Surgery, Gastroenterology and Oncology

|
|
Background: De novo tumors after liver transplantation are recognized as a major cause of long-term mortalities. Ampulla of Vater tumor is a relatively uncommon tumor among all periampullary tumors. In the current report, we describe a rare case of successful resection of De Novo tumor of the ampulla of Vater nine years after living-donor liver transplantation (LDLT).
Case report: 57 years male patient underwent LDLT utilizing right hemi-liver graft nine years ago for hepatitis C virus related liver cirrhosis. He developed recent onset diabetes mellitus and abnormal elevation of serum liver functions. After detailed work up, endoscopic retrograde cholangio-pancreatography (ERCP) was performed and showed an ampullary mass that was biopsied. Endoscopic biopsy result was poorly differentiated adenocarcinoma of the Ampulla of Vater. The patient was discussed in multi-disciplinary meeting and the decision was to proceed for exploration for potential resection. Pancreaticoduodenectomy (PD) was performed with adequate lymph nodes dissection. Reconstruction was performed by pancreatico-gastrostmy over an internal stent, retrocolic choledocho-jejunostomy, and antecolic gastro-jejunostomy. The patient developed grade B postoperative pancreatic fistula that required ultrasound guided tube drainage for abdominal collection. The patient was discharged from hospital for regular follow up.
Conclusion: Liver transplant recipients are at high risk for the development of De novo tumors. Here, we presented a rare case of successful PD for De novo adenocarcinoma of the Ampulla of Vater nine years after LDLT. The current case supports the feasibility and eligibility of performing such major pancreatic resection among recipients after LDLT.
Introduction
De novo tumors after liver transplantation have been well recognized as a major cause of long-term mortalities following cardiovascular complications (1,2). The incidence of de novo tumors after liver transplantation has been hetero-genous among different studies. This is related to several factors including patient demographics, the underlying aetiology of liver transplantation, the immunosuppression protocol utilized, and the duration of follow up after liver transplantation (3,4). We previously reported that the incidence of de novo tumors among Egyptian patients after living-donor liver transplantation (LDLT) was 2.3% after a mean follow-up period of 41.2 ± 25.8 months, in area where hepatitis C viral infection (genotype 4) is the main underlying cause of liver cirrhosis (5).
Previous studies had identified a wide variety of de novo malignancies after solid organ transplantation. The most reported de novo malignancies after liver transplantation include post-transplantation lymphoproliferative disorders (PTLDs), and cutaneous cancers. Other malignancies were also reported including head and neck tumors, gynecological malignancies, Kaposi sarcoma, genitourinary tumors, and gastrointestinal tumors (6-8).
Periampullary neoplasms are recognized among the most lethal tumors worldwide. They represent the seventh leading cause of cancer-related mortality worldwide with mortality rate of almost 7.7 per 100,000 population in European countries and almost 7.6 per 100,000 population in North American countries (9,10). Ampulla of Vater tumor is a relatively uncommon tumor, accounting for almost 6% of all periampullary tumors (11). In most series, a high resectability rate has been reported, and the prognosis is more favorable than with other malignant tumors of the periampullary region after curative resection (11,12).
Pancreaticoduodenectomy (PD) for De novo periampullary tumors following living-donor liver transplantation had been addressed in few previous reports (13,14). To the best of our knowledge, PD for De novo tumors of ampulla of Vater after LDLT had been rarely reported (15).
In the current report, we describe a rare case of successful PD for De Novo tumor of ampulla of Vater nine years after LDLT. This work has been reported in line with the SCARE criteria (16).
Case Presentation
57 years male patient underwent LDLT utilizing right hemi-liver graft nine years ago for hepatitis C virus related liver cirrhosis. The actual graft weight was 1100 g and graft weight to recipient weight ratio (GRWR) was 1.33. The surgical technique regarding LDLT had been described previously (17). He had smooth postoperative course and was under routine follow up in outpatient clinic. He was maintained on a single agent immunosuppressive regimen (Tacrolimus). He developed recent onset diabetes mellitus (two months ago) that was controlled with regular insulin therapy.
