Surgery, Gastroenterology and Oncology

|
|
Introduction: Pediatric sacrococcygeal teratoma (SCT), yet a rare tumor, is a common solid tumor among neonates. Although overall survival is excellent, tumor recurrence may compromise the outcomes.Objectives: The aim of this study is to determine overall survival rate, tumor recurrence rate, and associated factors for recurrence.
Materials and Methods: A retrospective chart review of patients admitted to Siriraj Hospital with SCT (2000-2018) was performed. Data were collected and analyzed for the association with outcomes, including survival rate, and tumor recurrence.
Results: Forty-one patients were included. Overall survival was 95.1%. Two patients died, one due to bleeding from perinatal tumors rupture and the other due to post-chemotherapy complications. Twenty-three patients who achieved at least 3-year period of follow-up. Among those, 2 patients developed recurrences which were significantly associated with late presentation, small tumor size, potentially malignant histology, and Altman type IV. Overall bowel or bladder dysfunctions were found in 8 patients.
Conclusion: Overall survival in SCTs was excellence. Recurrence occurred at 8.6%. However, it did not negatively influence the survival rate. Early diagnosis and complete tumor removal including the coccyx are crucial for minimizing tumor recurrence. Long-term follow-up and prompt intervention might improve outcomes of recurrent disease.
INTRODUCTION
Pediatric germ cell tumor is a rare tumor. However, sacrococcygeal teratoma (SCT) is one of common solid tumors among neonates. Histology of germ cell tumors varies from benign diseases (such as mature and immature teratoma) to malignant teratoma. The risk-based management protocol of SCTs has been created depends on histology of tumor, sites, and staging (1). According to current reports, overall survival of SCTs is excellent(2-4): 95-100% in immature teratoma, 95-100% in stage I-II malignant teratoma, and 75-90% in stage III-IV malignant teratoma (1).
Tumor recurrence leads the patient to unfavorable outcomes. Overall survival in recurrence cases is significantly decreases to 60% (2-4). Many factors contributing to recurrence were addressed in literatures, including delayed surgery, incomplete resection (2-5), preservation of coccyx (5), tumor spillage(5), and malignant histopathology (3, 4). However, there are still challenges to find other associated factors which finally lead to survival improvement.
Besides curing the diseases, another mandatory goal of SCT treatment is preserving bowel and bladder function. The dysfunctional problems included stress incontinence, enuresis, poor stream of urine, neurogenic bladder (6), involuntary bowel movement, soiling, and constipation (6,7). There are some risk factors which were reportedly associated with functional sequelae such as Altman’s classification, low gestational age (6), large tumor (7,8), and immature histology (8). However, there is still controversy regarding the significances of the associations of these factors to the functional outcomes among this group of patients.
The aims of this study were to address overall survival and recurrent rates among SCT patients in our center. Associated factors for recurrent disease were determined as well. Moreover, complications related with the treatment of SCTs were evaluated in this study.
MATERIALS AND METHODS
A retrospective chart review of patients who were admitted to Siriraj Hospital due to SCT between 2000 and 2018 was performed. Demographic data, clinical presentations and investigations, serum AFP, size, Altman type and histology of tumors, operative treatment, complications, survival, and recurrence of disease were collected.
Our institution adopted the management guideline proposed by Thai Pediatric Oncology Group (ThaiPOG) (9) which was developed based on Children’s Oncology Group (COG) recommendation. When a pre-sacral mass was suspected, complete physical examinations including digital rectal examination (DRE) were performed. Serum AFP, β-HCG and abdomino-perineal radiography were obtained as basic investigations. Further ultrasonography, CT scan or MRI were considered for determining extension of tumor and diagnosis confirming in uncertain cases. The majority of the patients, especially those who presented with protruded mass, had upfront surgery. Preoperative chemotherapy was reserved for patients with unresectable tumors with elevated serum AFP or distant metastasis. Surgical tumor resection en bloc with the coccyx was performed in all cases. Determining the deep edge of tumor by DRE and imaging provide beneficial information for surgical planning. Perineal incision was initiated first if the deep edge of tumor was palpable. Laparotomy assisted approach was required for deeper extension of tumor, especially in type III, IV. Tumor histology was evaluated by pathologists. Post-operative chemotherapy was required for all stages of malignant histology. However, children with immature teratoma either grade III or greater than stage II tumor may have received adjuvant chemotherapy upon the multidisciplinary team discretions as previously described (10). All patients were followed up by physical examination including DRE, serum AFP, and alternating US and CT imaging for at least 3 years (9). Interviewing regarding difficulty on urination and defecation were included.
