Surgery, Gastroenterology and Oncology

|
|
Objective: To evaluate the effectiveness among two incisional negative pressure wound
therapy (iNPWT) devices (Prevena™ and PICO™) and compare them with conventional dressings in preventing surgical site occurrences (SSOs), particularly surgical site infections (SSIs), in patients undergoing emergency laparotomies. Summary Background data: Surgical site occurrences (SSOs), particularly infections, are prevalent post-surgery complications, increasing morbidity and healthcare costs. The prophylactic use of advanced wound dressings such as Prevena™ and PICO™ are acclaimed for preventing SSOs. However, there is limited comparative data amongst devices regarding their effectiveness, especially in emergency surgeries which present a high risk for SSOs due to various patient-related factors.
Methods: We conducted a randomized controlled trial over a 1-year period. Patients undergoing urgent laparotomy were randomly assigned to Prevena™, PICO™ or conventional dressings. Data on patient demographics, risk factors, and procedural details were collected, with a 30-day post-operative follow-up to monitor primary (SSIs) and secondary outcomes (SSOs, length of stay, complications, reinterventions, readmissions, and mortality).
Results: A total of 123 patients were analyzed post-randomization exclusions. The Prevena™ and PICO™ groups demonstrated a significant reduction in SSIs and overall SSOs compared to the conventional dressing group. No significant differences were observed in other post-operative complications, reinterventions, readmissions, or mortality rates across the groups.
Conclusion: Prevena™ and PICO™ were more effective than conventional dressings in preventing SSOs and SSIs in emergency laparotomy patients. The study found no statistically significant differences between the two iNPWT devices in terms of overall wound complications, suggesting that device choice can be guided by cost and user experience without compromising clinical outcomes. Further studies are recommended to validate these findings.
INTRODUCTION
Surgical site occurrences (SSOs), particularly surgical site infections (SSIs), rank among the most prevalent complications following surgical procedures, especially when considering open approaches (1-3). These complications can prolong hospital admissions, increase healthcare expenditures and morbidity rates, while adversely affecting patient outcomes (1-3). This is notably evident in emergency laparotomies. The urgent nature of such procedures can inherently heighten the risk of SSOs, especially when combined with the compromised physiological status of an acutely ill patient (4).
Over recent years, advancements in wound management have introduced innovative dressings designed to minimize the post-operative risk of SSOs. Among these, Prevena™ (KCI Inc, San Antonio, TX, USA) and PICO™ (Smith & Nephew Inc, Andover, MA, USA) wound dressings have emerged as leading contenders, lauded for their advanced technology and efficacy in reducing SSOs rates (5,6). Prevena™, an incisional negative pressure wound therapy (iNPWT) system, maintains a sealed environment over the surgical incision, reducing edema and fluid accumulation by active drainage to a portable cannister (7). PICO™ offers the added advantage of simplicity, with fluid accumulating directly within the dressing system while maintaining a dry wound (8). Both devices provide different pressure to the wound, distinct means of fluid accumulation and have disparate costs (7, 8).
Although both Prevena™ and PICO™ are single-use iNPWT dressings gaining acceptance in the surgical field, a paucity of direct comparative data remains when evaluating their efficacy, particularly in the context of emergency laparotomies. Most of the existing studies focus on specific surgical subgroups or have limited sample sizes (5, 9-11). Furthermore, while these advanced dressings present promising results, understanding how each system compares with the other and with conventional dressings in real-world scenarios, especially in patients undergoing emergency procedures, who often present with high risk profiles for SSOs, is imperative (12).
Our study aims to provide a comprehensive analysis comparing the effectiveness of Prevena™, PICO™, and conventional dressings in preventing SSOs, with a primary focus on SSIs, in patients undergoing emergency laparotomies. By incorporating patient and procedure-related risk factors into our analysis, we intend to contribute to a better understanding on the potential benefits and limitations of each dressing type.
METHODS
Setting
The trial was conducted at Centro Hospitalar do Tâmega e Sousa, E.P.E, a secondary care hospital in Portugal. The study adhered to CONSORT guidelines and was registered on www.clinicaltrials.gov (NCT05716490) after local ethics committee approval. All patients, or legal guardians when needed, signed an informed consent before surgery.