The patient showed abnormal elevation of serum liver functions on follow up visit in the form of elevated serum total bilirubin 3.3 mg/dl, serum direct bilirubin 3 mg/dl, serum alkaline phosphatase 22 KAU, serum gamma glutamyl transferase 228, serum alanine aminotransferase 70 IU/ml and serum aspartate aminotransferase 92 IU/ml. Abdominal ultrasound showed healthy liver graft with mild dilatation of intrahepatic biliary radicals (IHBRs) and dilated common bile duct (CBD) up to 12 mm. Magnetic resonance cholangio-pancreatography (MRCP) was ordered and showed dilatation of IHBRs, CBD (16 mm) down to a periampullary mass (fig. 1 a). Endoscopic retrograde cholangio-pancreatography (ERCP) was performed and showed an ampullary mass that was biopsied, and a stent was placed inside the CBD (fig. 1 b,c). Endoscopic biopsy result was poorly differentiated adenocarcinoma of the Ampulla of Vater.
Figure 1 - (a) Preoperative magnetic resonance cholangio-pancreatography showing dilatation dilated intrahepatic biliary radicles and common bile duct down to a distal stricture. (b) - Endoscopic view during endoscopic retrograde cholangio-pancreatography showing a friable ampullary mass. (c) - Endoscopic retrograde cholangiography dilated intrahepatic biliary radicles and common bile duct down to a distal stricture.

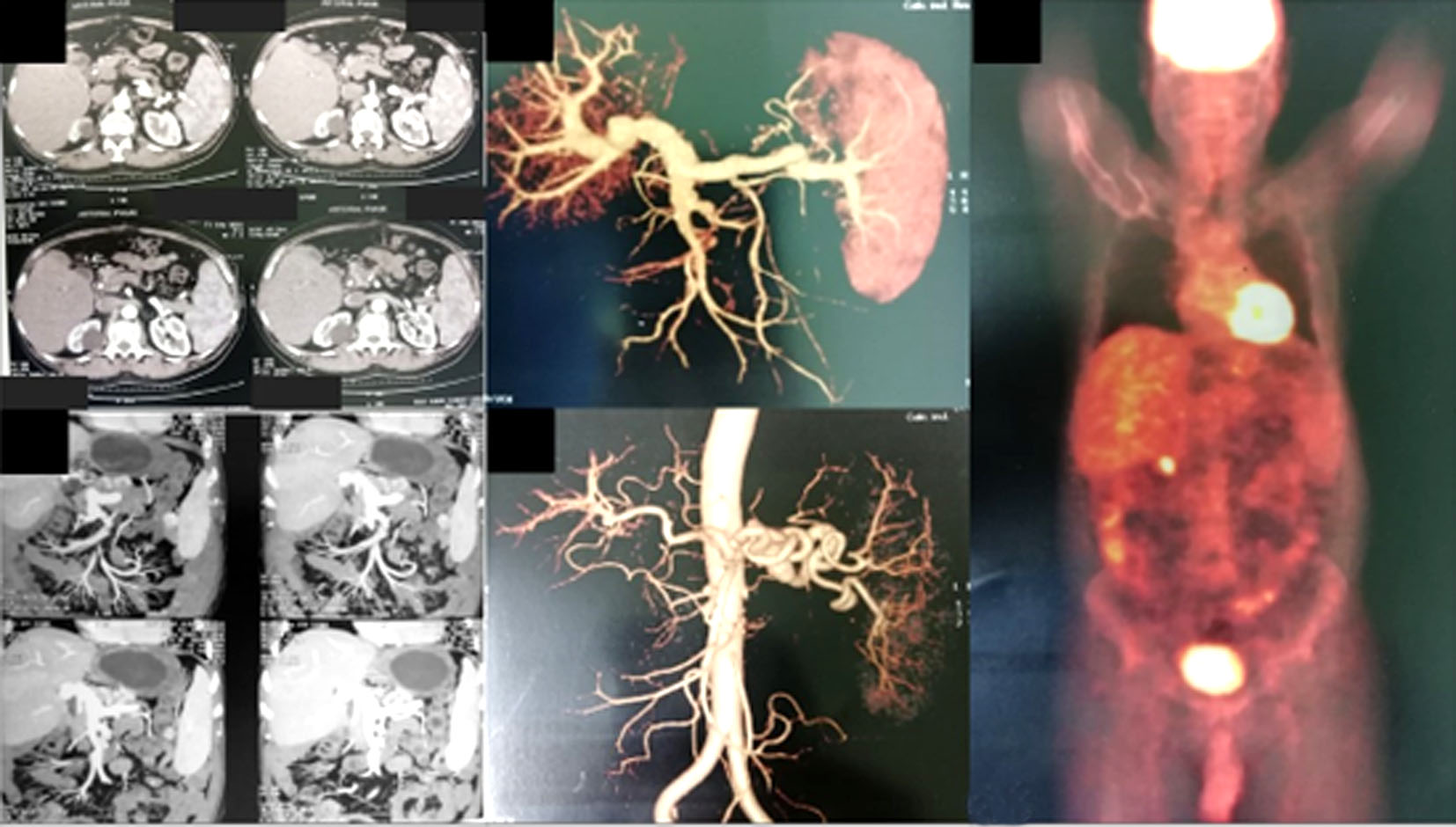
Abdominal computed tomography (CT) was ordered average sized liver graft with uniform parenchyma with no focal lesions of abnormal enhancement. Mild enlarged spleen with normal density and enhancement. The biliary tree showed mild dilatation of IHBRs, dilated CBD up to 16 mm with stent inside down to ampullary mass measuring 2 × 2.2 cm without any vascular invasion (fig. 2 a,b). CT portography showed a normal course and contrast filling of the main portal vein with mild decrease caliber at the anastomotic site without stenosis (fig. 2 c). CT angiography showed normal course and contrast filling of hepatic arteries till the liver graft (fig. 2 d).
