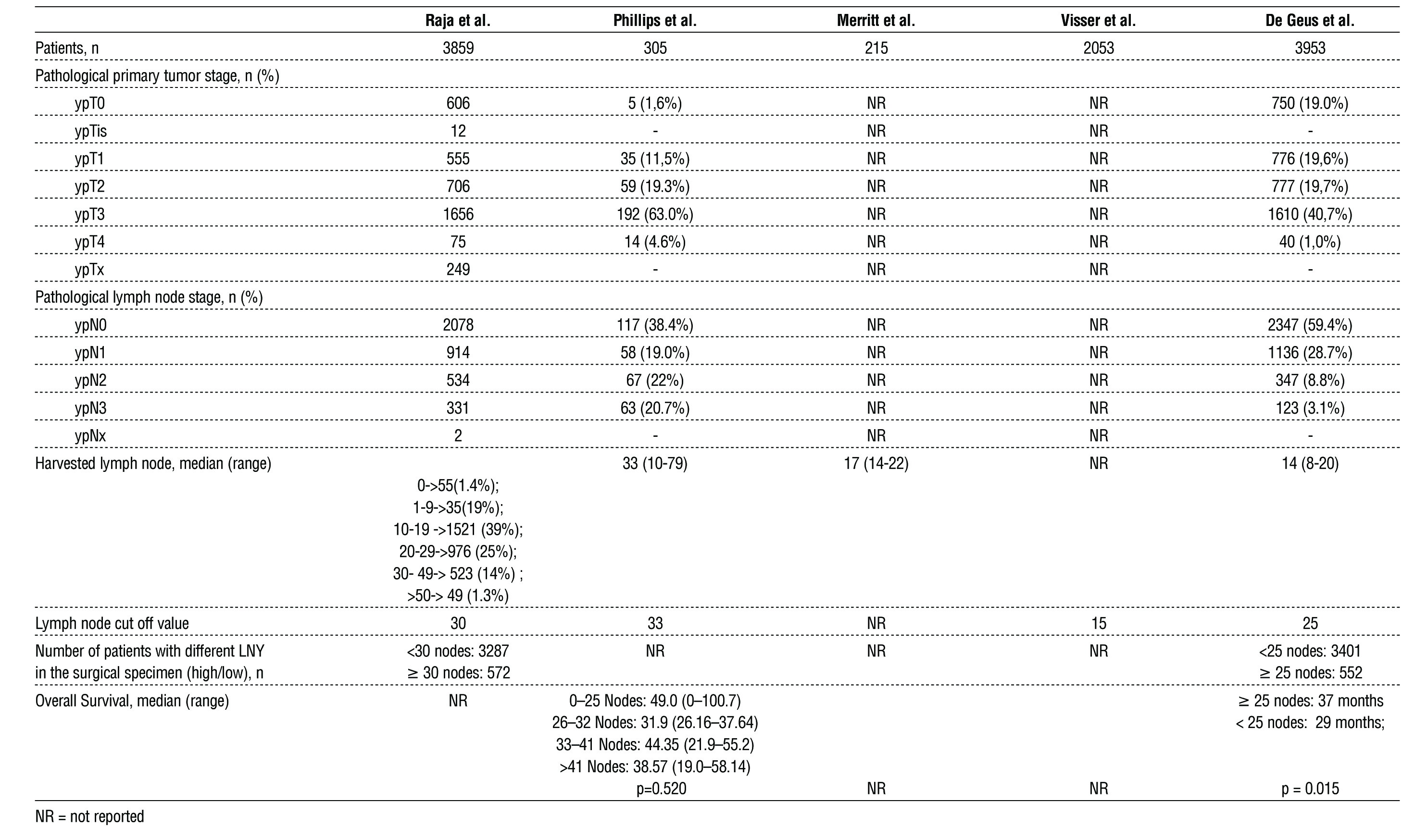
Table 2 - Tumor and Lymph node harvest characteristics of Included Studies
Prognostic impact of lymphadenectomy extension: qualitative analysis
As one study was not included in the meta-analysis we synthetized data in a descriptive way (28).
Patients’ median age ranged from 61 to 64 years-old and most were male gender. All five articles reported cases of EAC and three also included GEJ adenocarcinomas (16, 27, 28). There were some differences in the neoadjuvant therapy regimens among studies (three chemoradiation, one chemotherapy and another one chemotherapy, radiotherapy or both) Follow-up period ranged from 34 to 54.7 months but was not stated in two studies (28, 26). Four studies carried out univariate and multivariate analysis, providing or allowing estimation of HR (16,17,26,27) (table 1).