Statistical analysis
All statistical analysis were performed using PASW statistics 18.0 (SPSS Inc., Chicago, IL, USA). Quantitative data were described as median and range while number and percentage were used for qualitative data. Chi-square test or Fisher’s exact test was used to compare the proportions between groups. Kaplan-Meier method was used to estimate 3-year recurrence free survival and log rank test was performed to compare 3-year recurrence free survival between groups. A p-value < 0.05 was considered statistically significant.
RESULTS
A total of 41 SCT patients were found in our institution during the study period. Fourteen (34%) were male and 27 (66%) were female. Currarino syndrome was found in 2 patients. Annular pancreas, asplenia, Shinzel-Giedion syndrome, congenital heart disease, liver hemangioma and renal failure were also found as comorbidities in 6 cases. Demographics and clinical presentations categorized by Altman’s classification and age onsets are demonstrated in table 1.
Table 1 - Demographic, clinical presentations categorized by age groups and Altman’s classification

Thirty-five children (85.3%) had their first symptom during neonatal period (< 30 days). Among neonates, mean gestational age was 37 weeks and median birth weight was 3.2 kg. Most common presenting symptom in neonatal period was protruded mass with or without rupture.
Six neonates experienced intrapartum tumor rupture. One neonate experienced sudden cardiac arrest soon after birth due to exsanguinous bleeding from tumor rupture. After resuscitation, emergency tumor removal and bleeding control was successfully performed via perineal incision. However, due to prematurity and massive blood transfusion, she passed away 2 days later. Other 5 intrapartum ruptures survived without any recurrence (fig. 1). All of them were prenatally diagnosed from other hospitals. Four cesarean sections were performed for huge SCTs (> 15 cm), while normal labor was identified in one case who had a 10-cm tumor.
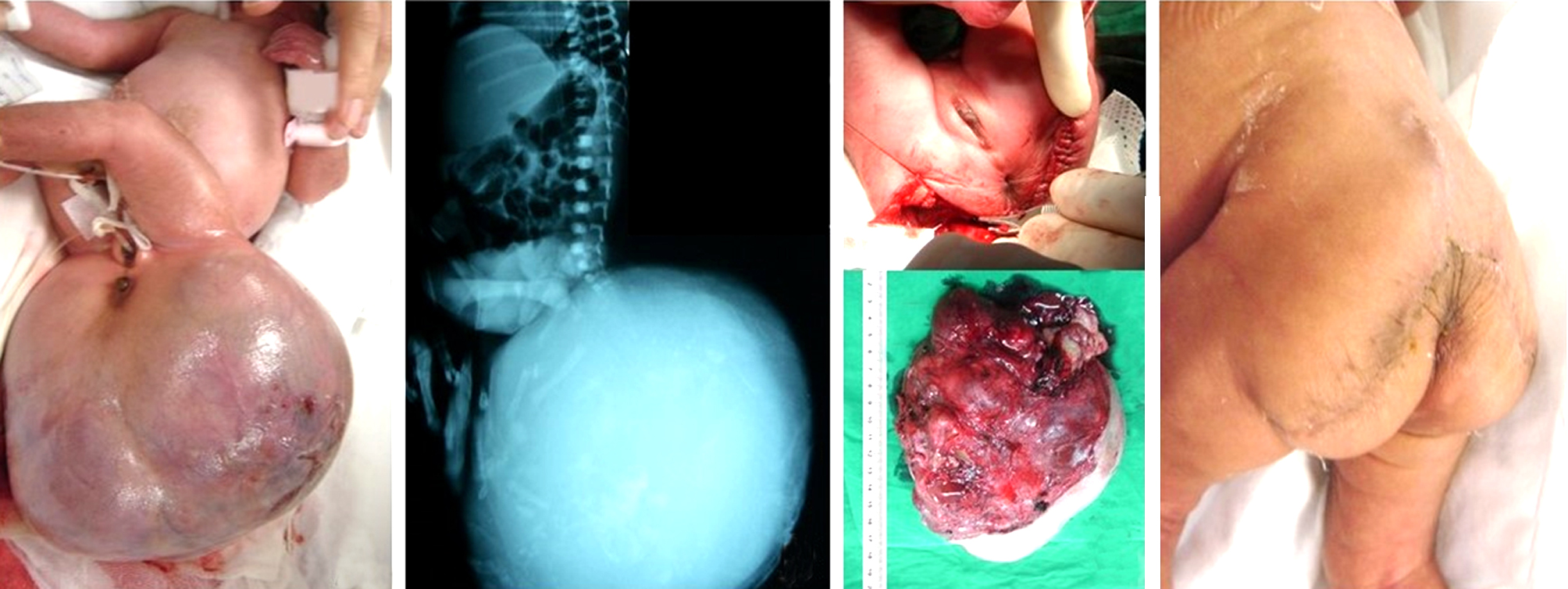
Figure1 - A 31-week GA, BW 2950 gm newborn presented with a huge sacrococcygeal teratoma with bleeding during intrapartum period (a). Plain film revealed soft tissue mass with multiple bony structures (b). After resuscitation, emergency en-bloc tumor resection with coccyx and concomitant anorectoplasty were performed. Tumor was 16 x 11 x 11 cm in size and 1050 gm in weight (c). Tumor histology was grade III immature teratoma. Healed surgical wound was achieved in two weeks after the operation (d). Now, she was 11-year-old and still visits our clinic for follow-up. There was no tumor recurrence occurs. She complained only occasional constipation which resolved by oral laxative drug