Positron emission tomography (PET-CT) study was ordered to rule out the presence of metastatic deposits. PET-CT showed glucose avid periampullary mass 2.4 × 2.8 cm with SUVmax of 32 (active tumor biology) without any nearby organ invasion. Few enlarged para-duodenal lymph nodes up to 1 cm in size eliciting increased tracer uptake with SUVmax of 5.5. No other metabolically active lesions were detected in the liver graft and other body organs (fig. 2 e).
Figure 2 - (a,b) - Abdominal computed tomography (CT) showing an ampullary mass 2 × 2.2 cm. (c) - Preoperative CT portography. (d) - Preoperative CT angiography. (e) - Preoperative positron emission tomography showing glucose avid periampullary mass without other metabolically active lesions.
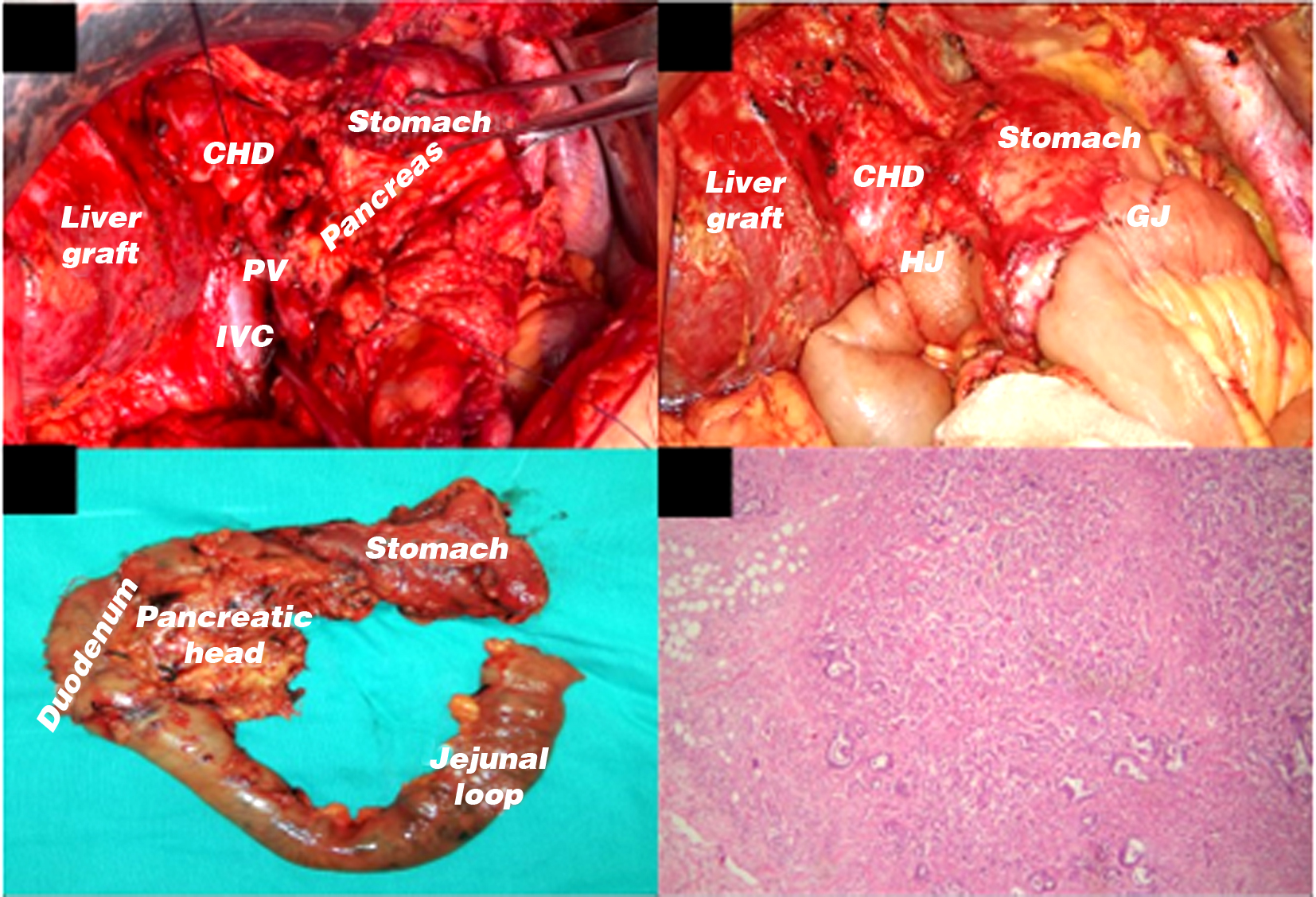
The patient condition was discussed in multidisciplinary meeting and the decision was to proceed for exploration for potential resection of the ampullary lesion. Surgical exploration was done which showed moderate perihepatic adhesions that were completely dissected. After Kocher maneuver of the duodenum, an ampullary lesion about 2 cm in size was identified with no local vascular invasion or distant abdominal metastasis. Pancreaticoduodenectomy was performed with adequate lymph nodes dissection (fig. 3 a). Reconstruction was performed by pancreatico-gastrostmy in two layers utilizing Vicryl 3/0 interrupted sutures over an internal stent. Choledocho-jejunostomy was performed in end-to-side fashion utilizing PDS 5/0 continuous sutures. We utilized the recipient remnant bile duct because of adequate bleeding from cut end of the bile duct denoting adequate vascularity. Finally, antecolic gastro-jejunostomy was performed in side-to-side fashion utilizing Vicryl 3/0 continuous sutures (fig. 3 b). Total