Surgery, Gastroenterology and Oncology

|
|
Materials and Methods: This was a prospective randomized clinical trial that enrolled 90 patients in intensive care units at a University Hospital. Patients were divided into 3 groups critically ill cirrhotic patients with AKI, critically ill cirrhotic patients without AKI and a third control group of critically ill without liver cirrhosis nor AKI. We assessed and compared NGAL, ALP and other parameters in each group.
Results: Liver cirrhosis patients had higher baseline creatinine but within the normal range, high ALT, AST, and NGAL while albumin levels were low significantly. Positive correlations existed between creatinine, NGAL, Alkaline phosphatase and MELD score. NGAL's increase had a stronger AKI association compared to baseline creatinine and albumin decrease. Baseline NGAL proved a superior AKI prediction (AUC 0.98) than creatinine (AUC 0.8) with also higher sensitivity and specificity.
Conclusion: NGAL and ALP have demonstrated to possess great sensitivity and specificity for AKI detection in critically ill cirrhotic patients helping in early starting of suitable therapy for the patients.
INTRODUCTION
Chronic hepatitis C virus (HCV) infection is a major public health concern in Egypt, with an estimate of over 170 million individuals worldwide. The occurrence of renal dysfunction is almost 40% more in HCV patients than in HCV-uninfected patients. Mild to end-stage renal impairment, renal dysfunction typically impacts the outcome and management of HCV infection (1).
Patients with acute decompensated cirrhosis who are hospitalized frequently develop acute kidney injury (AKI) (2). The presence of AKI negatively impacts prognosis, as patients have a high 3-month mortality rate after AKI up to 50%. Various factors, such as associated comorbidities, extent of liver failure, influence the mortality risk. AKI thought to be regarded as a highly consequential outcome of cirrhosis, thereby necessitating proactive measures to mitigate its deleterious effects on the morbidity and mortality rates (2).
Neutrophil gelatinase-associated lipocalin (NGAL) serves as a dependable indicator of injury to the renal tubules. In consequence of nephron injury, the renal epithelium produces this protein. In a variety of circumstances, it is employed to diagnose acute renal damage (3).
NGAL and interleukin-18 (IL-18) are likely to be valuable tools in distinguishing acute tubular necrosis (ATN) from AKI. caused by hepatorenal syndrome (HRS), according to several clinical investigations. In normal conditions, kidney tubular cells produce small amounts of NGAL and IL-18, but injured tubular cells show abundant expression of these proteins. ALP enzyme may be elevated in some liver disease patients (4,5).
This research aimed to evaluate the viability of utilizing NGAL and ALP enzyme as indicators for the detection of AKI and predict the survival in critically ill decompensated cirrhotic individuals with a history of hepatitis C.
MATERIALS AND METHODS
This was a prospective randomized clinical trial that enrolled 90 patients in critical care units at a University Hospital. We enrolled all the patients at their admission to the hospital during the period from January 2022 to January 2023.
Inclusion Criteria
Critically ill patients with post-HCV decompensated liver cirrhosis with or without AKI and control critically ill patients without cirrhosis nor AKI group.
Exclusion Criteria
Patients older than 80 years old, hepatocellular carcinoma beyond Milan criteria, extrahepatic malignancies, major co-morbidities as chronic obstructive pulmonary disease, patients requiring renal replacement therapy, chronic kidney diseases, human immunodeficiency virus infection, previous liver or kidney transplantation, and chronic liver diseases due to causes other than Hepatitis C. Also, we excluded all patients who died during follow up.
Patients Groups
Patients were divided into 3 groups. Group I: Thirty patients with critically ill post-HCV decompensated liver cirrhosis with AKI. Group II: Thirty critically ill post-HCV decompensated liver cirrhosis patients without AKI. Group III: Thirty critically ill patients without cirrhosis nor AKI.
All patients at admission had not AKI, all investigations have been done at admission, cirrhotic critically ill patients that did not develop AKI were enrolled to Group I, cirrhotic critically ill patients who developed AKI were enrolled to the second group. Critically ill Patients with other ICU admission causes cardiac, neurological and surgical who did not develop AKI were enrolled to the third group. Patients were followed up clinical and laboratory for 3 weeks.
