Surgery, Gastroenterology and Oncology

|
|
Background: Patients who are diagnosed with refractory chronic constipation that cannot be managed with maximal nonsurgical treatment may be considered for total colectomy with ileorectal anastomosis (TCIRA). However, the indications for determining a patient’s suitability for TCIRA remain unclear.
Methods: From December 2019 to September 2023, nineteen patients experiencing refractory chronic constipation who were selected for treatment with TCIRA according to our modified indications were retrospectively enrolled in this study. The medical records of and the original questionnaires administered to all patients were reviewed. The modified indications included a diagnosis of chronic constipation according to the Rome IV criteria; prior long-term management with maximal nonsurgical treatments, and a dilated, filled colon occupying the abdomen, resulting in frozen abdomen, as observed on computed tomography. We elected to perform TCIRA following the confirmation of frozen abdomen-induced organ disorders such as restrictive ventilatory defects, renal failure, and cardiac
disturbance or body weight loss (body mass index less than 16 kg/m2) due to severe appetite loss.
Results: According to the original questionnaires administered to all patients, eighteen (95%) patients were happy to have had undergone TCIRA, and 15 (79%) patients indicated improvements in their quality of life since the procedure. Medication use; stool frequency; stool form; bloating; abdominal pain; and appetite after the surgery were significantly improved compared with presurgical measurements. Eleven (58%) patients obtained body weight gain after the surgery.
Conclusions: Our results suggest that the modified indications for performing TCIRA are acceptable for selecting patients with refractory chronic constipation who require surgery.
INTRODUCTION
Constipation is a common gastrointestinal condition that is easily treated in most cases; however, a small group of patients with severe constipation continue to experience substantial symptoms despite maximal nonsurgical treatment (1). Surgery can successfully alleviate the symptoms of constipation; among the available surgical options, total colectomy with ileorectal anastomosis (TCIRA) is the gold standard for patients with refractory chronic constipation (1-4) and is widely accepted for patients suffering from refractory chronic constipation worldwide. However, because refractory chronic constipation has a variety of manifestations, such as colonic inertia, the indications for determining whether these patients should undergo TCIRA remain unclear. Therefore, we have continued to perform TCIRA for patients with refractory chronic constipation according to our modified indications established in 2019. There are no reports on the long-term outcomes of patients suffering from refractory chronic constipation who have been managed with TCIRA in Japan. The current retrospective study aimed to elucidate the validity of the modified indications for performing TCIRA for patients with refractory chronic constipation at our institution.
METHODS
The Ethics Committee for Biomedical Research of the National Hospital Organization Nishisaitama-chuo National Hospital Review Board approved the study protocol (2024-27), and all patients or their family members provided written informed consent for the use of their data. From December 2019 to September 2023, nineteen patients with refractory chronic constipation who underwent TCIRA according to our modified indications and through our original surgical procedure (3,4) by a single surgeon, (H. K.) were retrospectively included in this study. The medical records of and the original questionnaires administered to all patients were reviewed. The questionnaires, distributed to the patients more than one year after TCIRA, consisted of the following items: satisfaction with the surgery; quality of life changes since the surgery; body weight gain after the surgery; medication use after the surgery; stool frequency changes after the surgery; stool form changes after the surgery; bloating changes after the surgery; abdominal pain changes after the surgery; and appetite changes after the surgery (supplementary material). To evaluate the impact of TCIRA on those nine factors, we used the original questionnaires instead of the 36-item short form of the Medical Outcome Study Questionnaire (SF-36), Constipation Scoring System (CSS), and Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QOL).