Regarding tumor and lymph node sresected, three studies provided pathological staging (16,26,28), as described in Table 2. Three also reported a median number of lymph nodes resected, ranging from 14 to 33 (16, 26, 27), and one stratified patients through the number of nodes resected (28) (table 2).
All five articles included analyze the association between lymphadenectomy extension and OS in patients diagnosed with EAC treated with neoadjuvant therapy followed by esophagectomy. Three reported that extended lymphadenectomy improved OS, after controlling for confounders and regardless of the cutoff values defined for the number of lymph node resected (26, 17, 28). The other two studies could not find any significant differences in OS among groups (16, 27).
One study, Raja et al., found this relation to be parabolic (28). More extensive lymph node resections were associated with longer OS, only up to a certain point, after which OS progressively declines. They also concluded that the extension of lymphadenectomy needed to achieve better OS was higher in patients with positive lymph nodes (for ypN0 cancers an additional survival benefit was estimated for up to 25 lymph nodes resected and in ypN+ tumors up to 30 lymph nodes have to be resected to achieve this benefit). Visser et al., found that patients with negative lymph nodes benefit have greater benefit from higher lymphadenectomy yield (cN0 HR 0.70, 95% CI 0.58–0.85 vs cN+ HR 0.80, 95% CI 0.70–0.9) (17).
All studies reported that extended lymphadenectomy improves OS, regardless the cutoff values defined for number of lymph nodes resected, though only three show statistically significant results.
Prognostic impact of lymphadenectomy extension: quantitative analysis
Four studies (6526 patients) were included in the quantitative analysis comparing OS from high and low lymphadenectomy extension (16,17,26,27). Only two reported statistically significant differences between groups with different number of resected lymph nodes, with a better OS in the group with higher lymphadenectomies performed. Among studies with no statistically significant results, one reported higher survival rates in cases of more extensive lymphadenectomy and the other showed lower survival in patients submitted to more extended lymphadenectomies. The pooled analysis showed (HR=0.88; 95% CI:0.74-1.04, p=0.13) thath a higher extension of lymphadenectomy is associated with better OS. A significant heterogeneity (I2 = 86%, p < 0.001) was to be noticed. The forest plot is shown in fig. 2.
Figure 2 - Forest plot of random effects meta-analysis for the effect of lymphadenectomy extension on OS in EAC patients. The test for heterogeneity is indicated with the I2 value

The subgroup analysis of the three studies with categorical analysis of lymphadenectomy extension revealed that a higher extension of resected lymph nodes was associated with better OS (HR=0.82; 95% CI: 0.69-0.98, p<0.05; I2 = 61%, p=0.08). The subgroup analysis stratified by EAC location revealed that a higher lymphadenectomy extension was associated with favorable survival outcome in studies that only included patients with EAC, (HR=0.77; 95% CI: 0.68-0.88, p<0.001) with low heterogeneity for results (I2 = 34%, p=0.22). The forest plots of subgroup analysis are presented in figs. 3, 4, respectively.
Figure 3 - Forest plot demonstrating improved OS with a high lymph node yield in studies with categorical analysis

Figure 4 - Forest plot demonstrating improved OS with a high lymph node yield in esophageal adenocarcinoma only populations

Publication bias
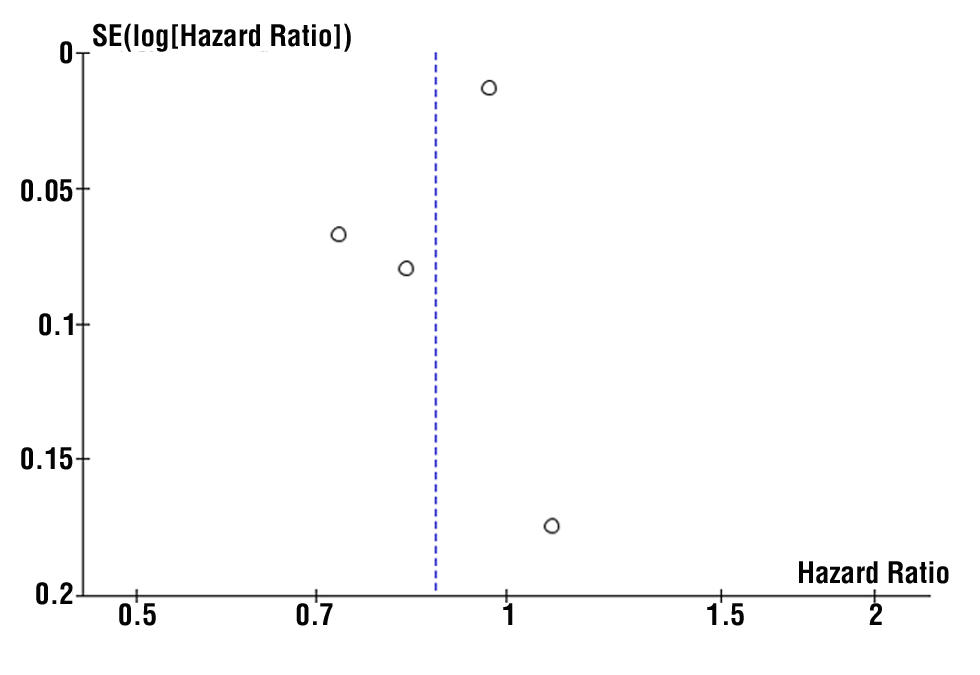
Funnel plot was made for visual screening of potential publication bias, particularly the association between results significance and opportunity of publication. As shown in fig. 5, despite the small number of studies, they were distributed evenly, suggesting no publication bias.
