Surgery, Gastroenterology and Oncology

|
|
Purpose: This study aims to investigate the role of mammographic microcalcification as an indicator for the occurrence of bone metastasis and to identify associated influencing factors.
Patients and Methods: A case-control study was conducted using data from breast cancer patients who sought treatment at the Dr. Cipto Mangunkusumo National Central General Hospital between June 2019 and June 2021. The case group included breast cancer patients with bone metastasis. On the other hand, the control group consisted of individuals who did not have bone metastasis determined by x-ray, Computed Tomography (CT) scan, and bone scan. Mammography was used to show the presence of microcalcification. Following that, univariate and bivariate analyses were carried out.
Results: Eighty-one patients were enrolled in this study. The cohort predominantly comprised individuals over 50 years of age (56.8%), with a body mass index (BMI) below 30 (86.4%), who were premenopausal (76.5%), and presented with advanced disease stages (71.6%). Most patients had Non-Special Type (NST) histopathology criteria (70.4%) and luminal B subtype of breast cancer (58%). Among all study subjects, 25 patients had bone metastasis. There was a significant association between the advanced stage and microcalcification (OR 3.740; 95%CI 1.288-10.860; p 0.024). The advanced stage (OR 6.900; 95% CI 1.475-32.278; p 0.014) and microcalcification (OR 3.284; 95% CI 1.212-8.899; p 0.032) were also significantly associated with bone metastasis.
Conclusion: The presence of microcalcification is associated with bone metastasis occurrence. Also, the advanced stage is associated with microcalcification and bone metastasis.
Introduction
In the world, breast cancer is the most frequent cancer diagnosis and the fifth leading cause of cancer death. According to GLOBOCAN 2020, the incidence of breast cancer accounts for 11.7% of all cancers in women and men (1). Epidemiological study by Hospital-Based Cancer Registry Data 2008-2012 in Indonesia shows that most breast cancer patients present with stage IIIB or IV (2,3). Breast cancer not detected early will develop into an advanced stage, leading to metastasis to other essential body organs, especially the bones (70%) (4). This delay in detection will increase morbidity in the form of permanent bone damage, pain, and paralysis due to pathological fractures or spinal nerve compression (4,5).
The mechanism of bone metastasis in breast cancer is a complex process. There is a role for several genes and biomarkers that have been studied to predict the incidence of bone metastasis in breast cancer. The ESR1, GATA3, and MLPH genes can be used as predictors (6). Receptor Activator of Nuclear Factor K? (RANK) and Type 4 CXC Chemokine Receptor (CXCR4) are significantly related to bone metastasis (7). Other than that, the biomarker DKK-1 is a potential predictor of bone metastasis (8). Other potential biomarkers crucial for predicting metastasis to the bone include Receptor Activator of Nuclear Factor K?-Ligand (RANKL), Breast Osteoblast-Like Cells (BOLCs), and Connective Tissue Growth Factor (CTGF). Additionally, bone biomarkers such as Bone Morphogenetic Proteins (BMP)-2, Pentraxin-3 (PTX3), and Small Integrin-Binding Ligand N-linked Glycoproteins (SIBLINGs) play a regulatory role in this process (9,10). SIBLINGs consisting of Osteopontin (OPN), Bone Sialoprotein (BSP), Dentin Matrix Protein-1 (DMP1), and Dentin Sialophosphoprotein (DSPP) have an indispensable role in the process of bone metastasis. SIBLINGs are expressed by bone and teeth and play a role in regulating hydroxyapatite (HA) crystal formation, an ectopic dystrophic premalignant calcification that arises outside the skeletal system in the form of microcalcification (11,12). Microcalcification is found in tumor areas with the highest immunoreactivity against bone matrix protein, indicating that OPN expression may play an essential role in facilitating the spread of tumor cells to the bone microenvironment (13). There is a significant association between microcalcification with 63.3% incidence of bone metastasis in breast cancer patients within five years.14 There is also an association between the formation of microcalcification in the breast and the formation of bone metastasis (15). The formation of microcalcification by breast cancer cells is similar to the mineralization process in bone.16 Other findings show there is a microcalcification in 79% of invasive breast cancer and 94% of Ductal Carcinoma In Situ (17).
Nowadays, various types of biomarkers and gene examinations are available to detect the early presence of metastasis. However, they are challenging in various healthcare centers, especially remote hospitals. Not only are these services costly, but they are not accessible in most hospitals. Presently, bone metastasis is detected through radiological examination in the form of bone scan, Computed Tomography (CT) Scan, Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET) Scan, and others (18). Current mammography examination is already widely available in type B hospitals in Indonesia and has been widely used to detect early breast cancer (19-21). Based on previously mentioned literature which states that there might be a relationship between microcalcification on mammography and the incidence of bone metastasis, authors intend to examine the presence of microcalcification in mammography of breast cancer patients as a parameter of the bone metastasis occurrence and the factors influencing it.