Indications for TCIRA
The indicators for TCIRA used in our institution include a diagnosis of chronic constipation according to the Rome IV criteria (5); previous management with long-term maximal nonsurgical treatments; and
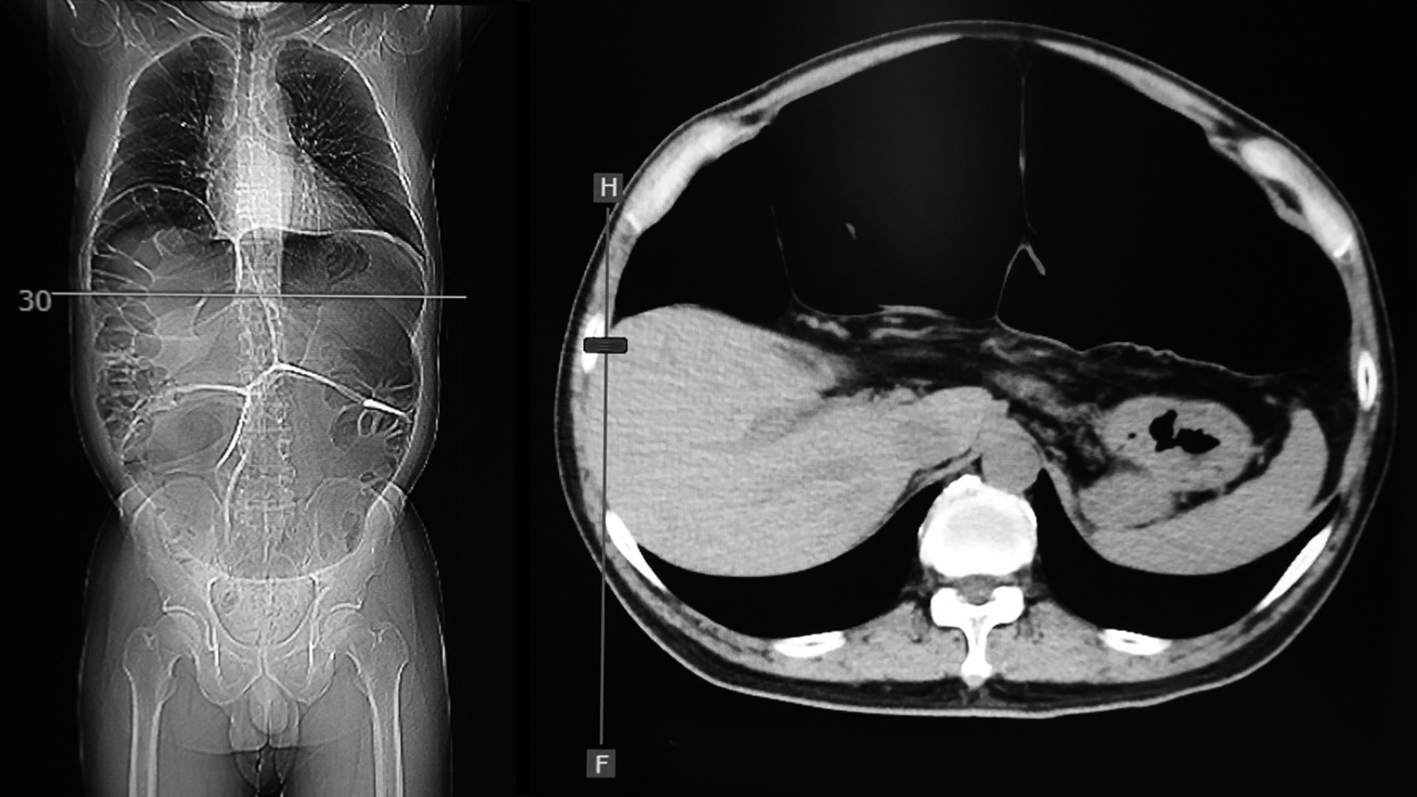
occupation of the abdominal cavity by a dilated, full colon in a manner similar to frozen abdomen, as confirmed by abdominal computed tomography (CT). Frozen abdomen is characterized by the persistent loss of natural free spaces between intraabdominal organs and compartmental structures such as the anterior abdominal wall, the retroperitoneal space, the pelvic cavity, and the diaphragm (fig. 1). We elected to perform TCIRA following confirmation of frozen abdomen-induced organ disorders, such as restrictive ventilatory defects (6), renal failure (7), and cardiac disturbance (8), or body weight loss (body mass index (BMI) less than 16 kg/m2) due to severe appetite loss (9). Patients who had gastric outlet obstruction and/or pelvic outlet obstruction were excluded.