operation time was 4 hours. Operative blood loss was about 600 cc and one unit of red blood cells was transfused to the patient. After surgery, the patient was transferred to the intensive care unit for monitoring of vital signs and abdominal drains. Afterwards, the patient was transferred for the ward for routine care till discharge. The patient developed grade B postoperative pancreatic fistula that required ultrasound guided tube drainage for abdominal collection. The patient was discharged from hospital for regular follow up. The patient was shifted from Tacrolimus monotherapy to Everolimus monotherapy afterwards. Postoperative pathological examination revealed a moderately differentiated ampullary adenocarcinoma infiltrating all the duodenal wall and encroaching pancreatic tissue (fig. 3 d). All surgical resection margins were free from tumor tissue. All dissected lymph nodes were free from tumor tissue. The tumor showed perivascular and perineural emboli.
Figure 3 - (a) - Operative field after completing pancreatico-duodenectomy. (b) - Operative photo after completing reconstruction. (c) - Gross picture of the surgical specimen after completing pancreatico-duodenectomy. (d) - Microscopic examination of the specimen showing a moderately differentiated ampullary adenocarcinoma (H&E X40) (CHD, common hepatic duct; PV, portal vein; IVC, inferior vena cava; HJ, hepatico-jejunostomy; GJ, gastro-jejunostomy).
Discussion
Adenocarcinoma of the Ampulla of Vater is the second most common periampullary neoplasm. It one of the uncommon tumors and accounts for almost 0.2% of all gastrointestinal tract tumors (11). In the setting of post-LDLT De novo tumors, Ampulla of Vater adenocarcinoma is very rarely reported (15). In the current report, we describe a rare case of De novo adeno-carcinoma of the Ampulla of Vater after LDLT that could be successfully managed with radical surgical excision.