Patient selection and randomization
Patient recruitment occurred between 1st July 2022 and 1st August 2023 and included adult patients, diagnosed in the emergency department or General Surgery ward requiring urgent laparotomy. Exclusion criteria are bellow outlined:
- Contraindications for iNPWT (incomplete abdominal wall closure, difficult wound hemostasis);
- Recent surgical history by same approach (within 90 days);
- Imminent mortality due to irreversible disease (such as extensive mesenteric ischemia);
- Those needing staged surgical procedures (second-look or clip-and-drop strategies).
An initial 1:1:1 allocation sequence was designed for two intervention groups (Prevena™ and PICO™ wound dressings) and one control group using online software from www.graphpad.com. The lead surgeon enrolled patients sequentially, updating the allocation table post-surgery. No blinding or allocation concealment occurred.
Following skin suture with surgical staples at the end of the procedure, each patient had a specific wound dressing applied according to the group they have been randomized into. All surgeries began with the WHO safe surgery checklist and concluded with patients adhering to the standard local wound care bundle. Abdominal wall closure was performed using monofilament material with continuous suturing mass closure, using small bites technique.
- Prevena Group: The Prevena™ dressing was applied and maintained for 7 days, with variations based on patient needs and suspicion SSO development.
- PICO Group: Post-laparotomy, the PICO™ dressing was applied and maintained for 7 days. As the PICO™ kit comes with an additional dressing, the wound was revised and the dressing changed between 3rd and 4th post-operative day or even earlier if suspicion of SSO occurred.
- Control group: A conventional dressing, comprised of a waterproof sterile dressing was used, with standard dressing exchange every 2 days, unless fluid accumulation within the dressing or signs of inflammation around the dressing was apparent.
Outcomes
Data was collected on both pre-operative (including patient demographics, admission date, and SSO risk factors) and intra-operative details (definitive diagnosis, surgical procedure, operative duration, spillage, surgical drain necessity, prophylactic antibiotic use, and the type of wound dressing).
The primary outcome was defined as surgical site infection diagnosed as cellulitis around the wound with other signs of infection (fever, elevated C-reactive protein or leukocystosis), purulent wound discharge (regardless of other findings) or identification of bacteria in fluids collected from wound when infection was suspected but not definitive.
Secondary outcomes encompassed surgical site occurrences (SSOs), including seroma, hematoma, and wound dehiscence. Since SSOs involve a dynamic interacting spectrum of wound complications (such as infection leading to wound dehiscence) we opted to register the main SSO for each patient. Other secondary outcomes include fascial dehiscence, length of stay (LOS), surgical complications, reinterventions, readmissions and mortality.
All study participants, underwent a 30-day post-operative monitoring. Should a reintervention be necessary, the focus shifted to only monitoring wound-related outcomes up to that intervention. Patient’s daily care, therapeutic decisions, and diagnostic requirements were managed by the designated surgical team, which always included at least one research team member. Patients discharged under a week post-
surgery had scheduled 2-week and 30-day follow-up appointments with the research team, while those discharged between 15 to 30 days post-surgery had only the 30-day appointment.
Statistical analyses
Frequency distributions are reported as absolute number and percentages for categorical variables, while measures of central tendency (means) and variability (standard deviation) were used for continuous variables, after confirming normal distribution of the samples in their respective histograms. To compare such variables within 3 groups, analysis of variance (ANOVA) test was performed and an independent samples T-test was used to compare among 2 groups. Categorical variables across groups were compared using the Chi-square frequency test. To determine effect size we used Cramer’s V for Chi-square frequency test, partial ETA squared for ANOVA test and Cohen’s D for independent samples T test. A significance level of 5% (p ≤ 0,05) was considered for all tests. Data analysis was carried out using IBM® SPSS Statistics® version 29.0 for Macintosh (IBM, Corp, Armonk, New York, United States of America).