Methods
This case-control study recruited subjects from the oncology outpatient clinic at Dr. Cipto Mangunkusumo National Central General Hospital from September to November 2021, using secondary data from the medical records. All subjects were patients diagnosed clinically with breast cancer. The inclusion criteria were as follows: (1) breast cancer patients seeking treatment at surgical oncology outpatient clinic who have undergone histopathology biopsy and immunohistochemistry examinations; (2) breast cancer patients who have undergone mammography examination; and (3) breast cancer patients who have undergone bone scan or other additional examination to confirm whether they have bone metastasis or not. The exclusion criteria were incomplete medical records. Data were collected regarding age, body mass index (BMI), cancer stage, cancer histopathology type, immunohistochemistry examination, mammography examination, and imaging examination. The data were analyzed using SPSS 20.0 and presented in the results. Univariate analysis was used to depict the characteristics of the patients. Bivariate analysis was used to show the association between clinicopathological characteristics (age, BMI, menopausal state, cancer stage, immuno-histo-chemistry type, and histology invasion) and micro-calcification found on mammography examination and metastasis. The association between variables was significant if the p-value was < 0.05.
Results
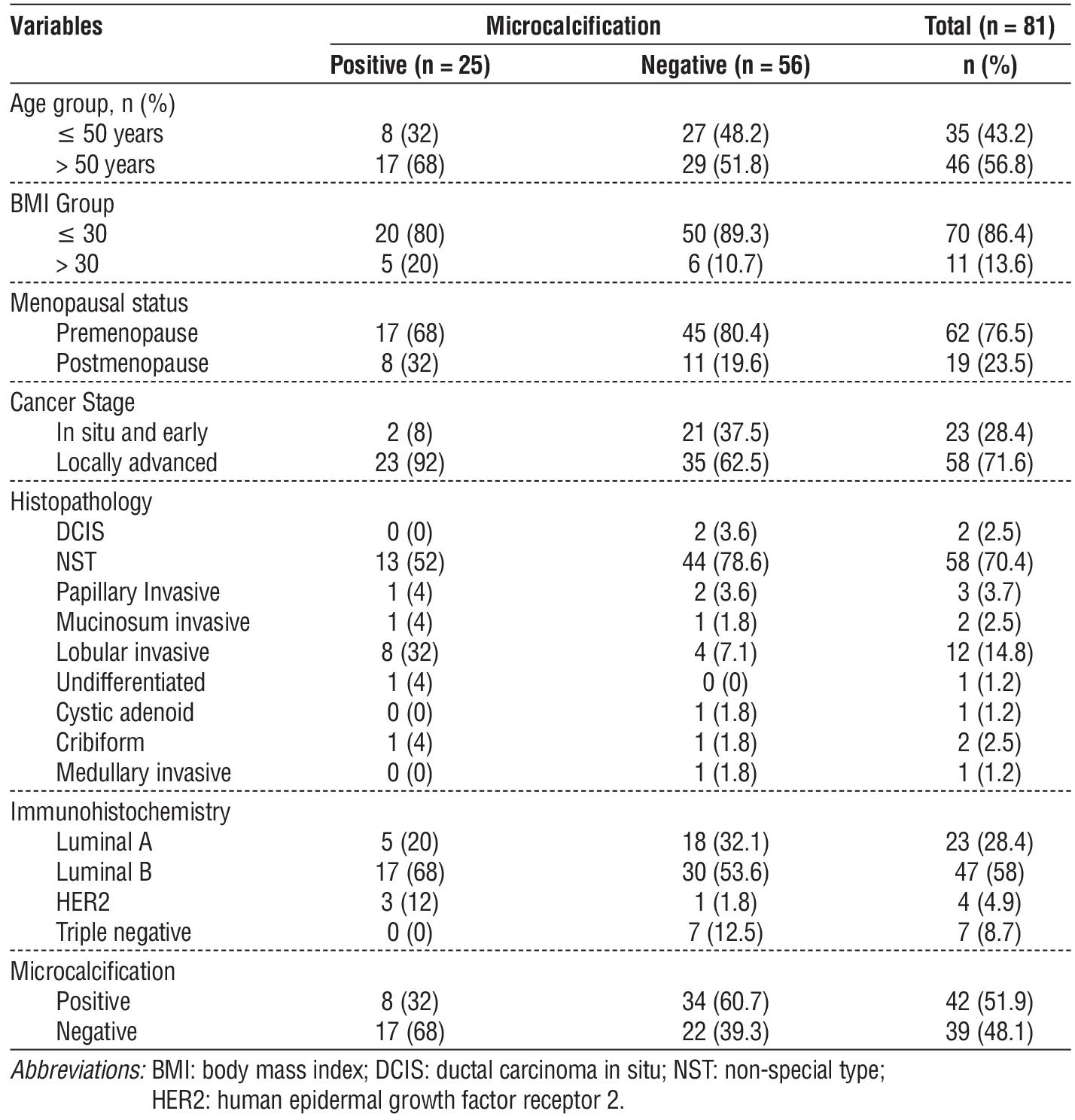
Eighty-one patients were included in the study. Most patients were over 50 years old, had BMI lower than or equal to 30, and were premenopausal. Most of the patients had an advanced stage (71.6%) with the histopathological type of Non-special Type (NST) (70.4%) and immunohistochemistry subtype of luminal B (58%). Thirty-nine patients out of 81 showed microcalcification in the mammography examination, and 25 patients out of 81 had metastatic disease at the time of data collection. Bone metastasis was mainly found in patients with age over 50, low or normal BMI, premenopause state, and locally advanced stage. Eight patients with microcalcification were found to have metastatic disease, as shown in table 1.