Methods
All patients were subjected at admission to ICU to full history taking, clinical examination and laboratory investigations (CBC, serum albumin, AST, ALT, ALP, blood urea, serum creatinine, urine analysis) and serum NGAL. NGAL was measured by ELISA and was withdrawn at 12 hours from hospital admission, at 48 hours from hospital admission and at 7 days after hospital admission. HCV diagnosis was confirmed by electro-chemiluminescence immunoassay (ECLIA), quantitative HCV RNA levels via real-time PCR. AKI in patients were diagnosed according to KDIGO guidelines in 2019.
Statistical Analysis
Data analysis was conducted using SPSS version 28.0 from IBM Inc. Mean ± SD was used to present quantitative data and number (%) for qualitative data and data was compared using independent sample t-test or chi-square test when appropriate. Correlations were evaluated using Pearson's correlation. Logistic regression was utilized for the analysis of the correlations between multiple variables and AKI. The cut-off value of NGAL and baseline creatinine for AKI was determined using ROC curve analysis. The level of statistical significance was established at a p value of less than 0.05.
Ethical Considerations
The data that was obtained from participants was confidential. No participant was identifiable by name in any record or publication pertaining to this study. Before participants were allowed to participate in this study, the objectives, methodology, and risk assessments were given to them. Each participant provided written consent, and the Faculty of Medicine at Menoufia University's ethics board gave its approval.
RESULTS
No statistically significant distinctions were observed between the groups in terms of age and sex. Serum baseline creatinine, ALT, AST, ALP, and NGAL were significantly higher in critically ill cirrhotic patients with AKI compared to cirrhotic patients without AKI and controls. Serum creatinine, ALT, AST, in addition to MELD were also significantly higher in cirrhotic patients with AKI compared to those without AKI. Albumin was significantly lower in cirrhotic patients with or without AKI compared to controls, and it was significantly lower in cirrhotic patients with AKI compared to those without AKI. No statistically significant differences were observed in child Pugh category and presence of ascites between cirrhotic patients with or without AKI (table 1).
Table 1 - Baseline data of the studied groups
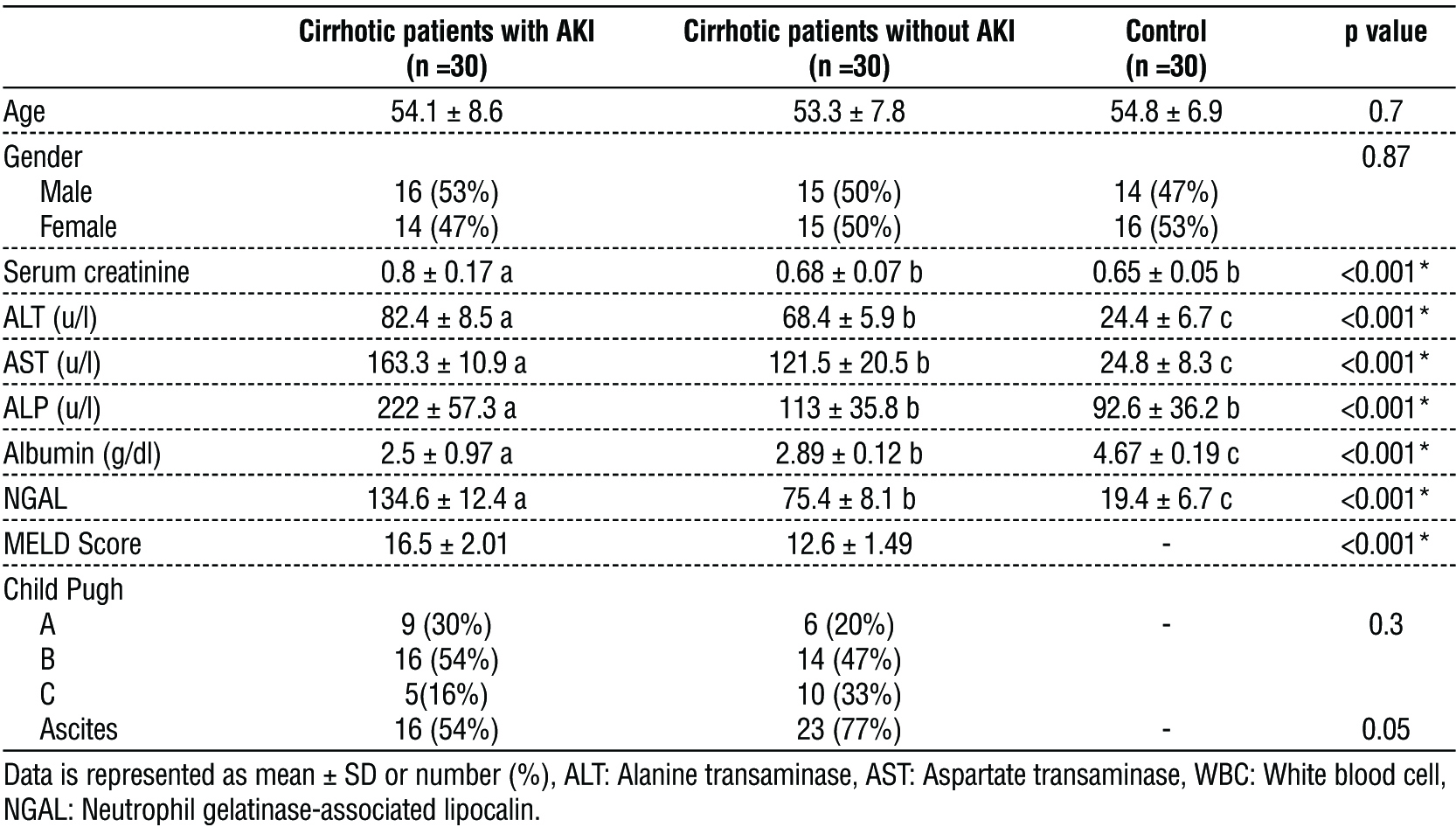
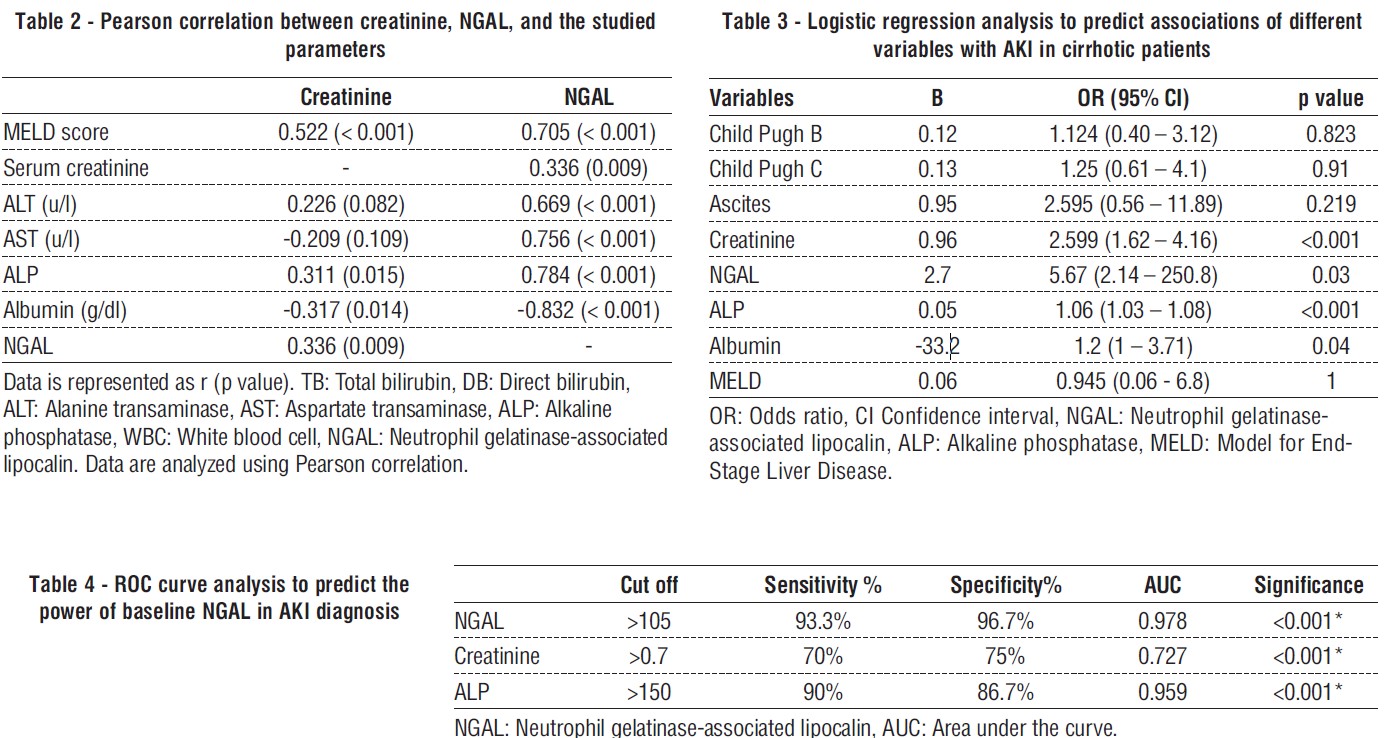
Creatinine showed a significant positive correlation with MELD score, ALP, albumin and NGAL. NGAL levels positively correlated with MELD score, serum creatinine, ALT, AST, ALP, and albumin (table 2).