Six patients developed first symptom later than 30 days of life. Most common presenting symptom was genitourinary symptoms. There were rupture and bleeding of tumor found in 2 children due to direct trauma. Recurrence occurred in 2 cases in the late presentation group.
All patients underwent urgent tumor resection en bloc with the coccyx after diagnosis in our institute. However, there were 13 patients who had late surgery which occurred later than 30 days after presenting symptoms. Among these, there were 4 delayed diagnoses from other hospitals, 4 missed diagnoses as anterior meningocele, and 5 advanced disease requiring neo-adjuvant chemotherapy.
Intraoperative tumor spillage occurred in 4 patients (9.7%). Tumor maximal diameter ranged from 3.4-30 cm (median 10.0 cm). Neonatal group had bigger tumor size than late SCTs (Median 10.0 cm vs. 4.5 cm). Definite histopathology of tumors revealed that 20 patients (48.7%) had mature teratomas, 13 (31.7%) had immature teratomas, and 8 (19.5%) had malignant teratomas with malignant yolk sac elements. Sixteen incomplete resection of benign pathology was reported. Details of initial surgery and histology are demonstrated in table 2.
Table 2 - Surgical technique, tumor histopathology, outcomes and complications categorized by Altman’s classification

Overall survival rate was 95.1%. When categorized by the tumor histology, the overall survival was 100% in mature teratoma, 92.3% in immature teratoma, and 87.5% in malignant teratoma. There were 2 deaths in this study. One was due to febrile neutropenia and multiple comorbidities. The other one was due to massive blood loss from ruptured tumor during intrapartum period.
Twenty-one children had 3-year follow-up time without recurrence. Two recurrence were reported. Times to recurrence were 6.9 and 8.6 months. Rising of serum AFP during routine follow-up protocol was an initial abnormal finding for recurrence of disease. Case series of recurrent disease is showed in table 3. All of recurrence cases survived after re-excision and adjuvant chemotherapy.
Table 3 - Case series of tumor recurrence

The associated risk factors of recurrence of disease were late presentation (P= 0.005), tumor size less than 5 cm (P= 0.02), potentially malignant histology (P=0.045), and Altman type IV (P=0.02). While tumor spillage (P= 0.70) and incomplete resection margin (P=0.08) were not significant associated to recurrence disease.
Overall complications were demonstrated in table 2. Early complications were found in 9 cases. Wound infection with or without dehiscence occurred in 8 cases. These complications were improved after local wound care and intravenous antibiotics.