Figure 5 - Funnel plot to evaluate publication bias of included studies
DISCUSSION
For many years now, the extent of lymphadenectomy has been considered important to accurately ascertain pathological tumor staging, providing it a better prognostic value (17). However, the true value of resecting more lymph nodes in terms of treatment and survival is unclear and still under debate. With increasing indications for neoadjuvant therapy in EAC, this issue has become more relevant, as some can expect it to reduce the extent of lymphadenectomy needed. In 2018, Visser et al. published a systematic review and meta-analysis on the prognostic value of LNY on OS in EC patients. Their analysis concluded that a more radical lymphadenectomy was associated with significantly improved OS. Only seven studies had patients receiving neoadjuvant therapy and the effect of lymphadectomy on OS was smaller in this subset of patients (HR = 0·82; 95% CI = 0·73–0·92; p < 0·01) (29). More recently, Chen et al. published a systematic review and meta-analysis on LNY affecting OS in EC patients submitted to both neoadjuvant therapy and esophagectomy (30). Their results demonstrate that an increased LNY was associated with improved OS (HR = 0·87; 95% CI: 0·79–0·95, p < 0·001). However, there was a significant heterogeneity in their meta-analysis (I2 = 90·1%, p < 0·001), and none of their subgroup analysis could reduce it (30). Even though both reviews evaluated the extent of LNY IN OS of EC patients submitted to esophagectomy, and one of them in patients also receiving neoadjuvant therapy, both failed to account for the biopathological differences among different types of EC. Due to an unfavorable biology, EAC is less likely to respond to neoadjuvant chemoradiation therapy, leading to an increase need to further extend the LNY during resection (17). As per our knowledge, this is the only systematic review with meta-analysis that fully addresses this situation, intending to provide more detailed information on how to manage this specific subset of patients, offering them the best available treatment options.
Our results have not found a statistically significant difference in OS based on the lymphadenectomy extension. However, when analyzing the subset of studies with categorical analysis for this outcome, an increased number of lymph nodes resected had a clear benefit in OS (n=3, HR=0.82, p<0.05; I2 = 61%, p=0.08), suggesting that differences in study methodology (i.e., group analysis for specific outcomes), had impact in OS pooled analysis.
Moreover, a more extended lymphadenectomy was associated with better OS in EAC patients without considering the GEJ adenocarcinomas (n=2, HR=0.77, p<0.001; I2 = 34%, p=0.22), showing that there might be a location-dependent difference influencing the overall analysis. Reasons for this remain to be cleared, but studies selection might play a role and further research is required.
Although heterogeneities were significantly reduced by subgroup analysis, they lead to a reduction in the number of studies included, limiting data reliability.
All five studies reported a similar conclusion, indicating that an extended lymphadenectomy during esophagectomy preceded by neoadjuvant treatment was associated with better OS. However, in one study this improvement in OS was only seen up to a certain extent, after which OS gradually declined (28). Contradicting Soloman et al., studies included in this review showed that a more extended lymphadenectomy had a positive impact on survival for both positive and negative lymph nodes EAC (31).
Altogether, our results suggest that an extended lymphadenectomy not only has prognostic value but also therapeutic implications in EAC patients treated with neoadjuvant chemoradiation followed by esophagectomy.
