Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
Parenchyma Sparing ALPPS - A New Technical Variant. Case Presentation (with video)
Associating liver partition and portal vein ligation (ALPPS) is nowadays an established surgical strategy for patients with liver tumors who are not amenable for upfront hepatectomy because of a too small future liver remnant (FLR) (1).
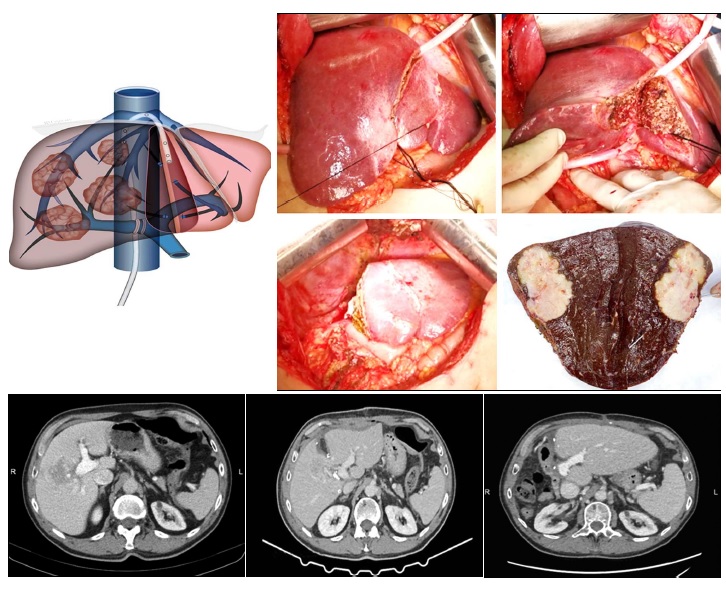
In these patients, we proposed a new technical variant of ALPPS, called parenchyma sparing ALPPS, consisting in shifting the transection plane though segment 4 (instead of the falciform ligament), thus increasing the FLR (2). The transection plane was established and performed under guidance of intraoperative ultrasound, ensuring oncological margins while maximizing the remnant liver volume.
Therefore, the main principles of our surgical strategy and technique were:
- Preserving the left part of S4; - Partial transection through S4 using IOUS guidance; - (Right) portal vein ligation with minimal hilum dissection; - Partial (right) liver venous deprivation - right accessory veins sectioned-ligated; - Longer interstage interval (2-3 weeks); - Extra-glissonian approach during staged 2.
The advantages are:
- Feasible even when ALPPS is not (S2-3 volume is <15%); - Safer than ALPPS: eliminates ischemia of segment 4, avoids biliary fistula due to segment 4 exclusion, and reduces the risk of liver failure due to small FLR.
We present the case of a 78-year-old male patient with significant comorbidities (atrial fibrillation, grade II hypertension, moderate pulmonary hypertension, compensated heart insufficiency, dyslipidemia), diagnosed at contrast MRI and CT with a tumor located in segments 5-8 liver lesion with extension to segments 6, 7, 4 and 1, in contact with the middle hepatic vein, enclosing the anterior right portal pedicle and in contact with the posterior right and the right portal pedicles (see video). The percutaneous tumor biopsy showed a moderate differentiated intrahepatic cholangiocarcinoma.
The patient required and extended right hepatectomy. However, the volumetry of segment 2 and 3 was insufficient even for a standard ALPPS, with parenchymal transection in the plane of the falciform ligament. Therefore, our new variant of ALPPS, parenchyma sparing ALPPS, was deployed, adding to the future remnant liver (FLR) part of segment 4 (see video). In this setting, the preoperative FLR was 24.8%, that increased to 34% during the interstage interval. No intraoperative adverse events were encountered during both operations. During the interstage interval of 15 days, there was a minor bleeding exteriorized through the drain placed on the cut surface, conservatively treated, requiring transfusion (1 unit). After the second stage, the postoperative course was uneventful, and the patient was discharged on the POD 8. The patient was alive and disease-free at 18 months.
In conclusion, parenchyma sparing ALPPS successfully combines two concepts of major liver surgery, regenerative and parenchyma-sparing liver surgery, and safely achieves resectability otherwise not be possible with any other technique.
Conflict of interest
The authors declare no conflicts of interests.
Ethical of approval
For this case ethical approval was obtained.
REFERENCES
1. Petrowsky H, Linecker M, Raptis DA, Kuemmerli C, Fritsch R, Kirimker OE, et al. First Long-term Oncologic Results of the ALPPS Procedure in a Large Cohort of Patients With Colorectal Liver Metastases. Ann Surg. 2020;272(5):793-800.
2. Botea F, Barcu A, Croitoru A, Tomescu D, Lupescu I, Dumitru R, et al. Parenchyma Sparing ALPPS - Ultrasound Guided Partition Through Segment 4 to Maximize Resectability (with video). Chirurgia (Bucur). 2022;117(1):81-93.
Full Text Sources:
Abstract:
Views: 2800

Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Dec 2025
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.