Table 1 - Clinicopathological characteristics of patients
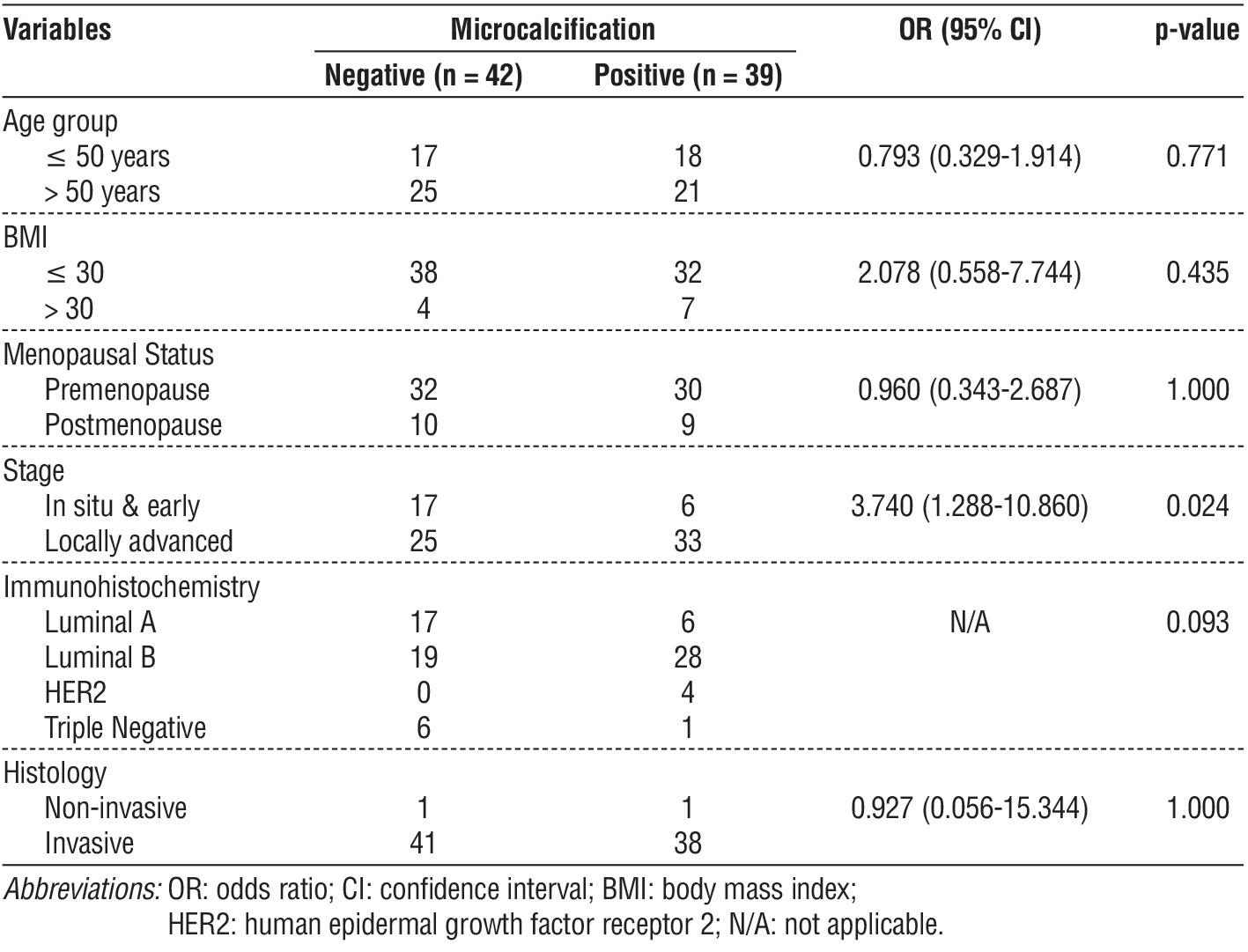
Among the clinicopathological characteristics in table 2, the cancer stage was the only one with a significant association with microcalcification. Patients with locally advanced cancer further correlated significantly with microcalcification in which locally advanced patients had a 3.74 times chance of having microcalcification on mammography examination compared to those with early stage and in situ cancer (p=0.024, OR 95% CI 1.29 – 10.86).