Of the assessed factors, serum creatinine, NGAL, ALP, and albumin were significant predictors of AKI in critically ill cirrhotic patients. The increase in NGAL levels had a stronger significant association with AKI in cirrhotic patients compared to the increase in baseline creatinine, ALP and decrease in albumin as risk factors for AKI (table 3).
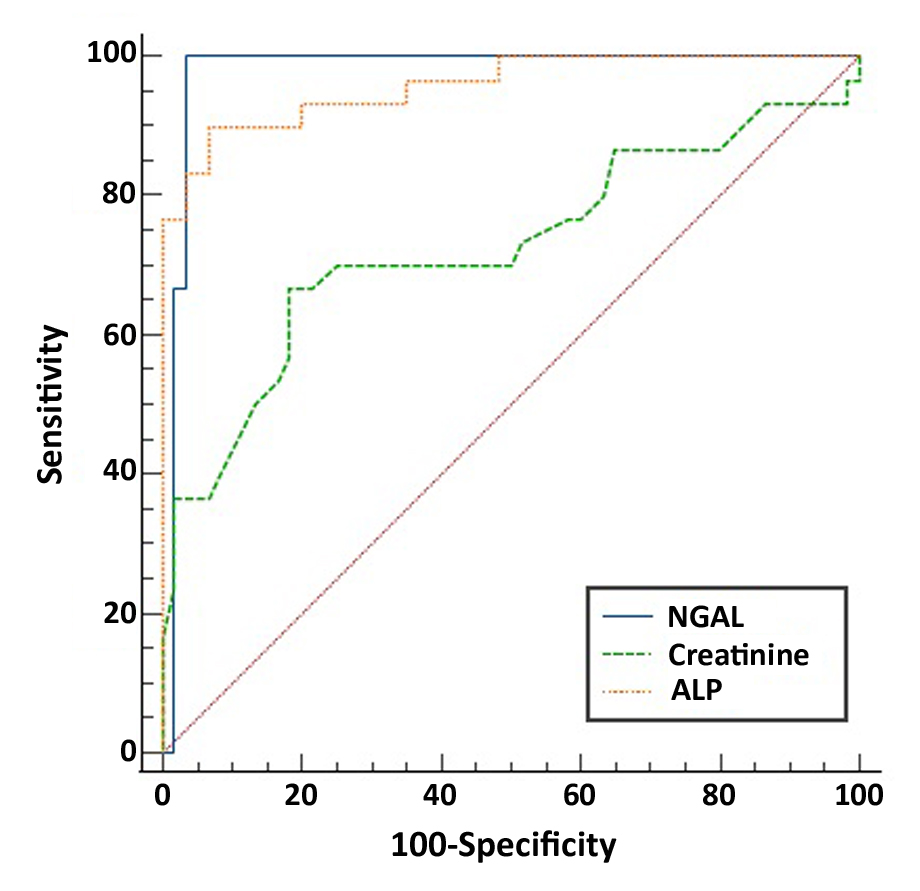
Baseline NGAL was better than baseline creatinine and ALP and could be used as a predictor of AKI in liver cirrhosis patients at level >105 with a sensitivity and specificity of 93.3% and 96.7% respectively, and AUC 0.978 while ALP at >150 IU/L had a sensitivity, specificity, and AUC of (90%, 86.7%, and 0.959) and creatinine at >0.7 had a sensitivity, specificity, and AUC of (70%, 75%, and 0.727) (table 4, fig. 1).