Figure 1 - The abdominal CT is shown 'frozen abdomen'.
Statistical Analysis
Continuous variables are expressed as the means and ranges. The Wilcoxon rank-sum test was used to compare the continuous variables, and the c2 test was used to compare categorical data. A p value of less than 0.05 was used to indicate statistical significance. All the data were analyzed with the Statistical Package for Social Sciences (SPSS) 24.0 (IBM SPSS, Tokyo, Japan).
RESULTS
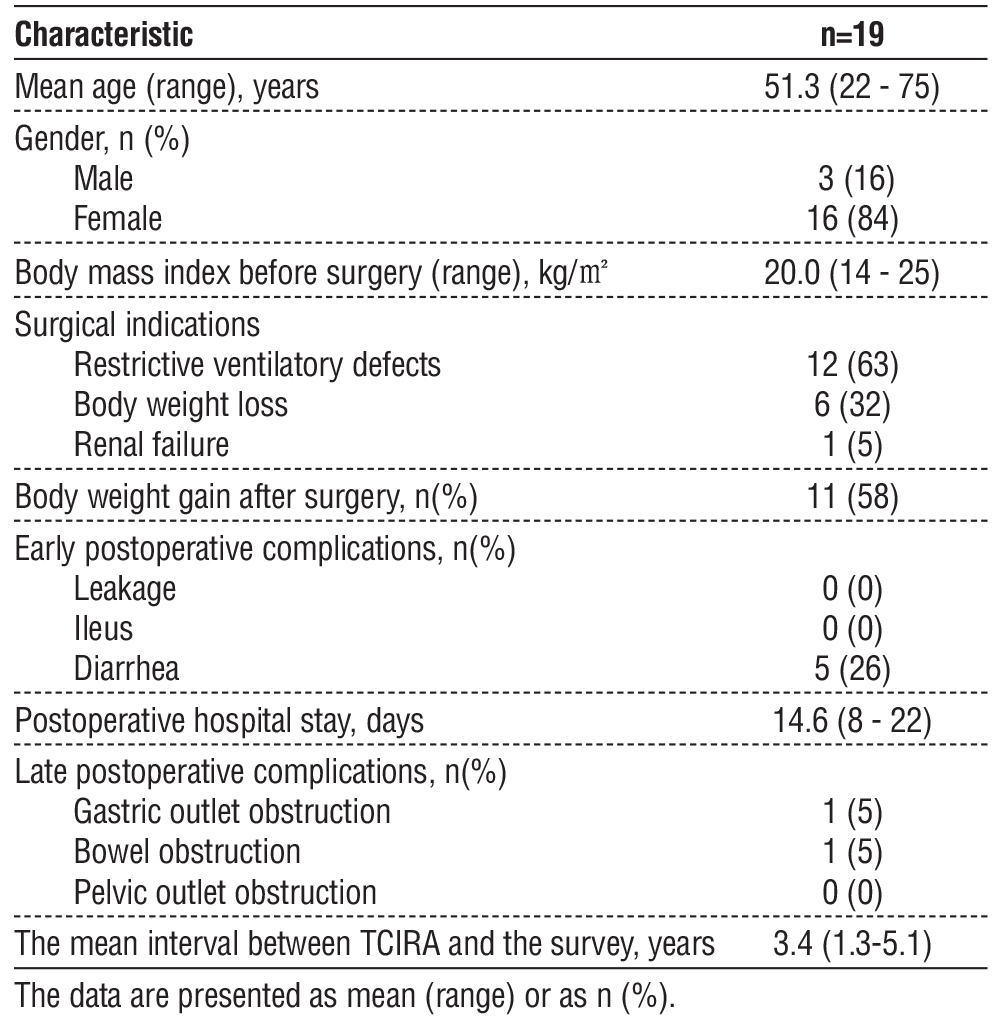
Clinical Patient Characteristics (table 1)
The mean age of the nineteen patients, including three males and sixteen females, was 51.3 (22-75) years, and the mean BMI was 20.0 (14-25) kg/m2. All patients who were referred from other institutions did not have gastric outlet obstruction and/or pelvic outlet obstruction. Regarding the surgical indications, twelve (63%) patients were due to restrictive ventilatory defects, six (32%) patients were due to body weight loss, and the remainder one (5%) patients underwent TCIRA due to renal failure. Eleven (58%) patients reported body weight gain after the surgery. With respect to early postoperative complications, five (26%) patients had severe diarrhea. Postoperative hospital stay was 14.6 (8-22) days. With respect to late post-operative complications, one patient who underwent gastrojejunostomy as the second surgery experienced gastric outlet obstruction, and one patient who
underwent adhesiotomy as the second surgery experienced bowel obstruction more than one year after surgery. The mean interval between TCIRA and the survey was 3.4 (1.35.1) years.
