Surgery, Gastroenterology and Oncology
|
|
A young gentleman presented with one day history of severe right sided abdominal pain with no other relevant history and normal blood work. Diagnostic laparoscopy revealed an omental infarct and resection was performed. He was well post operatively and discharged the following day.
BACKGROUND
Omental infarct is a rare cause of abdominal pain and usually has a similar presentation to appendicitis, cholecystitis, or diverticulitis. The first diagnosis of omental infarction was made by Bush in 1986 and since then, approximately 400 cases had been reported (1-3). This case report aims to discuss on the importance of keeping this rare diagnosis in mind as one of the differentials for patients presenting with severe right sided abdominal pain and normal biochemical markers.
CASE PRESENTATION
A gentleman in his 20s presented to Emergency Department with 1 day history of severe right iliac fossa pain with no other positive relevant history suggestive of urinary tract infection, trauma, or diverticulitis. The patient was otherwise fit and healthy prior to this presentation. Physical examination elicited right iliac fossa tenderness, but Rovsing sign was negative. There were no signs of an abdominal masses or hernia. Being a young and otherwise healthy male with localised right iliac fossa tenderness, early operative management was considered in the suspicion of acute appendicitis.
Clinical Features
Investigations
Full blood examination and C Reactive protein were within normal ranges. Ultrasound abdomen was unable to identify the appendix, however, no other source of abdominal pain was identified either.
Differential diagnosis
1. Acute appendicitis;
2. Diverticulitis;
3. Right renal calculus;
4. Epiploic appendagitis.
Treatment
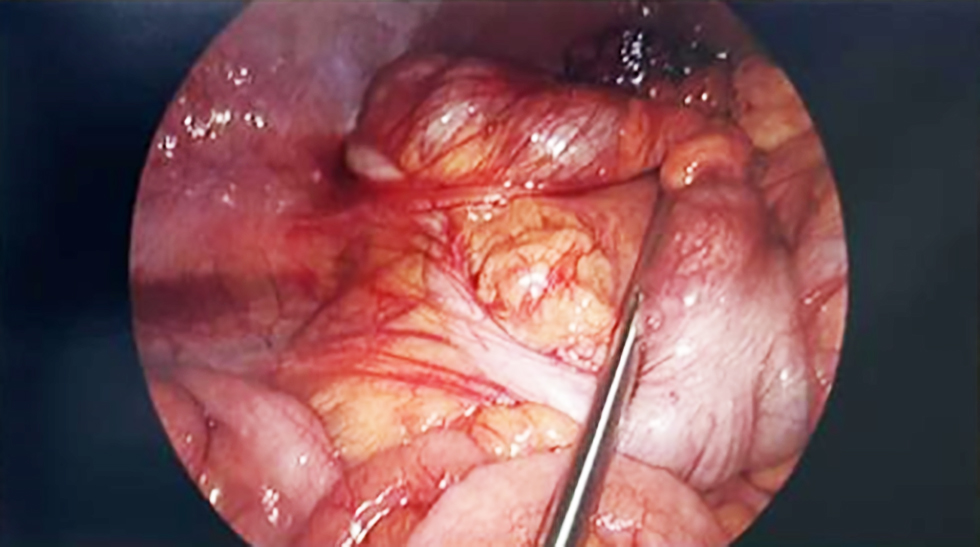
The patient was initially treated with fluid resuscitation and analgesia. He was brought to the operating theatre for a diagnostic laparoscopy due to persistent right iliac fossa pain despite conservative treatment. Intraoperatively, an omental infarct was seen in the right upper quadrant region with the anterior portion adhered to the anterior abdominal wall, and appendix appeared healthy as shown in fig. 1 and fig. 2.