The overall long-term dysfunctional problems were reported in 8 children. All of GI problems were constipation. Occasional overflow incontinence requiring laxative and low rectal enema were also found. Among those who had GI problems, 2 also had neurogenic bladder which were diagnosed after the workup for urinary tract infection. There were 2 poor cosmetic outcomes requiring scar revision at 2 and 3 years after first operation.
DISCUSSION
SCTs is the most common solid tumor diagnosed in neonates. Recent articles state overall survival rate in range of 91.5-97.5% (2-4). Herein, we demonstrated outcomes of SCTs during the period of 18 years in a single tertiary care hospital in Thailand. The overall survival rate is high at 95.1% which in the range of case series worldwide (2-4). Two recurrences were identified. However, there was no mortality among recurrence group. Two deaths occurred due to massive bleeding from intrapartum tumor rupture and complication related to chemotherapy during treatment.
We divided SCTs into 2 groups according to age of presentation because of distinctive characteristics and outcomes in each group. More than 80% were neonates. All of neonates presented with protruded mass since birth with the median tumor size of 10.0 cm. A straightforward diagnosis could be made among them.
Tumor rupture can be a catastrophic complication during intrapartum period especially in huge mass (3). Antenatal ultrasonography plays an important role for planning route, time and place of delivery to avoid intrapartum injury (11). Cesarean section has been advocated in fetus with large tumor (> 5-10 cm) (11-13). Tumor size among neonates in our series were quite large. More than 80% of newborn had tumor greater than 5 cm. While cesarean section was performed in only 60% of cases. The low rate of cesarean section might relate to low incidence of prenatal diagnosis. Scheduled delivery procedure in tertiary-level hospital might relate with survival (11). Moreover, careful and gentle manipulation of the tumor is a key step to avoid tumor rupture, especially in huge tumors.
Tumor recurrence reportedly leads the patient to unfavorable outcomes (2-4). The incidence of recurrent tumor varies from 5 to 20% (2-5,14,15). In this study, three-year disease-free survival rate is 91.3% (100 % in mature and immature teratoma, and 66.7% in malignant disease). Contrary to other series (2-5), both of recurrence cases survived after surgical re-excision and chemotherapy.
Many factors contributing to recurrence were addressed in literatures. Altman’s type IV, small tumor size, malignant-potential histology, and late presentation were found as significant associated factors of recurrence.
Altman and colleagues (16) proposed a classification system of SCTs since 1973. Neonates and young infants who had tumors protrude externally predominant had low rate of malignancy histology. Older children who had pelvic or abdominal predominant tumor related with a higher rate of malignancy. Our results concur with the literature, the most common type in neonate SCTs was type I and II. Concealed presacral tumor, type IV, was not found in neonatal subgroup, and were commonly seen in late SCTs with compressive symptoms to bowel and bladder. In this study, type IV disease also related with the highest rate of malignant histology (25%) and microscopically incomplete resection (75%). Due to all of these reasons, 50% of type IV developed recurrences.
Patients with late presentation had poor outcomes, 1 death and 2 recurrences. Most children with late presentation were Altman’s type 4, small tumor size (< 5 cm), which concealed in the presacral area, and had atypical presentations, i.e. constipation and urinary symptoms. All of these characteristics result in high incidence of malignant histology, advanced disease requiring neoadjuvant chemotherapy in the first presentation and high incidence of recurrence compared to those in the neonatal age group. Understanding manifestations of SCTs in each age group leads to early diagnosis which may contribute to outcome improvement. We advocate careful physical examination including DRE in all children who present with bowel and bladder symptoms.
Timing from first presentation to definite surgery may influence malignant transformation (17) which related to recurrences. Delayed definite surgery was identified in 13 patients. Late presentation and delayed diagnosis from other hospital were previously described. Moreover, we found 4 cases who were initially diagnosed with meningoceles which received delayed treatment due to waiting for MRI at the age of one year. Bulging of anterior fontanelle when gently compression of presacral mass is an important sign of meningocele. We advocate careful physical examination and ultrasonography of abdomen, pelvis and spine as initial approach for all pre-sacral mass. If meningocele cannot be excluded, urgent MRI should be considered (17). However, recurrence was not found in missed diagnosis group.