Table 2 - The association between clinicopathological characteristics and the presence of microcalcification
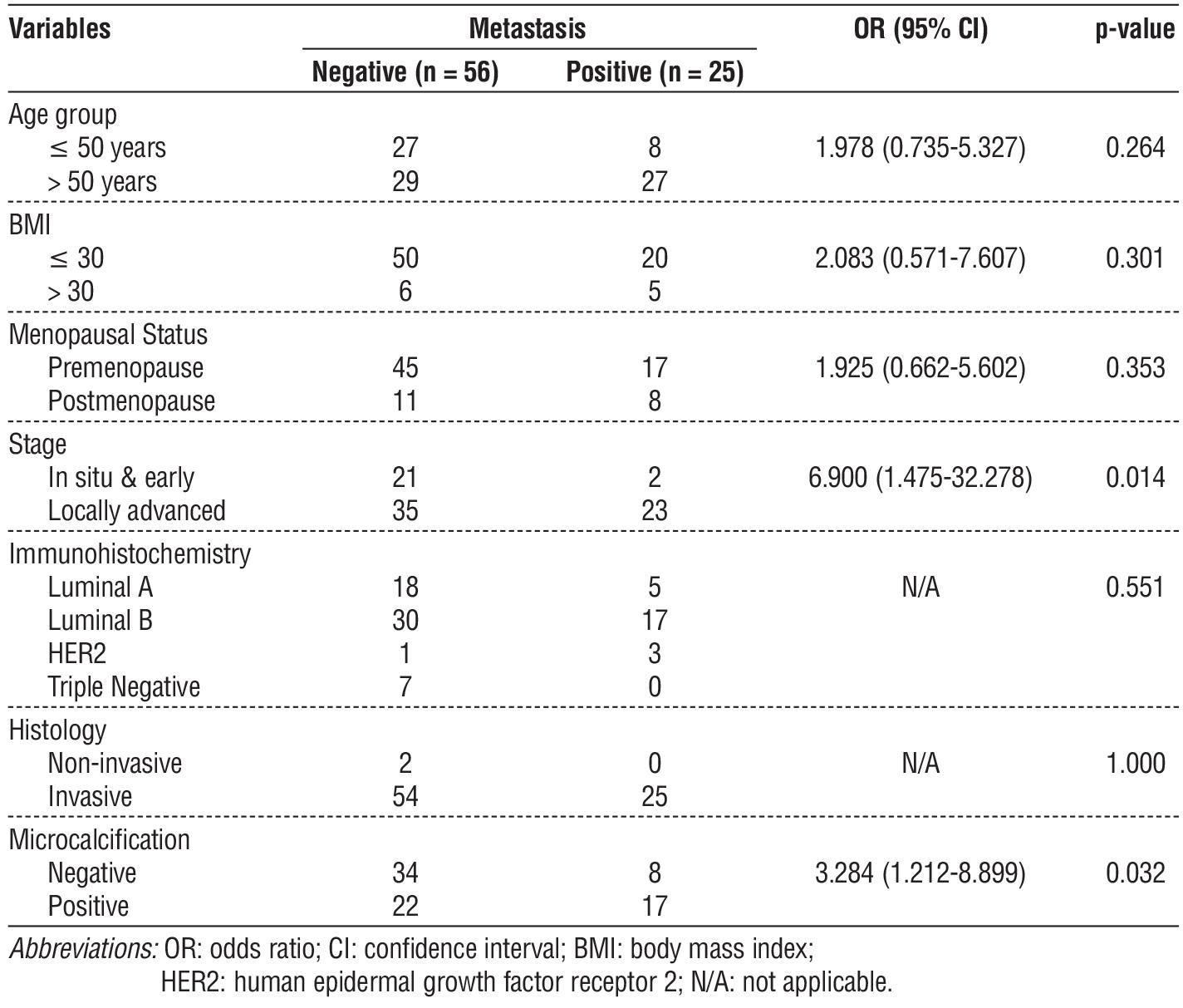
The association between clinicopathological characteristics, microcalcification, and metastasis is shown in table 3. The results showed that breast cancer stage and microcalcification were significantly associated with metastasis, with a p-value of 0.014 and 0.032, respectively.