Table 1 - Clinical patient characteristics
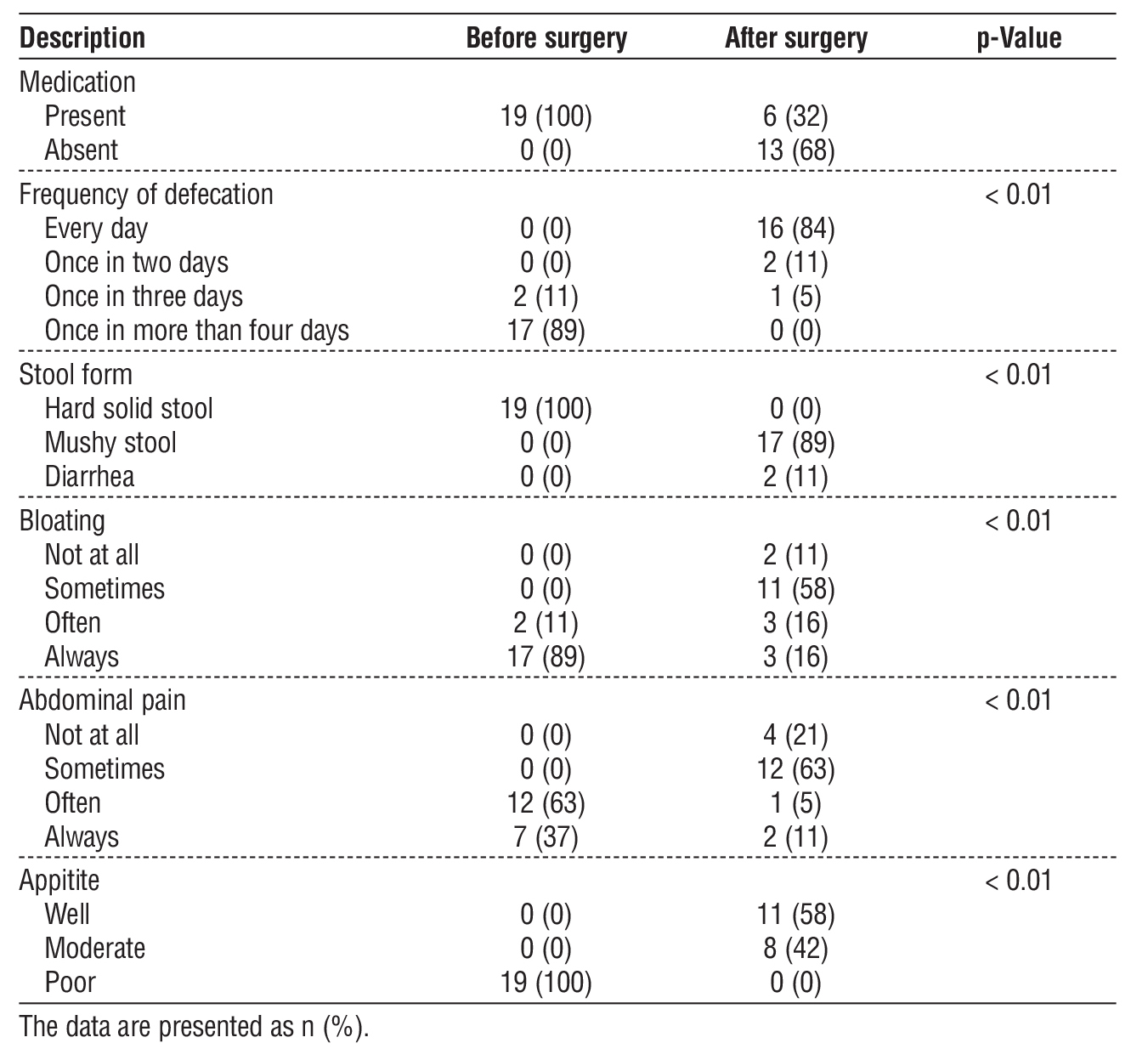
Comparison of Clinical Manifestations Between Before and After Surgery (table 2)
Six (32%) patients reported wanting to defecate every day and received linaclotide (10) after the surgery. However, these patients ultimately developed diarrhea within 3 hours after drug administration. Sixteen (84%) patients could defecate every day after the surgery, while no patients could defecate every day before the surgery. Seventeen (89%) patients could defecate mushy stool after the surgery, while all patients defecated hard solid stool before the surgery. Two (11%) patients felt no bloating after the surgery, whereas seventeen (89%) patients felt bloating before the surgery. However, seventeen (89%) patients continued experiencing