Figure 1 - Ability of NGAL, creatinine and ALP to predict AKI
DISCUSSION
Acute renal injuries are a common occurrence among critically ill patients with decompensated chronic liver disease. These injuries may take on various forms, ranging from pre-renal azotemia to HRS or intrinsic AKI (6).
We demonstrated that critically ill liver cirrhosis patients with AKI had a significantly higher MELD score, while significant differences were observed in the rest of the assessed factors. In agreement with our study, Yewale et al (6) demonstrated that participants with AKI had substantially higher Child-Pugh and MELD scores than patients without AKI with more occurrence of death. Also, Mogawer et al (7) showed a significant increase in MELD levels in the AKI patients.
We found significant differences in baseline biochemical data, worse in critically ill liver cirrhosis patients with AKI than those without AKI and control group. There was a significant increase in serum baseline creatinine, but within normal range, ALT, and AST in cirrhotic patients with AKI, while albumin showed significant decrease. In agreement with our study, Gomaa et al (8) found that when compared to controls, SCr levels were considerably higher in those with renal impairment. Also, Lee et al (9) comparing the groups, the average SCr level was significantly different. Also, Nassar et al (10) showed that as for lab data, the AKI group had considerably greater levels of sCr and NGAL than the non-AKI group.
We showed a substantial difference in baseline NGAL levels between critically ill liver cirrhosis patients with AKI and those without AKI and the control group. Consistent with our research, Yewale et al (6) demonstrated that urine NGAL differed significantly amongst the examined groups. In addition, Sahin et al (11) showed that NGAL was considerably higher in the AKI group as compared to patients with decompensated cirrhosis and no AKI. Furthermore, Gomaa et al (8) shown that the values obtained of NGAL differed significantly amongst all cirrhotic groups. AKI patients had considerably greater levels of NGAL than liver cirrhosis patients without AKI as compared to those without renal impairment.
We demonstrated a positive correlation between creatinine and MELD score, ALP, and NGAL. NGAL demonstrated a positive association with MELD score, serum creatinine, TB, DB, ALT, AST, and ALP, while there was a negative correlation with platelets. In agreement with our study, Yewale et al (6) have demonstrated a significant association between the baseline MELD score and the values of urine NGAL. Also, Gomaa et al (8) demonstrated that significant positive relationships were identified between NGAL and renal function measures such as urea and creatinine.
We showed that an increase of NGAL was significantly associated with AKI in cirrhotic patients than an increase of baseline creatinine, ALP and decrease of albumin and are considered significant contributors to AKI in cirrhotic patients. In agreement with our study, Mohan et al (12) showed that NGAL was a predictive factor of persistent AKI at day 3. Also, Lee et al (9) showed that NGAL level was also a predictor of AKI.
We showed that baseline NGAL was better than baseline creatinine and ALP and as a predictor of AKI in liver cirrhosis patients at a cut-off of >105, it had a sensitivity of 93.3%, specificity of 96.7%, and AUC 0.978 while creatinine at cut-off >0.7 had less sensitivity of 70%, specificity of 75% and AUC 0.727, and ALP at cut-off >150 had a sensitivity of 90%, specificity of 86.7%, and AUC of 0.959.
In agreement with our study, Mohan et al (12) found that the NGAL threshold value that best predicted AKI was 110 g/g creatinine. Also, Sahin et al (11) demonstrated that with an AUC of 0.984, NGAL might be employed to determine AKI in hospitalized cirrhotic patients with AKI with a 91.4% sensitivity and 94.3% specificity at levels ≥ 50 ng/mL. In addition, Jo et al (13) showed that The AUC for NGAL in urine was 0.707. The cut-off threshold for NGAL in urine was 84.8 g/gCr. On the other hand, in Mahfouz et al. study, AUC of 0.64 was observed, along with a sensitivity of 40% and a specificity of 84%. Multiple cutoffs have been proposed for NGAL mostly as a result of discrepancies in research design, condition severity, group numbers, definitions of renal dysfunction, and techniques of data processing. In addition, analyst differences, and the precision of ELISA kits can all impact test findings (14).