Table 3 - The association between clinicopathological characteristics and metastasis
Discussion
The results show that age, BMI, menopausal status, immunohistochemistry type, and histology type do not have a significant association with microcalcification. A study about the relationship between microcalcification and breast cancer patients’ clinicopathological characteristics supported the result of no significant association between age and microcalcification (p = 0.097) (22). In contrast, another study showed that age is significantly associated with microcalcification (p=0.004). There was a theory regarding the physiological association of age and microcalcification associated with menopause and aging processes. Many cases of microcalcification post-lactation were reported in several works of literature. The combination of apoptosis and secretion stasis that cause the breast glands to regress and become atrophy could result in an appearance of microcalcification (23). Those processes could change the nature of breast cells to increase proliferation activities, followed by enhanced differentiation and migration abilities into mesenchyme phenotype as the beginning of a malignant transformation (24). A prior study found that individuals with dense breast tissue had a considerably higher rate of underlying proliferative histology with calcifications than those with non-calcified lesions. This research implied that dense breasts may raise the risk of benign microcalcifications and that young women with dense breasts may have more of them (25). Hence, the relationship between age and Microcalcification still needs to be explored in a multicenter study involving more study samples.
This study shows that BMI is not associated with microcalcification formation. Another study that evaluated the association between BMI and microcalcification on mammography supports this study’s result (26). Many studies found an association between mammography density and microcalcification. The precise biological mechanisms underlying this association remain largely unclear. However, it is hypothesized that alterations such as an increase in proteoglycan matrix and collagen genesis within the extracellular matrix may be a contributing mechanism. These changes, by promoting more prevalent epithelial components and heightened matrix rigidity, are thought to induce Epithelial-Mesenchymal Transition (EMT), leading epithelial cells to acquire invasive mesenchymal characteristics that contribute to malignant microcalcification formation (27).
Another similar result to our study showed that menopausal status did not significantly associate with microcalcification (p=0.283) (22). Conversely, a Canadian study revealed a significant association between postmenopausal status and the incidence of micro-calcification (28). Postmenopausal condition causes increased breast gland involution, increasing breast density. This increasing density will induce the EMT process, implicating the risk of forming a mesenchymal phenotype as the first step of malignancy (27).
Statistically, the cancer stage has a significant association with microcalcification (p=0.024; OR = 3.740), which means that advanced disease has a 3.74 times probability of microcalcification occurrence compared to early and in situ diseases. This finding is supported by another study that showed size and cancer stage were factors determining the occurrence of microcalcification (p=0.041) (22). Advancement of the disease implicates increasing cancer stage, causing increased tissue density that induces involution process, microcalcification formation, and tumori-genesis (28).
Invasive histology type does not have a significant association with microcalcification in this study, supported by another study that showed no significant differences between non-invasive cancer and invasive carcinoma with microcalcification (p=0.231) (22). This finding is different from the theory that states there is a strong correlation between the presence of micro-calcification and the invasive nature of the tumor, along with increased calcium deposits and cell proliferation in breast tissue which surely increase microcalcification formation (28).
Immunohistochemistry subtypes that differentiate breast cancer according to the hormonal receptors do not significantly associate with microcalcification. A study about microcalcification in China supports this result (22). On the contrary, another study in Greece showed a significant correlation between positive estrogen and progesterone receptor with microcalcification (29).
Most of the research subjects are above 50 years old, and most patients with bone metastasis are also over 50. These results are supported by a study that evaluated breast cancer risk factors for distant post-operative metastasis. The supporting study also indicated that older age increases breast cancer risk (30). Another research on the relationship between age at diagnosis of breast cancer and the incidence of distant metastasis also reported that most breast cancer patients are over 50 years of age (71.7%) and have bone metastasis (63.8%) (31). There are different results from several studies of the effect of age on the risk of development of bone metastasis in breast cancer. Multicenter research in Germany found that over 65 years old, the risk of bone metastasis was 1.5 times higher than that of younger patients (32).