RESULTS
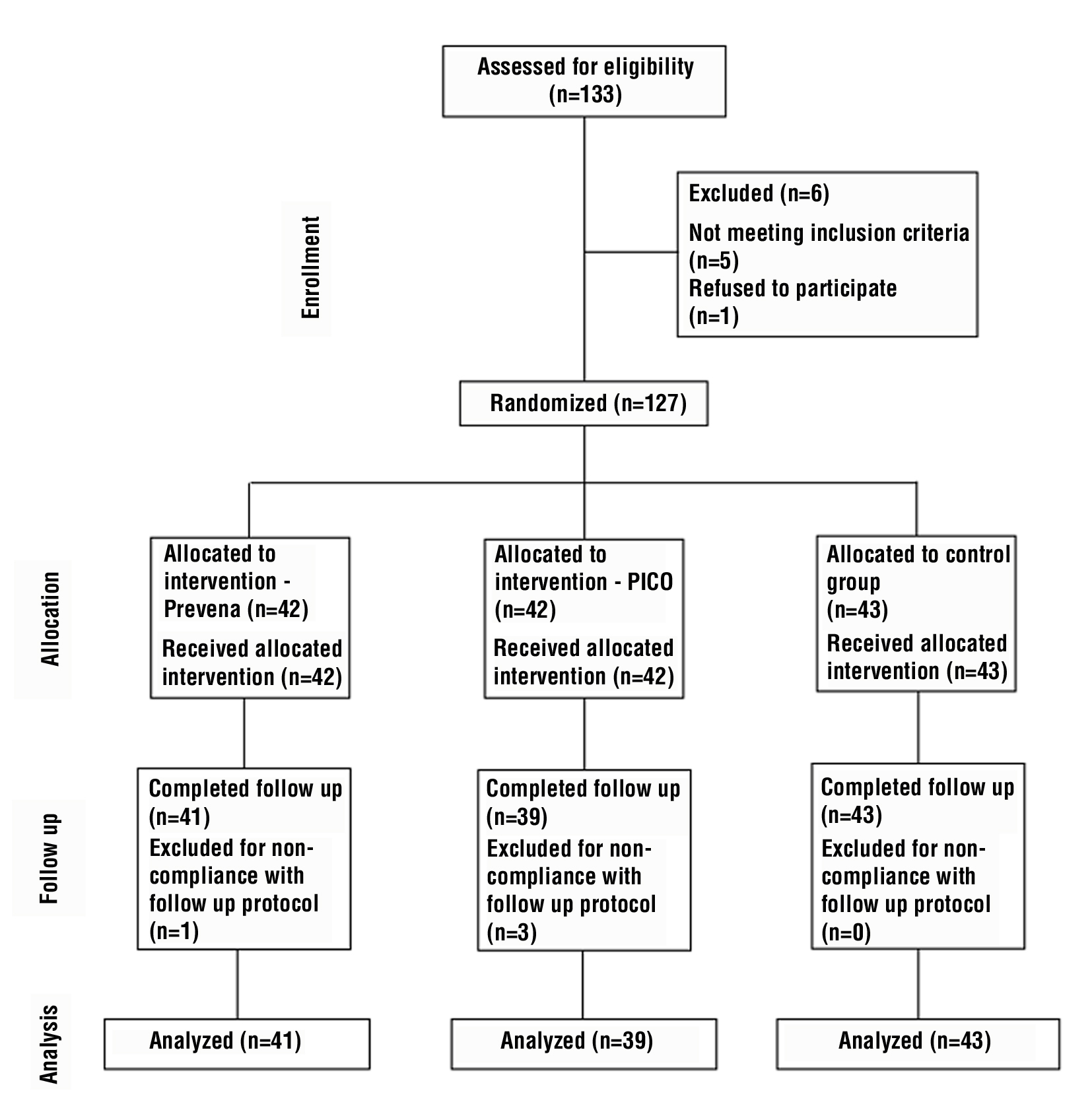
A total of 133 were assessed for eligibility during the study period. Of these, 1 patient refused to participate, and 5 patients failed to meet inclusion criteria. Following informed consent, 127 patients were randomized into the 2 interventional groups (Prevena and PICO) and 1 control group (conventional dressings). 42 patients were allocated to Prevena group, 42 to the PICO group and 43 in Control group. During follow-up 4 patients (1 in Prevena group and 3 in PICO group) did not comply with protocol and were later excluded. We analysed 123 patients (41 in Prevena group, 39 in PICO group and 43 in Control group) (fig. 1).
Figure 1 - Consort Flow diagram (Randomization and allocation of patients)
General cohort analysis
Demographics and patient related risk factors (table 1).