CONCLUSION
NGAL has demonstrated to possess great sensitivity and specificity in AKI detection in critically ill cirrhotic patients resulting in early sensible judgments regarding starting suitable therapy to the patients. Also, elevation of alkaline phosphatase is associated significantly with AKI occurrence in cirrhotic patients in ICU.
Conflict of interest
None to be declared.
Funding
None to be declared.
REFERENCES
1. Etik DO, Ocal S, Boyacioglu AS. Hepatitis C infection in hemodialysis patients: A review. World J Hepatol. 2015;7(6):885-95.
2. Huelin P, Piano S, Solà E, Stanco M, Solé C, Moreira R, et al. Validation of a staging system for acute kidney injury in patients with cirrhosis and association with acute-on-chronic liver failure. Clin Gastroenterol Hepatol. 2017;15(3):438-45.
3. Singer E, Schrezenmeier EV, Elger A, Seelow ER, Krannich A, Luft FC, et al. Urinary NGAL-positive acute kidney injury and poor long-term outcomes in hospitalized patients. Kidney Int Rep. 2016; 1(3):114-24.
4. Parikh CR, Mansour SG. Perspective on clinical application of biomarkers in AKI. J Am Soc Nephrol. 2017;28(6):1677-85.
5. Puthumana J, Ariza X, Belcher JM, Graupera I, Ginès P, Parikh CR. Urine interleukin 18 and lipocalin 2 are biomarkers of acute tubular necrosis in patients with cirrhosis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2017;15(7):1003-13.
6. Yewale RV, Ramakrishna BS. Novel biomarkers of acute kidney injury in chronic liver disease: Where do we stand after a decade of research? Hepatol Res. 2023;53(1):3-17.
7. Mogawer MS, El-Shazly MAE-R, Ali AY, Abd El El-Ghany AM, Abd Elhamid S. Novel biomarkers of acute kidney injury following living donor liver transplantation. Saudi J Kidney Dis Transpl. 2020; 31(2):360-7.
8. Gomaa SH, Shamseya MM, Madkour MA. Clinical utility of urinary neutrophil gelatinase-associated lipocalin and serum cystatin C in a cohort of liver cirrhosis patients with renal dysfunction: a challenge in the diagnosis of hepatorenal syndrome. Eur J Gastroenterol Hepatol. 2019;31(6):692-702.
9. Lee JH, Yoon EL, Park SE, Park JY, Choi JM, Jeon TJ, et al. Clinical significance of urinary neutrophil gelatinase-associated lipocalin levels in defining the various etiologies of acute kidney injury in liver cirrhosis patients. Korean J Gastroenterol. 2019;74(4):212-8.
10. Nassar DK, Elkenawy MF, El-Naggar MM, Khalil E-SA-M, Barakat GI. Neutrophil Gelatinase-Associated Lipocalin (NGAL): An Early Dual Biomarker in Diagnosis of Ascitic Fluid Infection and Acute Kidney Injury in Liver Cirrhosis in a Tertiary Centre, Egypt. J adv microbiol. 2021;20(12):95-107.
11. Sahin E, Handiri E, Altay DU. POSTER PRESENTATION ABSTRACTS. Turk J Biochem. 2020;45(S2):65-83.
12. Mohan PB, Nagaraju SP, Rangaswamy D, Musunuri B, Attur RP, Bhat G, et al. Urinary neutrophil gelatinase-associated lipocalin: Acute kidney injury in liver cirrhosis. Clinica Chimica Acta. 2021; 523339-47.
13. Jo SK, Yang J, Hwang SM, Lee MS, Park SH. Role of biomarkers as predictors of acute kidney injury and mortality in decompensated cirrhosis. Sci Rep. 2019;9(1):14508.
14. Mahfouz MH, Assiri AM, Mukhtar MH. Assessment of neutrophil gelatinase-associated lipocalin (NGAL) and retinol-binding protein 4 (RBP4) in type 2 diabetic patients with nephropathy. Biomark Insights. 2016;1131-40.
Full Text Sources:
Abstract:
Views: 2072

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.