While many other studies showed that age did not significantly impact the risk of bone metastasis (33). A study by Pulido et al indicated age to be protective for bone metastases, whereas age under 40 tends to increase the risk of bone metastases twice as much as the older age (4). One of the causes of such differences in age groups obtained in this study could be the small number of samples.
Metastasis cases are more common in patients with lower or normal BMI than in higher ones. This result is similar to another study that found the most distant metastasis cases in the lower BMI group (90.6%) (30). The mechanism of BMI's role in bone metastasis is still in debate. BMI negatively affects the prognosis of breast cancer patients with bone metastasis. Patients with high levels of obesity have low overall survival and high recurrence. The underlying mechanism seems to be related to increased estradiol levels derived from the aromatization of androgens in high adipose tissue in postmenopausal women. This mechanism causes higher use of chemotherapy therapeutic doses and other harmful effects of obesity which further worsens patient performance and failure in therapy, thereby increasing tumor proliferation and causing metastasis to continue, including to the bone (4).
Breast cancer patients are more prevalent in the premenopausal group (76.5%) than the postmenopausal group (23.5%). The cases with bone metastasis also show similar results, with 68% of the patients in the premenopausal state. A study evaluated the risk factors of bone metastasis in breast cancer patients and had a similar result, in which 76% of the patients were in the premenopausal state (4). Another study showed that breast cancer was mostly found in the premenopause group (63.9%) (5). This phenomenon can be explained as breast cancer tends to arise at productive age because of the hormonal role in the development of the disease that causes an increased risk from 30 to 50% (4). Estrogen is an essential regulator of bone remodeling and contributes to a suitable environment for bone metastasis. A British study on 367 patients showed that bone-only metastasis was likely found in the older postmenopausal group (34).
Plenty of bone metastasis belongs to the locally advanced group. This finding is in line with another study that showed a higher incidence of bone metastasis in the locally advanced group (72.8%) (30). These findings support the theory that clinico-pathological factors such as cancer stage and lymph node involvement influence the occurrence of distant metastasis. Advanced cancer stage increases metastasis risk, in which chest wall and skin infiltration in locally advanced diseases strongly predict distant metastasis (30).
Most patients have the NST histology examination (70.4%). A similar finding was found, in which 69% of patients have NST breast cancer (3). Another study found that in breast cancer patients with bone metastasis, the majority of histologic type was also NST (80.7%) (5). A study that evaluated factors related to bone metastasis found that NST breast cancer significantly correlated with bone metastasis (p=0.011) (6). This is also supported by a study that stated NST was the most prevalent histologic type in breast cancer patients with bone metastasis (75.5%) (31). Several histopathology types of invasive breast cancer, namely ductal, lobular, medullar, tubular, and mucinous, have distinct characteristics influencing bone metastasis. Several studies showed that the invasive lobular type has more predictive value than the other types. There were debates among studies about whether tumor types influence the development of bone metastasis. Many researchers find no evidence that patients with lobular carcinoma are more likely to develop bone metastasis than those with ductal carcinoma and vice versa. Several other authors stated that lobular carcinoma tends to metastasize to bone (4).
The distribution of immunohistochemistry in this study is as follows: luminal B is 58%, luminal A is 28.4%, the triple negative is 8.7%, and HER2 is 4.9%. In the metastasis group, 68% are categorized as luminal B, 20% as luminal A type, and 12% as HER2 type. Different findings are found in a study that states the most prevalent type is luminal A (3). Strong association between hormonal receptors and bone metastasis has been studied extensively for the last two decades. Several theories have been proposed to support the association. One of which is the role of hormones, such as estrogen, that influences the development of bone growth and bone micro-environment, and the role of several gene expression, namely estrogen receptor (ESR 1) and progesterone receptor (PGR) in breast cancer patients with bone metastasis (33). Differences in this study may be due to the number of samples collected as patients is not as much as in other studies.
Among the breast cancer patients in this study, 39 of them (48.1%) have microcalcification on mammography examination. In the group of patients that have bone metastasis, seventeen of them (68%) have microcalcification on mammography examination. This result is found to be different from a previous study in which only 25% of the patients have microcalcification (22).
The association between microcalcification and bone metastasis has OR value of 3.284 with a p-value of 0.032. Breast cancer patients who have microcalcification on mammography examination have a 3.284 increased risk of bone metastasis compared to others who do not have microcalcification on mammography. This finding supports a previous study that stated several proteins like OPN are responsible for forming osteoblast-like phenotype, which has a role in the development of microcalcification and bone metastasis formation (15). This study result is in accordance with a study that supports the phenomenon in which they found BMP and OPN in microcalcification (14). Biopsy in the breast indicates both proteins' role in microcalcification formation and supports a study that showed the role of OPN in the development of bone metastasis (4). Similar results are also found in a study that showed BMP-2 as a protein that has a role in microcalcification formation, which tends to develop bone metastasis (22). A case report found the presence of microcalcification in 63.2% of bone metastasis patients and stated that the presence of microcalcification could be thought of as a poor prognosis to predict the occurrence of bone metastasis (14).