Table 1 - Patient demographics and patient related risk factors distribution
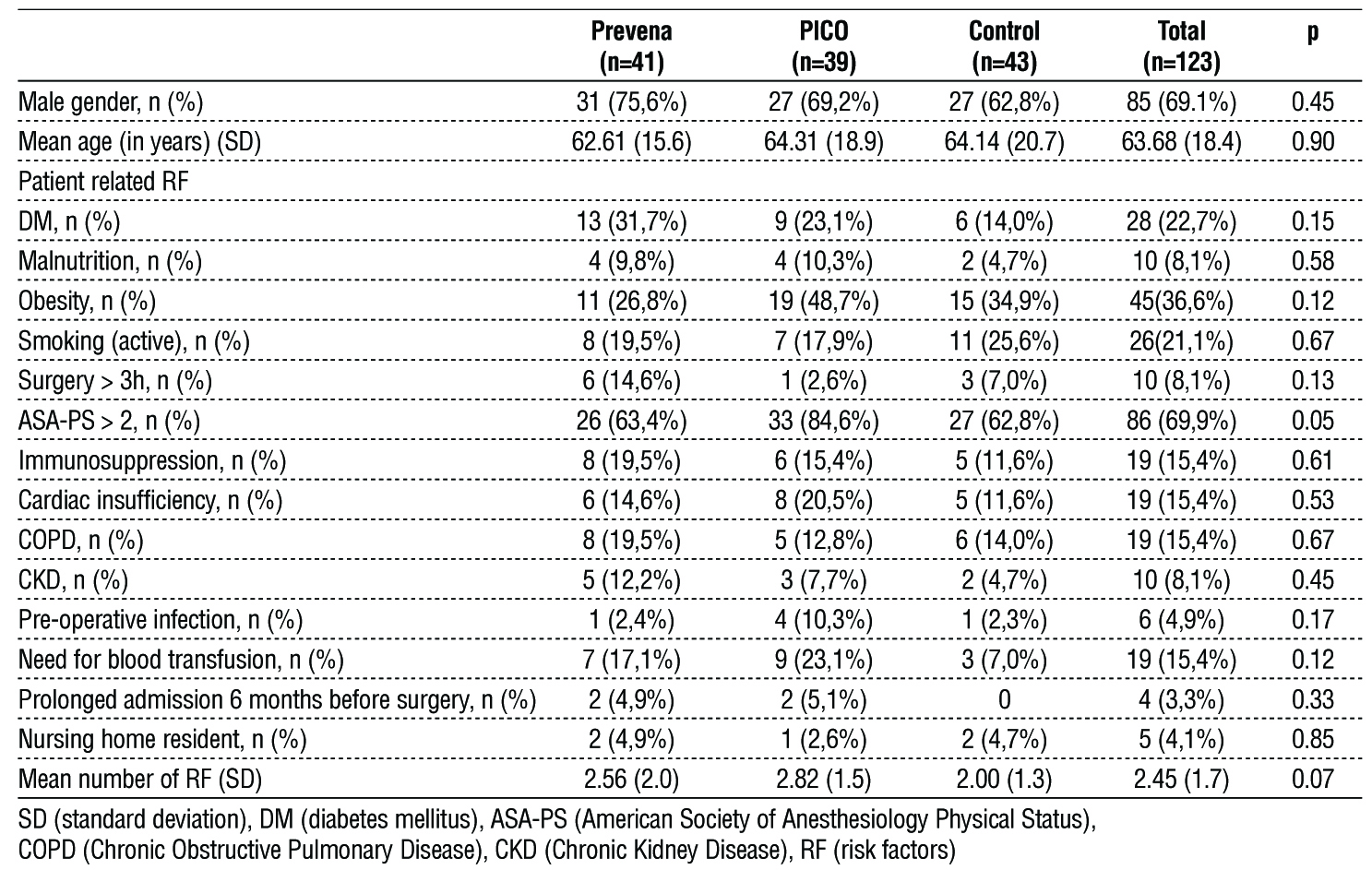
Gender distribution was consistent across the three groups, with the Prevena group comprising 75,6% males, the PICO group at 69,2%, and the Control group at 62,8%, showing no significant difference (p = 0.45). Likewise, the age profile of the participants was similar, with an overall mean age of 63.68 years, and the differences among groups were not statistically significant (p = 0.90).
A noteworthy observation was the predominance of patients with an ASA-PS (American Society of Anesthesiology Physical Status) score greater than 2, particularly in the PICO group (84,6%, p = 0.05). Other risk factors, such as diabetes mellitus, malnutrition, and obesity, demonstrated no statistically significant differences across the cohorts. Furthermore, when considering the average number of combined risk factors, the Prevena group had 2.56, the PICO group 2.82, and the Control group 2.00, highlighting a comparable risk profile of participants in our study (p = 0.07).