bloating sometimes, often or always after the surgery. Four (21%) patients felt no abdominal pain after the surgery, whereas seven (37%) patients always felt abdominal pain before the surgery. However, fifteen (79%) patients continued experiencing abdominal pain sometimes, often or always after the surgery. Eleven (58%) patients increased in appetite after the surgery, whereas all patients associated with anorexia before the surgery. All nine of these factors after the surgery were significantly improved compared with presurgical measurements.
Table 2 - Comparison of clinical manifestations between before and after surgery
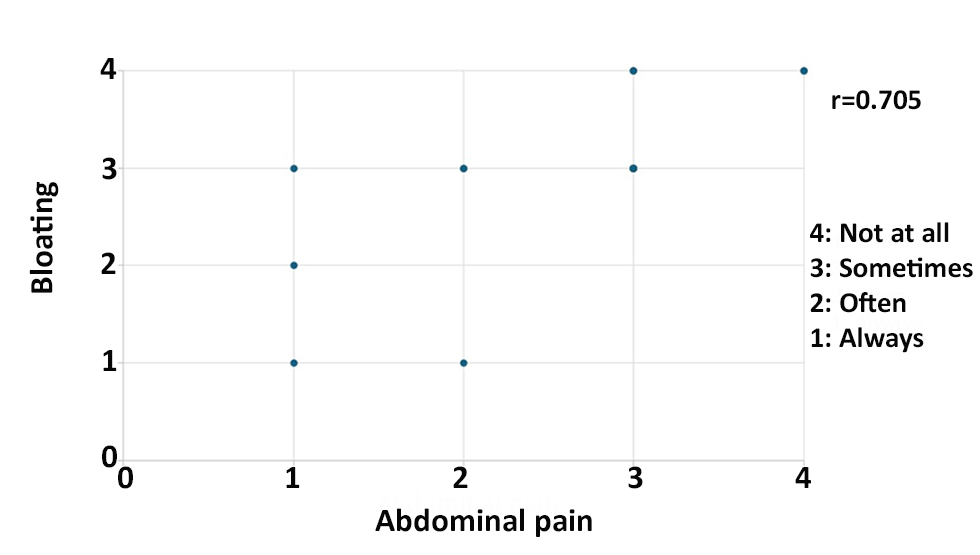
Correlation Between Bloating and Abdominal pain (fig. 2)
There was a strong correlation between bloating and abdominal pain (0.705).