Limitation
Some of the data are incomplete as some patients have been diagnosed in other institutions and came to our institution only for bone metastasis treatment. Thus, we did not have full access to the other investigations carried out in the previous institutions. This study also did not assess the period between the presence of microcalcification found on mammography examination with the occurrence of bone metastasis, so that it can bias the significance of the research results. Another limitation of this study is that case-control studies do not have temporality between exposures and effects on study subjects.
Conclusion
There is a statistically significant association between the presence of microcalcification on mammography and the occurrence of bone metastasis in breast cancer patients. Furthermore, cancer stage is also significantly associated with microcalcification.
Acknowledgements
The authors would like to thank Shabrina Adzania, MD, and Lie Rebecca Yen Hwei, MD, for assisting the publication of this study.
Conflicts of Interest
The author reports no conflicts of interest in this work.
Ethics Approval and Consent to Participate
This study received ethical approval from The Health Research Ethics Committee – Faculty of Medicine Universitas Indonesia and Dr. Cipto Mangunkusumo Hospital (HREC-FMUI/CMH) with reference number KET/820/UN2.F1/ETIK/PPM.00.02/ 2021. Informed consent from the study participants was obtained to be involved in this study.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
2. Gondhowiardjo S, Christina N, Ganapati NP, Hawariy S, Radityamurti F, Jayalie V, et al. Five-year cancer epidemiology at the national referral hospital: hospital-based cancer registry data in Indonesia. JCO Glob Oncol. 2021;5(1):190-203.
3. Gondhowiardjo S, Soediro R, Jayalie VF, Djoerban Z, Siregar NC, Poetiray EDC. Multicenter Management of Breast Cancer in Indonesia: Ten Years of Experience. eJournal Kedokteran Indonesia. 2020;8:121–30.
4. Pulido C, Vendrell I, Ferreira AR, Casimiro S, Masinho A, Alho I, et al. Bone metastasis risk factors in breast cancer. Ecancermedicalscience. 2017;11:715.
5. Chen WZ, Shen JF, Zhou Y, Chen XY, Liu JM, Liu ZL. Clinical characteristics and risk factors for developing bone metastases in patients with breast cancer. Sci Rep. 2017;7(1):1-7.
6. Cosphiadi I, Atmakusumah TD, Siregar NC, Muthalib A, Harahap A, Mansyur M. Bone metastasis in advanced breast cancer: analysis of gene expression microarray. Clin Breast Cancer. 2018;18(5):e1117-e1122.
7. Yulian ED, Panigoro SS, Sudijono B, Gautama W, Rustamadji P, Dosan R. CXCR4 and RANK Combination as a Predictor of Breast Cancer Bone Metastasis in Indonesia. J Surg Surgical Res. 2021; 7(1):020-025.
8. Limba FWS, Yulian ED, Kartini D, Andinata B, Tjahjadi H, Vidiawati D. Dickkopf-1 Expression as a Predicting Factor for Bone Metastasis in Breast Cancer. UHOD-ULUSLAR HEMATOL. 2020;31(3):171-179.
9. Lamour V, Nokin MJ, Henry A, Castronovo V, Bellahcène A. Les protéines SIBLING - Outils moléculaires de la progression tumorale et de l’angiogenèse. Med Sci (Paris). 2013;29(11):1018-1025.
10. Zhao H, Chen Q, Alam A, Cui J, Suen K, Soo A, et al. The role of osteopontin in the progression of solid organ tumour. Cell Death Dis. 2018;9(3):1-15.
11. Scimeca M, Urbano N, Bonfiglio R, Schillaci O, Bonanno E. Breast osteoblast-like cells: A new biomarker for the management of breast cancer. Br J Cancer. 2018;119(9):1129-1132.
12. Scimeca M, Trivigno D, Bonfiglio R, Ciuffa S, Urbano N, Schillaci O, et al. Breast cancer metastasis to bone: From epithelial to mesenchymal transition to breast osteoblast-like cells. Semin Cancer Biol. 2021;72:155–164.
13. Bellahcène A, Castronovo V, Ogbureke KU, Fisher LW, Fedarko NS. Small integrin-binding ligand N-linked glycoproteins (SIBLINGs): multifunctional proteins in cancer. Nat Rev Cancer. 2008;8(3):212–226.