Many challenges remain concerning the diagnosis and management of the Ampulla of Vater tumors. The diagnosis is mainly dependent on endoscopic biopsy. However, endoscopic biopsy fails to identify the presence of malignant tumor foci in about 12% to 40% of ampullary tumors. Also, the pathologic examination of the resected surgical specimens demonstrated concomitant adenomas in up to 80% of ampullary carcinomas (18,19). In the current case, our patient presented with laboratory abnormalities of early biliary obstruction allowing early endoscopic intervention by ERCP. Endoscopic biopsies confirmed the presence of adenocarcinoma of the Ampulla of Vater.
Major pancreatic resections for periampullary tumors after LDLT had been rarely reported in the literature (13-15). Major pancreatic operations, especially PD, after LDLT are always complex and technically demanding. This is attributed to the extensive postoperative surgical adhesions especially around the hepatoduodenal ligament. Also, the associated risks of accidental injuries to essential hepatic vascular structures like the portal vein and hepatic artery (15). In the current study, performing PD for De novo adenocarcinoma of the Ampulla of Vater after LDLT was challenging. The tissues around the area of the hepatoduodenal ligament, the pancreatic head, and the porto-mesentric junction were soft and friable compared to the routine PD patients owing to the impact of the immunosuppressive medications. Meticulous dissection was performed with acceptable blood loss during the dissection stage and the patient required transfusion of only one unit of red blood cells.
Another important point to be clarified is the biliary reconstruction in PD after LDLT with duct-to-duct anastomosis. In this situation, it is not safe to remove the whole recipient extrahepatic bile duct till the hepatic hilum. So, division of the distal part of the recipient common bile duct is performed away from the site of previous duct-to-duct anastomosis. The vascularity of this segment of recipient bile duct remains a matter of debate. This issue had been raised by Na et al. in a previous report from ASAN Medical Center, Korea. They worried about the blood supply of the interposed portion of recipient bile between the graft bile duct and jejunal bowel loop. They recommended checking of retrograde arterial blood flow of this interposed portion of the common bile duct from the graft side. If the retrograde arterial blood flow is adequate, thus choledocho-jejunostomy could be safely performed (15). In the current report, we performed the same procedure and checked the retrograde arterial bleeding from the divided recipient bile duct. The vascularity of the recipient bile duct was adequate and allowed choledocho-jejunostomy to be performed safely. The patient did not suffer from biliary leakage after the operation.
Finally, the association between the development of De novo tumors and recurrent rejection episodes after solid organ transplantation is well demonstrated in previous studies (20-22). The development of rejection episodes will require higher doses of immuno-suppression medications or addition of other anti-rejection therapies to transplant recipients. On the other hand, other studies did not find any significant difference in the incidence of De novo tumors among liver transplant recipients with and without rejection episodes (23). We previously reported the strong association of rejection episodes and the development of De novo tumors among liver transplant recipients (5). However, in the current study, the patient did not suffer from any clinically significant rejection episodes during the follow up period.
The patient was shifted from calcineurin inhibitor, as a primary immunosuppressant agent, to a mammalian target of rapamycin (mTOR) inhibitor owing to the expectation of anti-tumor effect of the mTOR inhibitor.
Conclusion
Liver transplant recipients are at high risk for the development of De novo tumors which are a leading cause of their long-term mortality. Here, we presented a rare case of successful PD for De novo adenocarcinoma of the Ampulla of Vater nine years after LDLT. The current case supports the feasibility and eligibility of performing such major pancreatic resection among recipients after LDLT.
Conflicts of interest / Competing interest
All authors declare no conflicts of interest.
Funding
No external funding resources for research.
Consent to participate
Written informed consent was obtained from the patient of this case report.
References
1. Watt KD, Pedersen RA, Kremers WK, Heimbach JK, Charlton MR. Evolution of causes and risk factors for mortality post-liver transplant: results of the NIDDK long-term follow-up study. Am J Transplant. 2010;10(6):1420-7.
2. Rossetto A, Tulissi P, De Marchi F, Gropuzzo M, Vallone C, Adani GL, et al. De novo solid tumors after kidney transplantation: is it time for a patient-tailored risk assessment? Experience from a single center. Transplant Proc. 2015;47(7):2116-20.