Figure 1 - A segment of infarcted omentum was identified and dense adherence to the anterior abdominal wall which was released during laparoscopic procedure
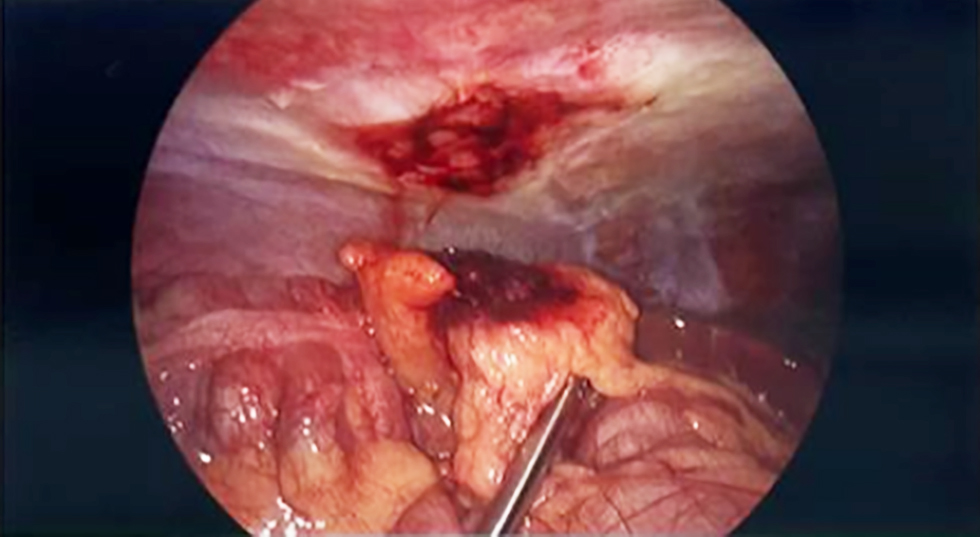
The infarcted portion of the omentum was dissected bluntly from the anterior abdominal wall and sub-sequently resected with adequate haemostasis. The cause of the omental infarct was unclear, as there was no obvious torsion, and no other stigmata of embolism.
Outcome and Follow-up
Patient recovered well post operatively and was discharged on the following day. Histopathology reported as omental infarction. Follow up was done 2 weeks post operatively, patient was pain free and able to conduct daily activities with no issue.
Figure 2 - Laparoscopic view demonstrating a macroscopically normal appendix with no evidence of inflammation, perforation, or surrounding exudate
DISCUSSION
Omental infarction is a rare cause of acute abdominal pain. Regarding idiopathic omental infarction, the literature has reported only 400 known cases (1). Patients usually present with abdominal pain that mimics appendicitis and cholecystitis, making the diagnosis more challenging. This case has highlighted the diagnostic challenge of differentiating omental infarct from appendicitis leading to unnecessary surgical intervention (4). Bush was the first to describe a case of omental infarction associated with a traumatic event, whereas Eitel was the first to report omental torsion as the primary cause of infarction (2,5). The diagnosis of idiopathic omental infarction is made when no identifiable primary cause is found, as in the case being reported here.
The pathology of omental infarction remains unclear. Some theories suggest that poor blood supply leads to venous congestion, hemorrhage, and necrosis of part of the omentum. Secondary causes of omental infarction have been postulated to result from pathological foci such as inflammation and neoplasm (7). Over the past decade, a few case reports have highlighted the difficulty of diagnosing omental infarction due to its rarity and its tendency to mimic other abdominal pathologies, such as appendicitis and cholecystitis (8-10).
There is no global consensus on the optimal treatment for omental infarction. However, Medina-Gallardo and colleagues conducted a systematic review of case series, suggesting that the majority of surgeons opt for conservative treatment, as it is a self-limiting disease. However, conservative management has been associated with longer hospital stays compared to surgical intervention. There is strong support on both surgical and conservative approach however they are very diagnosis-dependent. Limitations still exist in the conservative approach is due to diagnostic uncertainty and persisting symptom despite conservative management which eventually leads to explorative surgery (11). In our present case, we have a patient presenting with an appendicitis-like symptom with the absence of pre-operative imaging leading to surgical intervention. Alternative management would be an imaging to determine the actual abdominal pathology contributing to patient’s presentation whereby diagnosis accuracy can be improved and possibly facilitating non-operative management instead.