However, several limitations should be acknowledged in this study and must be taken into account regarding its results. First, several unmeasured prognostic factors may have influenced survival results presented (i.e., number of positive nodes resected). However, given the limited information available, meta-regression to correct for these factors was not possible. Second, lymph node thresholds used to define high and low LNY groups varied considerably among studies, posing a major limitation to our analysis. This heterogeneity depends on surgical approach as well as pathological nodal identification protocol (32). Subgroup analysis regarding surgical approach and neoadjuvant therapy was not possible as data were too scarce to stratify for different treatment regimens.
Moreover, the number of lymph nodes resected does not necessarily correlate with the extent of lymphadenectomy performed. Several factors may contribute to a higher or lower number of lymph nodes identified by the pathologist, such as neoadjuvant chemorradiation therapy and surgical skills. Other than the number per se, positive lymph nodes distribution in relation to the diaphragm plays a role in prognosis (33). Prospective studies analyzing these variables altogether are required to fully evaluate the OS impact of lympha-denectomy extension. Lastly, the number of eligible studies included in our meta-analysis is relatively small, and considerable heterogeneity was observed on the pooled forest plot.
CONCLUSION
In conclusion, increased lymphadenectomy extension during esophagectomy (preceded by neoadjuvant therapy) might be associated with improved OS. Despite advances in EAC treatment, extended lymphadenectomy should be the standard of care and the yield of lymph node resection should be taken into account as it is a prognostic factor for patients’ survival.
Compared to surgery alone, multimodal therapy is associated with higher rates of negative resection margins, lower recurrence rates, and improved survival.
Comparisons regarding EC treatment should consider oncological protocols as a whole while drawing conclusions in EAC patients’ cohorts.
More studies are required to assess the survival benefits of a higher LNY in EAC patients receiving
multimodal therapy. Pathological node identification protocols need to be taken into consideration in designing future cohorts.
Authors’ Contribution
All listed contributors designed the study and did the collection and assembly of data as well as data analysis and interpretation. All authors wrote the manuscript and did its final approval.
Conflicts of interest: None
Acknowledgments and Disclosures
The authors have no conflict of interest to declare. No financial support and technical or other assistance were received.
REFERENCES
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
2. Arnold M, Laversanne M, Brown LM, Devesa SS, Bray F. Predicting the future burden of esophageal cancer by histological subtype: international trends in incidence up to 2030. Am J Gastroenterol. 2017;112(8):1247-1255.
3. Mansour NM, Groth SS, Anandasabapathy S. Esophageal adeno-carcinoma: screening, surveillance, and management. Annu Rev Med. 2017;68:213-227.
4. Lerut T. Carcinoma of the esophagus and gastro-esophageal junction. Surgical treatment: evidence-based and problem-oriented. Munich: Zuckschwerdt: 2001.
5. Rice TW, Blackstone EH, Rusch VW. 7th edition of the AJCC Cancer Staging Manual: esophagus and esophagogastric junction. Ann Surg Oncol. 2010;17(7):1721-4.
6. Rice TW, Ishwaran H, Blackstone EH. Oesophageal cancer: location, location, location. Oxford University Press; 2015.
7. Howlader N NA, Krapcho M, Miller D, Bishop K, Altekruse SF, Kosary CL, et al. SEER Cancer Statistics Review. Bethesda, MD: National Cancer Institute 1975-2013.
8. Wu PC, Posner MC. The role of surgery in the management of oesophageal cancer. Lancet Oncol. 2003;4(8):481-8.
9. Sjoquist KM, Burmeister BH, Smithers BM, Zalcberg JR, Simes RJ, Barbour A, et al. Survival after neoadjuvant chemotherapy or chemo-radiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12(7):681-92.
10. Eng O, Nelson R, Konstantinidis I, Chao J, Erhunmwunsee L, Raz D, Kim J. Disparities in survival after multimodal therapy for esophageal adenocarcinoma. Dis Esophagus. 2018;31(9).
11. Hagens ERC, Kunzli HT, van Rijswijk AS, Meijer SL, Mijnals RCD, Weusten B, et al. Distribution of lymph node metastases in esophageal adenocarcinoma after neoadjuvant chemoradiation
therapy: a prospective study. Surg Endosc. 2020;34(10):4347-4357.
12. Prenzel KL, Bollschweiler E, Schröder W, Mönig SP, Drebber U, Vallboehmer D, et al. Prognostic relevance of skip metastases in esophageal cancer. Ann Thorac Surg. 2010;90(5):1662-7.