Diagnosis and procedure related factors (table 2). The distribution of diagnosis throughout the groups showed no statistically significant differences (p = 0.64). Intestinal occlusion was the most frequent reason for intervention (48,8%), followed by abdominal sepsis (26,0%) whereas gastrointestinal bleeding was the least.
Table 2 - Procedure related risk factors distribution; RF (risk factors), ICU (Intensive Care Unit)

Wound classifications by the World Health Organization (WHO) showed comparable rates for 'Clean' across the groups. 'Clean-contaminated' was most prominent in the Control group at 37,2%, whereas 'Contaminated' and 'Infected' categories were the most frequent across Prevena and PICO groups, with both above 28%. No statistically significant differences among groups was found (p = 0.22).
In procedure-related risk factors, drain usage was prevalent across groups, peaking at 76.7% in Control group (p = 0.53). Notably, the Prevena group had a distinctively higher need for a stoma creation (41.5%) when compared to PICO and Control group (p = 0.01).
Wound related and general morbidity and mortality (table 3).
Table 3 - Wound and general morbidity and mortality
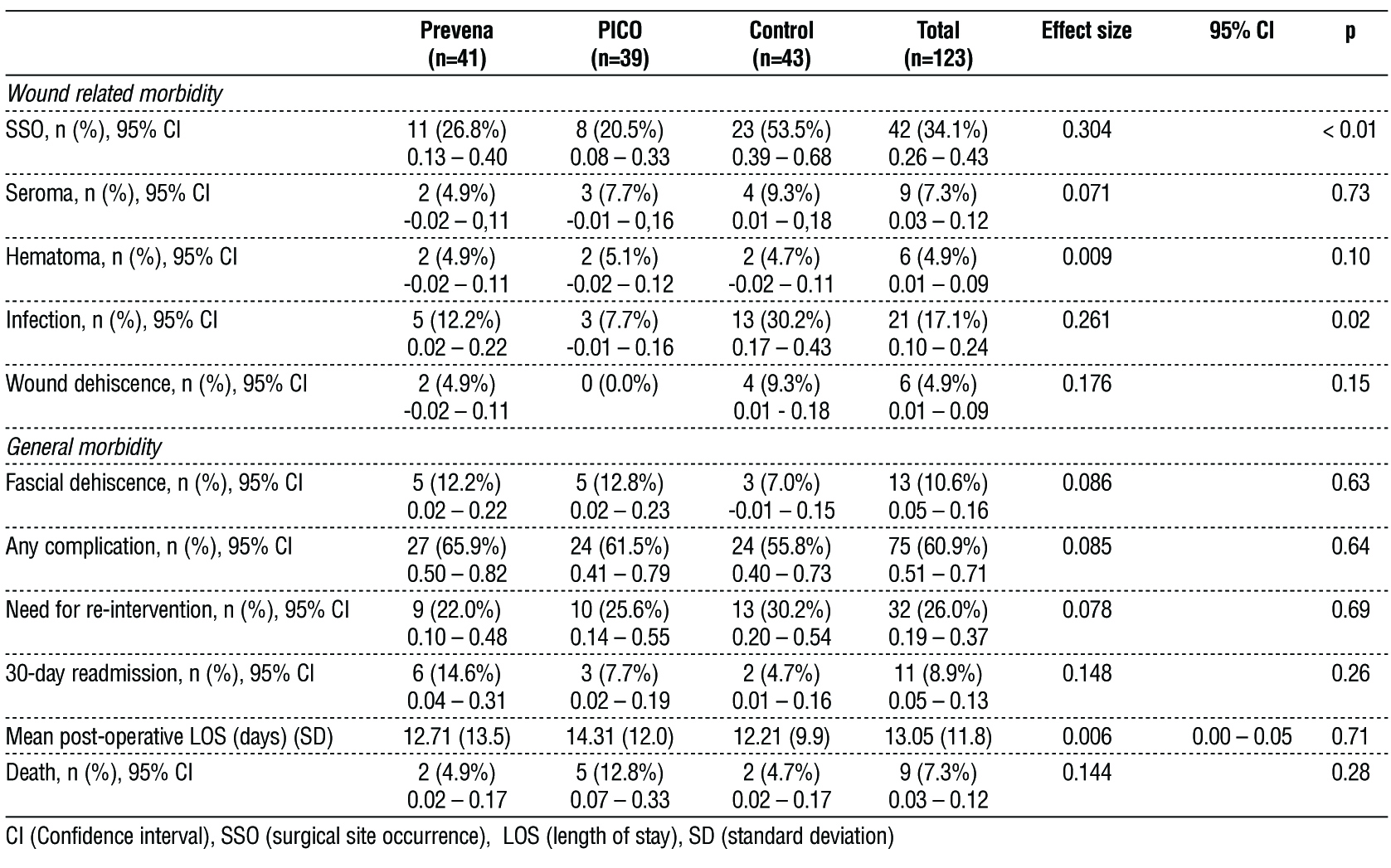
Within wound-related morbidity, the Control group had the highest rate of surgical site occurrences (SSOs) at 53,5%, compared to 26,8% in the Prevena group and 20,5% in the PICO group (p < 0.01). Additionally, the Control group showed a notably elevated incidence of infection at 30,2%, in contrast to 12,2% in the Prevena group and 7,7% in the PICO group (p = 0.02).