14. Bonfiglio R, Scimeca M, Toschi N, Pistolese C, Giannini E, Antonacci C, et al. Radiological, histological and chemical analysis of breast microcalcifications: diagnostic value and biological significance. J Mammary Gland Biol Neoplasia. 2018;23(1):89-99.
15. Rizwan A, Paidi SK, Zheng C, Cheng M, Barman I, Glunde K. Mapping the genetic basis of breast microcalcifications and their role in metastasis. Sci Rep. 2018;8(1):1-10.
16. Cox RF, Morgan MP. Microcalcifications in breast cancer: Lessons from physiological mineralization. Bone. 2013;53(2):437–450.
17. Tsai HT, Huang CS, Tu CC, Liu CY, Huang CJ, Ho YS, et al. Multi-gene signature of microcalcification and risk prediction among Taiwanese breast cancer. Sci Rep. 2020;10(1):1-10.
18. Rong Y, Ren H, Ding X. MRI and bone scintigraphy for breast cancer bone metastases: a meta-analysis. Open Med. 2019;14(1):317–323.
19. Cook GJR, Azad GK, Goh V. Imaging Bone Metastases in Breast Cancer: Staging and Response Assessment. J Nucl Med. 2016; 57(Suppl 1):27S-33S.
20. Pesapane F, Downey K, Rotili A, Cassano E, Koh DM. Imaging diagnosis of metastatic breast cancer. Insights into Imaging. 2020; 11(1):1-14.
21. Kementerian Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor 1014/MENKES/SK/IX/2008 tentang Standar Pelayanan Radiologi Diagnostik Di Sarana Pelayanan Kesehatan. 2008. (Unpublished)
22. Zhang L, Hao C, Wu Y, Zhu Y, Ren Y, Tong Z. Microcalcification and BMP-2 in breast cancer: correlation with clinicopathological features and outcomes. Onco Targets Ther. 2019;12:2023-2033.
23. Alsheh Ali M, Czene K, Hall P, Humphreys K. Association of microcalcification clusters with short-term invasive breast cancer risk and breast cancer risk factors. Sci Rep. 2019;9(1):1-8.
24. Clemenceau A, Michou L, Diorio C, Durocher F. Breast cancer and microcalcifications: an osteoimmunological disorder? Int J Mol Sci. 2020;21(22):8613.
25. Lewis MC, Irshad A, Ackerman S, et al. Assessing the relationship of mammographic breast density and proliferative breast disease. Breast J. 2016;22(5):541–546.
26. Kosovic V, Krolo I, Zadravec D, Drviš P. Correlation between mammography detected breast arterial calcifications and lifestyle risk factors. Acta Clin Croat. 2015;54(2):143–147.
27. Azam S, Eriksson M, Sjölander A, Gabrielson M, Hellgren R, Czene K, et al. Predictors of mammographic microcalcifications. Int J Cancer. 2021;148(5):1132–1143.
28. Naseem M, Murray J, Hilton JF, et al. Mammographic microcalcifications and breast cancer tumorigenesis: a radiologic-pathologic analysis. BMC Cancer. 2015;15(1):1-9.
29. Karamouzis MV, Likaki?Karatza E, Ravazoula P, Badra FA, Koukouras D, Tzorakoleftherakis E, et al. Non?palpable breast carcinomas: Correlation of mammographically detected malignant?appearing microcalcifications and molecular prognostic factors. Int J Cancer. 2002;102(1):86–90.
30. Anwar SL, Avanti WS, Nugroho AC, Choridah L, Dwianingsih EK, Harahap WA, et al. Risk factors of distant metastasis after surgery among different breast cancer subtypes: a hospital-based study in Indonesia. World J Surg Oncol. 2020;18(1):1-16.
31. Purushotham A, Shamil E, Cariati M, Agbaje O, Muhidin A, Gillet C, et al. Age at diagnosis and distant metastasis in breast cancer–a surprising inverse relationship. Eur J Cancer. 2014;50(10): 1697–1705.
32. Diessner J, Wischnewsky M, Stüber T, Stein R, Krockenberger M, Häusler, et al. Evaluation of clinical parameters influencing the development of bone metastasis in breast cancer. BMC Cancer. 2016;16(1):1-13.
33. Irawan C, Hukom R, Prayogo N. Factors associated with bone metastasis in breast cancer: a preliminary study in an Indonesian population. Acta Med Indones. 2008;40(4):178–180.
34. Coleman R, Smith P, Rubens R. Clinical course and prognostic factors following bone recurrence from breast cancer. Br J Cancer. 1998;77(2):336–340.
Full Text Sources:
Abstract:
Views: 1066

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.