13. Hagen JA, DeMeester SR, Peters JH, Chandrasoma P, DeMeester TR. Curative resection for esophageal adenocarcinoma: analysis of 100 en bloc esophagectomies. Ann Surg. 2001;234(4):520-30; discussion 530-1.
14. Swanson SJ, Batirel HF, Bueno R, Jaklitsch MT, Lukanich JM, Allred E, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophago-gastrostomy for esophageal carcinoma. Ann Thorac Surg. 2001; 72(6):1918-24; discussion 1924-5.
15. Samson P, Puri V, Broderick S, Patterson GA, Meyers B, Crabtree T. Extent of Lymphadenectomy Is Associated With Improved Overall Survival After Esophagectomy With or Without Induction Therapy. Ann Thorac Surg. 2017;103(2):406-415.
16. Phillips AW, Lagarde SM, Navidi M, Disep B, Griffin SM. Impact of extent of lymphadenectomy on survival, post neoadjuvant chemo-therapy and Transthoracic Esophagectomy. Ann Surg. 2017;265(4): 750-756.
17. Visser E, van Rossum PSN, Ruurda JP, van Hillegersberg R. Impact of lymph node yield on overall survival in patients treated with neoadjuvant chemoradiotherapy followed by esophagectomy for cancer a population-based cohort study in the Netherlands. Ann Surg. 2017;266(5):863-869.
18. Page MJ, Moher D, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021; 372:n160.
19. Wells GA, Shea B, O’Connell Da, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Oxford; 2000.
20. Griffiths RI, Keating NL, Bankhead CR. Quality of diabetes care in cancer: a systematic review. Int J Qual Health Care. 2019;31(2):75-88.
21. Yeh T-L, Lei W-T, Liu S-J, Chien K-L. A modest protective association between pet ownership and cardiovascular diseases: A systematic review and meta-analysis. PLoS One. 2019;14(5): e0216231.
22. Simon R. Confidence intervals for reporting results of clinical trials. Ann Intern Med. 1986;105(3):429-35.
23. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8(1):1-16.
24. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
25. West SL, Gartlehner G, Mansfield AJ, Poole C, Tant E, Lenfestey N, et al. Comparative effectiveness review methods: clinical heterogeneity. 2010.
26. de Geus SWL, Hirji S, Hachey KJ, Sachs TE, Suzuki K, Ng SC, et al. Lymphadenectomy and Survival After Neoadjuvant Chemoradiation for Esophageal Adenocarcinoma: Is More Better? J Gastrointest Surg. 2020;24(11):2447-2455.
27. Merritt RE, Abdel-Rasoul M, Souza DMD, Kneuertz PJ. Nomograms for predicting overall and recurrence-free survival after multimodal therapy for esophageal adenocarcinoma. J Surg Oncol. 2021; 123(4):881-890. Epub 2020 Dec 17.
28. Raja S, Rice T, Murthy S, Ahmad U, Semple M, Blackstone E, et al. Value of lymphadenectomy in patients receiving neoadjuvant therapy for esophageal adenocarcinoma. Ann Surg. 2021;274(4): e320-e327.
29. Visser E, Markar SR, Ruurda JP, Hanna GB, van Hillegersberg R. Prognostic value of lymph node yield on overall survival in esophageal cancer patients a systematic review and meta-analysis. Ann Surg. 2019;269(2):261-268.
30. Chen D, Mao Y, Xue Y, Sang Y, Liu D, Chen Y. Does the lymph node yield affect survival in patients with esophageal cancer receiving neoadjuvant therapy plus esophagectomy? A systematic review and updated meta-analysis. EClinicalMedicine. 2020;25:100431.
31. Solomon N, Zhuge Y, Cheung M, Franceschi D, Koniaris LG. The roles of neoadjuvant radiotherapy and lymphadenectomy in the treatment of esophageal adenocarcinoma. Ann Surg Oncol. 2010; 17(3):791-803. Epub 2009 Dec 2.
32. Talsma AK, Shapiro J, Looman CW, van Hagen P, Steyerberg EW, van der Gaast A, et al. Lymph node retrieval during esophagectomy with and without neoadjuvant chemoradiotherapy: prognostic and therapeutic impact on survival. Ann Surg. 2014;260(5):786-92;
discussion 792-3.
33. Talsma AK, Ong C-AJ, Liu X, van Hagen P, Van Lanschot JJ, Tilanus HW, et al. Location of lymph node involvement in patients with esophageal adenocarcinoma predicts survival. World J Surg. 2014; 38(1):106-13.
Full Text Sources:
Abstract:
Views: 3725

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.