No statistically significant differences in general morbidity, namely for the rate of surgical complications and need for reintervention, post-operative length of stay (LOS) and mortality.
Direct comparison between iNPWT devices (table 4).
Table 4 - Outcome comparison between Prevena and PICO groups
In a comparative analysis between the Prevena and PICO wound management systems, surgical site occurrences (SSO) were observed in 26.8% of patients in the Prevena group and 20.5% in the PICO group (p = 0.51). Specific wound complications also showed no statisticaly significant differences between the Prevena and PICO groups including seroma (4.9% vs 7.7%, p = 0.60), hematoma (4.9% vs 5.1%, p = 0.96), and infection (12.2% vs 7.7%, p = 0.50). Wound dehiscence was exclusive to the Prevena group at 4.9% (p = 0.16).
For general morbidity outcomes, fascial dehiscence was observed in 12.2% of Prevena patients and 12.8% of PICO patients (p = 0.93). Overall complication rates were slightly higher in the Prevena group at 65.9%
compared to 61.5% in the PICO group (p = 0.69). The need for reintervention was slightly higher in the PICO group (25.6% vs. 22.0%, p = 0.48) and the 30- day readmission rate was lower in the PICO group at 7.7%, compared to 14.6% in the Prevena group (p = 0.33).
The average post-operative length of stay (LOS) was slightly longer for the PICO group (14.31 days vs 12.71 days, p = 0.77). Mortality was higher in the PICO group at 12.8% versus 4.9% in the Prevena group (p = 0.21).
DISCUSSION
Our study aimed to assess the effectiveness of iNPWT in reducing wound related morbidity, measured as the development of SSIs and other SSOs, in patients undergoing emergent laparotomy for various causes. We observed a statistically significant reduction in SSIs (p = 0.02) and SSOs (p < 0.01) with the use of iNPWT devices, among comparable cohorts in terms of patient and procedure related risk factors. When comparing only the devices, no statistically significant differences were found between them.
Emergency laparotomy cases encompass a group of pathologies with different etiologies and degrees of wound contaminations but sharing an increased likelihood for SSIs due to greater contamination and reduced physiological condition. Consequently, several societies have made recommendations for iNPWT use in this context (1,12). Our data supports this recommendation, as the use of iNPWT led to lower rates of SSIs and SSOs when comparing to conventional dressings.
The World Society of Emergency Surgery stated that due to lack of data, no recommendation on type of iNPWT device could be made (12). To our knowledge, this is the first RCT comparing the performance of 2 iNPWT devices – PICO™ and Prevena™. We found no differences in outcomes between the groups despite important mechanical differences (including different pressure levels and fluid accumulation mechanisms) which also translate to differences in pricing. According to the National Institute for Health and Care Excellence (NICE) in the United Kingdom, a standard Prevena™ kit costs £299 to £351 and £179 to £233 for an additional dressing if needed (7), PICO™ standard kit cost ranges from £127.06 to £145.68 and comes with 2 dressings available (8). In our institution PICO™ kits prices range from 123€ to 141€ while Prevena™ kits vary from 250€ to 450€. The fact that PICO™ kit comes with an additional dressing at no extra cost is of particular importance in the setting of emergency procedures as patients are at higher risk of reintervention, allowing to continue wound therapy without additional costs. However, oversaturation of the PICO™ dressing, an event less likely with Prevena™ system which drains to a portable canister, might constitute an increase in costs, especially in discharged cases, as the patient must return to the outpatient for a dressing switch. Moreover, patients undergoing emergency laparotomy are also at increased risk of fascial dehiscence which could be suspected by an unexpected increase in fluid drainage but could be masked by iNPWT as no wound inspection or exploration can be made. While the incidence of fascial dehiscence showed no differences among the 3 groups (p = 0.63) makes the use of iNPWT safe, the possibility to switch dressings and evaluate the wound at no added cost mid-therapy is another advantage from the PICO kit, allowing for early diagnosis and treatment. Altogether PICO™ dressings seem to be more cost efficient than Prevena™, given the higher cost without a commensurate improvement in outcomes with the Prevena™ dressing.