All of patients in our institution underwent gross complete resection and coccygectomy. Almost 70% of operations were performed via perineal incision only. Among these, inverted-V shaped incision was chosen for adequate surgical exposure and also for good cosmetic outcomes (fig. 1). Laparotomy assisted approach was required in type III and IV tumor. Among these, posterior sagittal approach with muscle stimulator was performed in 4 cases. The posterior sagittal incision provided familiar operative field, good exposure and satisfactory cosmetic outcome (18). However, our experiences are limited in only type IV cases.
Microscopic involvement of any tumor histology at resection margin was mentioned as a risk factor related to recurrence (2-5). There was no recurrence among patients with mature teratoma who had microscopic involvement. Above-mentioned standard follow-up program of SCTs was sufficient for benign teratomas. On the other hand, microscopic residual of malignant histology and immature teratoma required additional adjuvant chemotherapy even with histology of mature part at the surgical margin. However, due to incomplete data in pathological reports, we were unable to identify relationship between recurrences and positive resection margin in our series. In our recent practice, cautions should be taken on tumor involvement at resection margin of mature teratoma.
According to histology, grade III immature teratoma and malignant teratoma were included in potentially malignant histology group because high grade immature teratoma also required adjuvant chemotherapy. Potentially malignant histology also had significant relationship with recurrence. This association was also confirmed in other articles (3,4). However, the malignant recurrence could occur in previously diagnosed mature and immature teratomas as well (4,14). Long-term follow-up should be taken in all histology SCTs.
Time to recurrence influence an optimal timing for follow-up protocol. Both recurrences occur within the first year. The range of time to recurrence is 12-26 months (3,4,11). Rising of serum AFP during follow-up prompted the investigation for the recurrences (11,15). The follow-up protocol suggests monitoring patients using rectal examination, serum AFP, and imaging for at least for 3 years (1,11,15). However, Padilla et al reported recurrence occur in several years after surgery (5). In our practice, all patients were followed until adulthood.
Nine early complications were identified. Wound infection with or without dehiscence was common. In the past, Ruangtrakool et al (14) reported wound complication in our institution to be as high as 34.3%. The improvement in surgical technique, antibiotics, wound care techniques may influence better wound outcomes.
Long-term dysfunctional problems influence quality of life. A Swedish multicenter study reported the incidence of bowel dysfunction and urinary tract dysfunction among SCTs as high as 36% and 46%, respectively (6). In this study, twenty-one children had 3-year follow-up time. Among these, eight children (38%) experienced dysfunctional problems, which still in range among other reports (6,7). Common dysfunctional problem was constipation which could be managed using occasional laxative and low rectal enema. Two neurogenic bladders were addressed. Both of them developed urinary tract infection during the follow-up. Postoperative urinary tract infection should prompt the work up for urinary tract dysfunction. However, the risk factor associated with long term complication could not be demonstrated in this study due to relatively small number of patients. Formal follow-up protocol focusing on bowel and urinary tract dysfunction may enhance the accuracy of functional outcomes among SCT patients. Prospective long-term study should be encouraged to find certain incidence of dysfunction outcomes and associated risk factors.
Limitations of this retrospective review were small sample size during long period of time and lack of complete information. Prospective multi-centered study was encouraged, especially to examine long-term bowel/bladder dysfunctions.
CONCLUSION
Overall survival in SCTs was excellence. Recurrence disease occurred in 8.6%. However, it did not negatively influence the survival rate. Early diagnosis and complete tumor removal including the coccyx are crucial for minimizing tumor recurrence. Long-term follow-up and prompt intervention might improve outcomes of recurrence disease.
Conflicts of interest
All authors declare no conflicts of interest.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki, and was approved by the Human research protection unit, Faculty of Medicine Siriraj Hospital, Mahidol University (#169/2562).
REFERENCE
1.Rescorla FJ. Chapter 37 - Teratomas and Other Germ Cell Tumors. In: Coran AG, editor. Pediatric Surgery (Seventh Edition). Philadelphia: Mosby; 2012. p. 507-16.
2.De Backer A, Madern GC, Hakvoort-Cammel FG, Haentjens P, Oosterhuis JW, Hazebroek FW. Study of the factors associated with recurrence in children with sacrococcygeal teratoma. J Pediatr Surg. 2006;41(1):173-81; discussion -81.