Figure 2 - Correlation between bloating and abdominal pain. The correlation coefficient between the two factors was estimated 0.705.
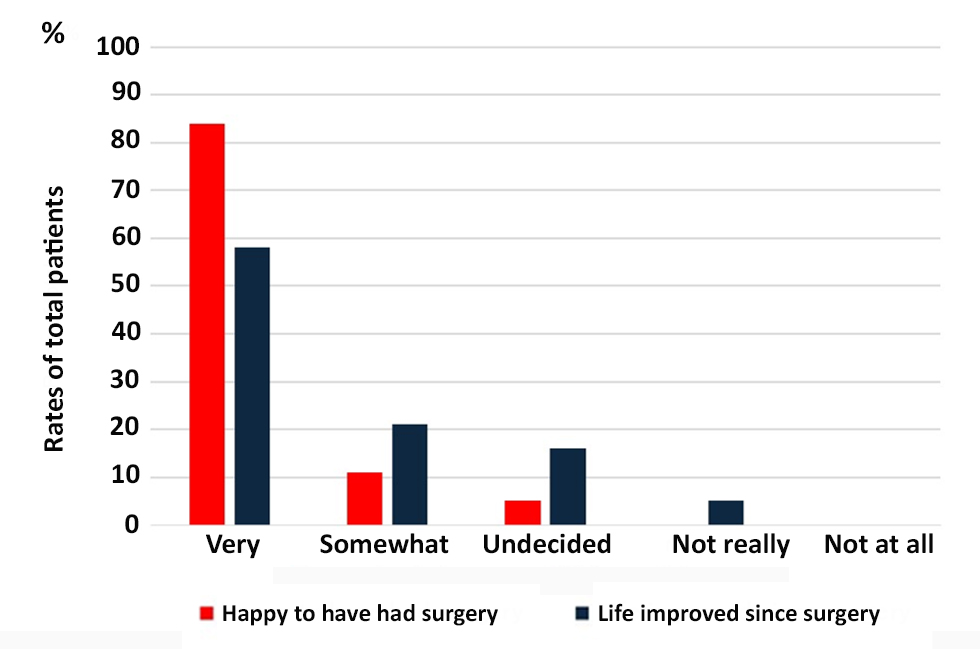
Satisfaction with TCIRA (fig. 3)
Sixteen patients felt very happy to have had surgery, and 2 patients felt somewhat happy to have had surgery. Therefore, 18 (95%) of nineteen patients felt at least somewhat happy to have had TCIRA. Eleven patients reported highly improved quality of life since the surgery, while 4 patients reported somewhat improved quality of life since the surgery. Therefore, 15 (79%) of all patients reported at least somewhat improved quality of life following TCIRA.
Figure 3 - Satisfaction with TCIRA. The bar graphs demonstrate the rates of all patients with happy to have had surgery or life improved since surgery.
DISCUSSION
TCIRA is the most effective and widely used surgical procedure for patients with refractory chronic constipation who fail to respond to maximal non-surgical treatment (11-13). However, the indicators for performing TCIRA for patients with refractory chronic constipation remain unclear. Previously, stimulant laxatives were considered the most effective therapeutic substances for patients with chronic constipation. In Japan, six new therapeutic drugs, including lubiprostone (14), linaclotide (10), and elobixibat (15), have been released since 2012 for patients with chronic constipation. Since then, however, the treatment strategy for patients with chronic constipation has changed drastically. As patients with chronic constipation have typically been managed with long-term maximal nonsurgical treatments involving the use of new therapeutic drugs, their colons have remained full and dilated, occupying the abdominal cavity in a manner similar to frozen abdomen, as confirmed by abdominal CT. Consequently, in our institution, we have elected to perform TCIRA following confirmation of frozen abdomen-induced organ disorders, such as restrictive ventilatory defects, renal failure, and cardiac disturbance, or body weight loss (BMI less than 16 kg/m2) due to severe appetite loss. These criteria for performing TCIRA are easier to understand than conventional criteria.