3. Chapman JR, Webster AC. Cancer after renal transplantation: the next challenge. Am J Transplant. 2004;4(6):841-2.
4. Buell JF, Gross TG, Woodle ES. Malignancy after transplantation. Transplantation. 2005;80(2 Suppl):S254-64.
5. Wahab MA, Abdel-Khalek EE, Elshoubary M, Yassen AM, Salah T, Sultan AM, et al. Predictive factors of DE Novo malignancies after living-donor liver transplantation: A single-center experience. Transplant Proc. 2021;53(2):636-644.
6. Liu ZN, Wang WT, Yan LN, Group LS. De novo malignancies after liver transplantation with 14 cases at a single center. Transplant Proc. 2015;47(8):2483-7.
7. Herrero JI. De novo malignancies following liver transplantation: impact and recommendations. Liver Transpl. 2009;15 Suppl 2: S90-4.
8. Herrero JI, Lorenzo M, Quiroga J, Sangro B, Pardo F, Rotellar F, et al. De novo neoplasia after liver transplantation: an analysis of risk factors and influence on survival. Liver Transpl. 2005;11(1):89-97.
9. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
10. Rawla P, Sunkara T, Gaduputi V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J Oncol. 2019; 10(1):10-27.
11. Giorgio AD, Alfieri S, Rotondi F, Prete F, Di Miceli D, Pericoli Ridolfini M, et al. Pancreatoduodenectomy for tumors of Vater’s ampulla: report on 94 consecutive patients. World J Surg. 2005; 29(4):513-8.
12. Bouvet M, Gamagami RA, Gilpin EA, Romeo O, Sasson A, Easter DW, et al. Factors influencing survival after resection for periampullary neoplasms. Am J Surg. 2000; 180(1):13-7.
13. Yoshizumi T, Shimada M, Soejima Y, Terashi T, Taketomi A, Maehara Y. Successful pylorus-preserving pancreaticoduodenectomy for a patient with carcinoma of the papilla Vater two years after living donor liver transplantation. Hepatogastroenterology. 2007;54(75): 941-3.
14. Soejima Y, Ueda S, Sanefuji K, Kayashima H, Yoshizumi T, Ikegami T, et al. Sequential pancreaticoduodenectomy after living donor liver transplantation for cholangiocarcinoma. Am J Transplant. 2008; 8(10):2158-62.
15. Na BG, Hwang S, Kim SM, Yang G. Pancreaticoduodenectomy for de novo ampulla of Vater cancer 15 years after living donor liver transplantation: Report of a case. Annals of Liver Transplantation 2021(2):187-93.
16. Agha RA, Fowler AJ, Saeta A, Barai I, Rajmohan S, Orgill DP; SCARE Group. The SCARE statement: consensus-based surgical case report guidelines. Int J Surg. 2016;34:180-186.
17. Wahab MA, Shehta A, Elshoubary M, Yassen AM, Elmorshedi M, Salah T, et al. Living-donor liver transplantation in hepatitis C virus era: a report of 500 consecutive cases in a single center. Transplant Proc. 2018;50(5):1396-1406.
18. Kozuka S, Tsubone M, Yamaguchi A, Hachisuka K. Adenomatous residue in cancerous papilla of Vater. Gut. 1981;22(12):1031-4.
19. Rostain F, Hamza S, Drouillard A, Faivre J, Bouvier AM, Lepage C. Trends in incidence and management of cancer of the ampulla of Vater. World J Gastroenterol. 2014;20(29):10144-50.
20. Geissler EK. Post-transplantation malignancies: here today, gone tomorrow? Nat Rev Clin Oncol. 2015;12(12):705-17.
21. Fung JJ, Jain A, Kwak EJ, Kusne S, Dvorchik I, Eghtesad B. De novo malignancies after liver transplantation: a major cause of late death. Liver Transpl. 2001;7(11 Suppl 1):S109-18.
22. Yao FY, Gautam M, Palese C, Rebres R, Terrault N, Roberts JP, et al. De novo malignancies following liver transplantation: a caseecontrol study with long-term follow-up. Clin Transplant. 2006;20(5):617-23.
23. Sanchez EQ, Marubashi S, Jung G, Levy MF, Goldstein RM, Molmenti EP, et al. De novo tumors after liver transplantation: a single-institution experience. Liver Transpl. 2002; 8(3):285-91.
Full Text Sources:
Abstract:
Views: 1656

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.