3.Derikx JP, De Backer A, van de Schoot L, Aronson DC, de Langen ZJ, van den Hoonaard TL, et al. Factors associated with recurrence and metastasis in sacrococcygeal teratoma. Br J Surg. 2006;93(12): 1543-8.
4.Wang Y, Wu Y, Wang L, Yuan X, Jiang M, Li Y. Analysis of Recurrent Sacrococcygeal Teratoma in Children: Clinical Features, Relapse Risks, and Anorectal Functional Sequelae. Med Sci Monit. 2017; 23:17-23.
5.Padilla BE, Vu L, Lee H, MacKenzie T, Bratton B, O'Day M, et al. Sacrococcygeal teratoma: late recurrence warrants long-term surveillance. Pediatr Surg Int. 2017;33(11):1189-94.
6.Hambraeus M, Al-Mashhadi A, Wester T, Svensson P-J, Stenström P, Lilja HE. Functional outcome and health-related quality of life in patients with sacrococcygeal teratoma – a Swedish multicenter study. Journal of Pediatric Surgery. 2019;54(8):1638-43.
7.Kremer ME, Derikx JP, van Baren R, Heij HA, Wijnen MH, Wijnen RM, et al. Patient-Reported Defecation and Micturition Problems Among Adults Treated for Sacrococcygeal Teratoma During Childhood--The Need for New Surveillance Strategies. Pediatr Blood Cancer. 2016;63(4):690-4.
8.Hambraeus M, Hagander L, Stenstrom P, Arnbjornsson E, Borjesson A. Long-Term Outcome of Sacrococcygeal Teratoma: A Controlled Cohort Study of Urinary Tract and Bowel Dysfunction and Predictors of Poor Outcome. J Pediatr. 2018;198:131-6 e2.
9.The Thai Pediatric Oncology Group. Treatment protocol for extra-cranial germ cell tumors National protocol for the treatment of childhood cancers 2018;1:338-343
10. Laohverapanich K BJ, Vathana N, Sanpakit K, Takpradit C, Narkbunnum N, Pongtanakul B, et al. Clinical Outcomes of Extracranial Germ Cell Tumors: A Single Institute’s Experience. Siriraj Med J [Internet]. 2021;73(10):680-6.
11. Fumino S, Tajiri T, Usui N, Tamura M, Sago H, Ono S, et al. Japanese clinical practice guidelines for sacrococcygeal teratoma, 2017. Pediatr Int. 2019;61(7):672-8.
12. Peiro JL, Sbragia L, Scorletti F, Lim FY, Shaaban A. Management of fetal teratomas. Pediatr Surg Int. 2016;32(7):635-47.
13. Kremer ME, Wellens LM, Derikx JP, van Baren R, Heij HA, Wijnen MH, et al. Hemorrhage is the most common cause of neonatal mortality in patients with sacrococcygeal teratoma. J Pediatr Surg. 2016;51(11):1826-9.
14. Ruangtrakool R, Nitipon A, Laohapensang M, Meekaewkunchorn D, Sangkhathat S, Sathornkich C, et al. Sacrococcygeal teratoma: 25 year experience. J Med Assoc Thai. 2001;84(2):265-73.
15. van Heurn LJ, Knipscheer MM, Derikx JPM, van Heurn LWE. Diagnostic accuracy of serum alpha-fetoprotein levels in diagnosing recurrent sacrococcygeal teratoma: A systematic review. J Pediatr Surg. 2020;55(9):1732-9.
16. Altman RP, Randolph JG, Lilly JR. Sacrococcygeal teratoma: American Academy of Pediatrics Surgical Section Survey-1973. J Pediatr Surg. 1974;9(3):389-98.
17. Jean-Martin Laberge PSPaKS. Teratomas, Dermoids and other soft tissue tumors. In: George W. Holcomb III JPM, Shawn D. St. Peter, editor. Holcomb and Ashcraft's Pediatric Surgery. Seventh ed: Elsevier Inc.; 2020. p. 1066-90.
18. Jan IA, Khan EA, Yasmeen N, Orakzai H, Saeed J. Posterior sagittal approach for resection of sacrococcygeal teratomas. Pediatr Surg Int. 2011;27(5):545-8.
Full Text Sources:
Abstract:
Views: 8390

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.