The absence of CT imaging represents a limitation as cross-sectional imaging would have been able to delineate abdominal pathology and avoiding surgical intervention. The decision to operate was decided solely based on established surgical principles prioritising early management of acute appendicitis to avoid complications such as perforation. This case report highlights the underappreciation of omental infarct as a differential diagnosis and value of early imaging which may improve accuracy and possibly avoiding surgery.
CONCLUSION
In conclusion, neither surgical nor conservative management holds a more superior benefit. Instead, management should be individualised, incorporating clinical assessment, imaging where appropriate, and consideration of patient-specific factors. Further studies are needed to establish clearer guidelines for the diagnosis and management of omental infarction.
Learning Points
1. Keeping unusual diagnoses such as this in mind when assessing patients presenting with atypical but severe right sided abdominal pain.
2. Omental infarct is a rare cause for acute abdominal pain.
3. Clinical assessment outweighs biochemical markers.
Patient’s Perspective
The patient reported significant improvement in symptoms following surgery and expressed gratitude for the intervention. He was surprised by the intra-operative finding of omental infarction, having initially believed his symptoms were due to appendicitis based on discussions with peers.
Conflict of Interest
No conflict of interest.
Ethical Statement
Not required.
REFERENCES
1. Buell KG, Burke-Smith A, Patel V, Watfah J. Omental Infarction: The Great Impersonator. Cureus. 2017;9(12):e1940.
2. Kataoka J, Nitta T, Ota M, Takashima Y, Yokota Y, Fujii K, et al. Laparoscopic omentectomy in primary torsion of the greater omentum: report of a case. Surg Case Rep. 2019;5(1):76.
3. Medina-Gallardo NA, Curbelo-Peña Y, Stickar T, Gardenyes J, Fernández-Planas S, Roura-Poch P, et al. Omental infarction: surgical or conservative treatment? A case reports and case series systematic review. Ann Med Surg (Lond). 2020;56:186-193.
4. Paroz A, Halkic N, Pezzetta E, Martinet O. Idiopathic segmental infarction of the greater omentum: a rare cause of acute abdomen. J Gastrointest Surg. 2003;7(6):805-8.
5. Eitel G.G. Rare omental torsion. NY Med Rec. 1899;55:715.
6. Diab J, Badiani S, Berney CR. Diagnosis and Management of Adult Omental Infarction: 10-Year Case Series. World J Surg. 2021;45(6): 1734-1741.
7. Singh AK, Gervais DA, Lee P, S Westra, Hahn PF, Novelline RA, et al (2006) Omental infarct: CT imaging features. Abdom Imaging. 2006;31(5):549-54.
8. Buell KG, Burke-Smith A, Patel V, Watfah J. Omental Infarction: The Great Impersonator. Cureus. 2017;9(12):e1940.
9. Que Son T, Hieu Hoc T, Duc Long V, Thanh Tung T, Van Tuyen P, Toan Thang N, et al. Laparoscopic Surgery for Diagnosis and Treatment of Acute Right Upper-Quadrant Abdominal Pain Due to Omental Infarction: A Report of a Rare Case in a Single Vietnamese Hospital. Am J Case Rep. 2021;22:e931098.
10. Miu K, Yousef M, Siddika A. Omental infarction mimicking acute appendicitis with negative radiological findings. BMJ Case Rep. 2023;16(3):e254340.
11. Itenberg E, Mariadason J, Khersonsky J, Wallack M. Modern management of omental torsion and omental infarction: a surgeon's perspective. J Surg Educ. 2010;67(1):44-7.
Full Text Sources:
Abstract:
Views: 283

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.