In this study, 95% of the patients felt at least somewhat happy to have had TCIRA. In addition, 79% of the patients had experienced at least somewhat improved quality of life since TCIRA. The satisfaction rate of all patients who received TCIRA was extremely high, consistent with previous reports (16-20). Additionally, medication use; stool frequency; stool form; bloating; abdominal pain; and appetite significantly improved after the surgery. Eleven (58%) patients reported body weight gain after the surgery. However, 89% of the patients reported experiencing at least some bloating after surgery, while 79% of the patients reported experiencing at least some abdominal pain postoperatively. Neither of these symptoms disrupted the patients’ daily activities. Previously published studies have reported that symptoms of bloating and abdominal pain frequently persist following surgery (21,22). The high satisfaction rates may be due to the relief that the patients experienced from their long-term refractory chronic constipation following TCIRA.
On the other hand, there was a strong relationship between bloating and abdominal pain after the surgery according to the questionnaire responses, with a correlation coefficient of 0.705. Patients with refractory chronic constipation tend not to consider bloating and abdominal pain to be different events. Abdominal pain may result from bloating, such as that which occurs in irritable bowel syndrome, and these events may not be improved by only surgical procedures such as TCIRA.
A recent review demonstrated that individual studies on the effectiveness of TCIRA may yield varying results; however, the satisfaction rates of patients who received TCIRA were extremely high despite differences in functional outcomes, including frequent continuation of pain and bloating symptoms and the possibility of very poor functional outcomes (16-20).
Conclusion
Despite potential limitations, our experience suggests that our original indications for performing TCIRA are acceptable for selecting patients with refractory STC who require surgery.
Authors’ Contributions
Study conception and design: H.K; Acquisition of data: H.K; Analysis and interpretation of data: H.K,
N.O; Drafting of manuscript: H.K; Critical revision of manuscript: H.K, N.O. Final approval of the version to be published: H.K, N.O.
Conflict of Interest
The authors declare no financial conflict of interest.
Ethics Approval
The Ethics Committee for Biomedical Research of the National Hospital Organization Nishisaitama-chuo National Hospital Review Board approved the protocol (2024-27).
Informed Consent
All participants provided informed consent prior to their participation.
REFERENCES
1. Johnston BJ, Clark DA, Warwick AM. Long-term outcomes of total colectomy for severe constipation. Colorectal Dis. 2023;25(6):1194-201.
2. Corsetti M, Brown S, Chiarioni G, Dimidi E, Dudding T, Emmanuel A, et al. Chronic constipation in adults: contemporary perspectives and clinical challenges. 2: conservative, behavioural, medical and
surgical treatment. Neurogastroenterol Motil. 2021;33(7):e14070.
3. Kawahara H, Watanabe K, Tomoda M, Enomoto H, Akiba T, Yanaga K. Single-incision clipless laparoscopic total colectomy. Hepatogastroenterol. 2014;61(130):453-5.
4. Kawahara H, Omura N. Single-incision clipless laparoscopic total colectomy for intractable slow transit constipation: a single surgeon's experience. Langenbecks Arch Surg. 2022;407(6):2585-93.
5. Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, et al. Bowel disorders. Gastroenterology. 2016;S0016-5085(16)00222-5.
6. Milanese A, Schechter NL, Ganeshananthan M. Constipation presenting as respiratory distress. J Adolesc Health Care. 1986;7(4): 255-8.
7. Sumida K, Molnar MZ, Potukuchi PK, Thomas F, Lu JL, Matsushita K, et al. Constipation and Incident CKD. J Am Soc Nephrol. 2017;28(4):1248-58.
8. Maruyama T, Hieda M, Eiraku K, Uozumi Y, Nomura H. Constipation and heart failure: An overlooked but important linkage. Geriatr Gerontol Int. 2023;23(3):255-6.