The patient cohorts of Prevena, PICO, and Control groups showed no statistically significant differences in terms of demographics and risk factors, ensuring robust comparability. Moreover, applying the same wound care bundle to all patients, established a consistent baseline for intervention analysis. Outcomes were measured for 30-days with protocol defined dates for inpatient and outpatient observations from the study team, reducing observation bias. Cheong Chung et al (11) conducted a prospective cohort study comparing the rates of SSI in patients with and without iNPWT using the Prevena system among 474 patients. Similarly to our results, they found decreases in surgical site infection (16.9% vs 33.8%, p < 0.01), despite having a greater proportion of colorectal resections and a higher physiological and a greater operative severity score for the enumeration of mortality and morbidity (POSSUM) in the Prevena group, probably due to surgeons preference for iNPWT in higher risk patients.
Kabir et al (13) retrospectively analyzed 152 cases of emergency laparotomies in trauma context comparing wounds managed with standard dressings (n=79) or iNPWT (n=73). The study, unlike ours, failed to show a statistically significant difference in rates of SSI between groups (p = 0.15). While our sample contains a lower number of trauma laparotomies (n = 10, 8.1%), this finding might be due to different methodology as Kabir et al defined only 5 days of iNPWT vs 7 days in Optiwound which could further potentiate its benefits. The authors found however a statistically significant decrease in SSIs on patients with full thickness bowel injury (p = 0.03) (those at greater risk for wound complications) and a significant reduction in wound dehiscence in patients managed with iNPWT overall (p = 0.02), emphasizing the benefits of iNPWT even with a shorter duration of therapy.
A recent meta-analysis (14) on emergency laparotomies setting indicated a lower risk of wound breakdown including fascial dehiscence with iNPWT (OR 0.36, 95% CI 0.19-0.72, p < .01). This finding was based on a metanalysis of 3 studies (10,13,15) which report on wound breakdown and fascial dehiscence as the same outcome, which raises caution when using iNPWT to enhance such outcomes. In our study we did not observe any benefit besides a decreased rate of SSIs and global SSOs, suggesting limited effectiveness of iNPWT beyond superficial wound outcomes.
This is the first RCT comparing 2 different iNPWT devices. The methodology of the working group on monitoring the outcomes for 30 days also accounts for a thorough report of the outcomes, allowing for reliable interpretation.
An alpha of 0.05 was considered, in line with current practices in medical field, with a power of 70% which we recognize could yield a higher probability (30%) of a type II error. A minimum of 50 patients per arm would be required to achieve a power of 80%. While we recognize the low number of cases as a potential limitation of our study, it accurately reflects the reality of a secondary center in Portugal. Moreover, the incidence of laparotomy has drastically diminished due to the implementation of laparoscopic surgery in the emergency context.
Having only one center involved in the study might limit the generalizability of our findings as the outcomes will depend not only on wound dressings but also on local bundles of care and patients’ particularities. The addition of a control group mitigates this potential limitation by setting our standard of care with conventional wound dressings allowing to assess results of implementation of a new device.
In light of the current findings, it is recommended that additional RCTs be conducted to enhance the evidentiary base regarding the distinctions among various iNPWT devices, particularly with an emphasis on cost-effectiveness, which might be a prominent factor in this context. Moreover, there is a need for further research to evaluate the efficacy of these devices in outcomes not directly associated with wound healing, such as length of stay (LOS) and fascial dehiscence, contributing to a more comprehensive understanding of the utility and potential expansion of indications for iNPWT devices in clinical practice.
CONCLUSION
We concluded iNPWT to be efficient for the prevention of SSOs, namely SSI, in the setting of laparotomy for emergent cases. The benefits of these devices do not seem to expand over the spectrum of wound complications although this was not one of our primary outcomes. No difference was observed in wound-related outcomes between both devices, therefore, both PICO™ and Prevena™ emmerge as valid options, with the consideration of acquisition cost being a crucial factor in decision-making process.