9. Alame AM, Bahna H. Evaluation of constipation. Clin Colon Rectal Surg. 2012;25(1):5-11.
10. Castro J, Harrington AM, Hughes PA, Martin CM, Ge P, Shea CM, Jin H, Jacobson S, et al. Linaclotide inhibits colonic nociceptors and relieves abdominal pain via guanylate cyclase-C and extracellular cyclic guanosine 3',5'-monophosphate. Gastroenterology. 2013; 145(6):1334-46.e1-11.
11. Ho YH, Tan M, Eu KW, Leong A, Choen FS. Laparoscopic-assisted compared with open total colectomy in treating slow transit constipation. Aust N Z J Surg. 1997;67(8):562-5.
12. Nyam DC, Pemberton JH, Ilstrup DM, Rath DM. Long-term results of surgery for chronic constipation. Dis Colon Rectum. 1997;40(3): 273-9.
13. Bernini A, Madoff RD, Lowry AC, Spencer MP, Gemlo BT, Jensen LL, et al. Should patients with combined colonic inertia and nonrelaxing pelvic floor undergo subtotal colectomy? Dis Colon Rectum. 1998; 41(11):1363-6.
14. Johanson JF, Morton D, Geenen J, Ueno R. Multicenter, 4-week, double-blind, randomized, placebo-controlled trial of lubiprostone, a locally-acting type-2 chloride channel activator, in patients with chronic constipation. Am J Gastroenterol. 2008; 103(1):170-7.
15. Nakajima A, Seki M, Taniguchi S, Ohta A, Gillberg PG, Mattsson JP, et al. Safety and efficacy of elobixibat for chronic constipation: results from a randomised, double-blind, placebo-controlled,
phase 3 trial and an open-label, single-arm, phase 3 trial. Lancet Gastroenterol Hepatol. 2018;3(8):537-47.
16. Knowles CH, Grossi U, Horrocks EJ, Pares D, Vollebregt PF, Chapman M, et al. Surgery for constipation: systematic review and practice recommendations: graded practice and future research
recommendations. Colorectal Dis. 2017;19 Suppl 3:101-13.
17. Xie X-Y, Sun K-L, Chen W-H, Zhou Y, Chen B-X, Ding Z, et al. Surgical outcomes of subtotal colectomy with antiperistaltic caecorectal anastomosis vs total colectomy with ileorectal
anastomosis for intractable slow-transit constipation. Gastroenterol Rep. 2019;7(6):449-54.
18. Baelum JK, Qvist N, Ellebaek MB. Ileorectal anastomosis in patients with Crohn's disease. Postoperative complications and functional outcome - a systematic review. Colorectal Dis. 2021; 23(10):2501-14.
19. Chaichanavichkij P, Vollebregt PF, Tee SZY, Scott SM, Knowles CH. Slow-transit constipation and criteria for colectomy: a crosssectional study of 1568 patients. BJS Open. 2021;5(3):zrab049.
20. Scott SM, Simrén M, Farmer AD, Dinning PG, Carrington EV, Benninga MA, et al. Chronic constipation in adults: contemporary perspectives and clinical challenges. 1: epidemiology, diagnosis, clinical associations, pathophysiology and investigation. Neuro-gastroenterol Motil. 2021;33(6): e14050.
21. Corsetti M, Brown S, Chiarioni G, Dimidi E, Dudding T, Emmanuel A, et al. Chronic constipation in adults: contemporary perspectives and clinical challenges. 2: conservative, behavioural, medical and surgical treatment. Neurogastroenterol Motil. 2021; 33(7):e14070.
22. Knowles CH, Grossi U, Chapman M, Mason J. Surgery for constipation: systematic review and practice recommendations: results I: colonic resection. Colorectal Dis. 2017 Sep:19 Suppl 3:17-36.
Full Text Sources:
Abstract:
Views: 2592

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.