Acknowledgments
The authors express gratitude for the valuable the contribution of the entire Department of Surgery at Centro Hospitalar do Tâmega e Sousa. The unwavering dedication and enthusiasm of the team in patient enrollment significantly contributed to the success of our study.
Conflict of interest
No conflict of interest to declare.
Funding
We disclose that this study was made without support (equipment or grants) or funding from any institution being the costs fully supported by the authors.
Ethical consideration
The study was approved by the local ethics committee in Centro Hospitalar do Tâmega e Sousa, complying with the Helsinki declaration. Patients were enrolled in study after signature of informed consent.
REFERENCES
1. Societies WUoWH. Closed surgical incision management: Understanding the role of NPWT: Wounds International, 2016.
2. Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. 2017;96(1):1-15.
3. Ban KA, Minei JP, Laronga C, Harbrecht BG, Jensen EH, Fry DE, et al. American College of Surgeons and Surgical Infection Society: Surgical Site Infection Guidelines, 2016 Update. J Am Coll Surg. 2017;224(1):59-74.
4. Tolstrup MB, Watt SK, Gögenur I. Morbidity and mortality rates after emergency abdominal surgery: an analysis of 4346 patients scheduled for emergency laparotomy or laparoscopy. Langenbecks Arch Surg 2017; 402(4):615-623.
5. Boland PA, Kelly ME, Donlon NE, Bolger JC, Mehigan BJ, McCormick PH, et al. Prophylactic negative pressure wound therapy for closed laparotomy wounds: a systematic review and meta-analysis of randomised controlled trials. Ir J Med Sci 2021; 190(1):261-267.
6. Groenen H, Jalalzadeh H, Buis DR, Dreissen YEM, Goosen JHM, Griekspoor M, et al. Incisional negative pressure wound therapy for the prevention of surgical site infection: an up-to-date meta-analysis and trial sequential analysis. EClinicalMedicine 2023;62:102105.
7. (NICE) NIfHaCE. Prevena incision management system for closed surgical incisions, 2019.
8. (NICE) NIfHaCE. PICO negative pressure wound dressings for closed surgical incisions, 2019.
9. Scalise A, Calamita R, Tartaglione C, Pierangeli M, Bolletta E, Gioacchini M, et al. Improving wound healing and preventing surgical site complications of closed surgical incisions: a possible role of Incisional Negative Pressure Wound Therapy. A systematic review of the literature. Int Wound J 2016;13(6): 1260-1281.
10. Liu DS, Cheng C, Islam R, Tacey M, Sidhu A, Lam D, et al. Prophylactic Negative-pressure Dressings Reduce Wound Complications and Resource Burden After Emergency Laparotomies. J Surg Res 2021;257:22-31.
11. Cheong Chung JN, Ali O, Hawthornthwaite E, Watkinson T, Blyth U, McKigney N, et al. Closed incision negative pressure wound therapy is associated with reduced surgical site infection after emergency laparotomy: A propensity matched-cohort analysis. Surgery 2021; 170(5):1568-1573.
12. Frassini S, Cobianchi L, Fugazzola P, Biffl WL, Coccolini F, Damaskos D, et al. ECLAPTE: Effective Closure of LAParoTomy in Emergency-2023 World Society of Emergency Surgery guidelines for the closure of laparotomy in emergency settings. World J Emerg Surg 2023;18(1):42.
13. Kabir I, Nguyen T, Heaton J, Peterson K, Martyak M. Incisional Negative Pressure Wound Therapy to Decrease the Incidence of Surgical Site Infections in Trauma Laparotomy Wounds. Am Surg 2023;89(5):1908-1911.
14. Lakhani A, Jamel W, Riddiough GE, Cabalag CS, Stevens S, Liu DS. Prophylactic negative pressure wound dressings reduces wound complications following emergency laparotomies: A systematic review and meta-analysis. Surgery 2022;172(3):949-954.
15. Garg A, Jayant S, Gupta AK, Bansal LK, Wani A, Chaudhary P et al. Comparison of closed incision negative pressure wound therapy with conventional dressing for reducing wound complications in emergency laparotomy. Pol Przegl Chir 2021;93(5):1-5.
Full Text Sources:
Abstract:
Views: 7124

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.